
Abstract
BACKGROUND AND PURPOSE: In carotid artery stent placement, marked oversizing of the stent relative to the internal carotid artery lumen is common. This study was performed to determine the influence of using oversized self-expanding nitinol stents on neointimal hyperplasia.
METHODS: In six greyhound dogs, 24 self-expanding nitinol stents (eight SMART stents, eight Easy Wallstents, eight Sinus-Flex stents) were inserted into both common carotid arteries (CCAs). In each CCA, two stents were deployed; a stent of the appropriate diameter was implanted distally and an oversized stent proximally. After 4 months, transverse sections of each stent were examined histologically and at computerized image analysis. Neointimal hyperplasia was determined as the proportion of the residual diameter of the patent vessel lumen compared with the stent lumen.
RESULTS: The amount of neointimal hyperplasia did not differ between the normal-sized and oversized stents. The mean preserved luminal diameter (± SEM) with normal- and oversized stents, respectively, were as follows: Easy Wallstent, 94% ± 1.0 and 96% ± 1.5; SMART stent, 92% ± 1.6 and 93% ± 1.8; and Sinus-Flex stent, 93% ± 2.7 and 93% ± 2.6. The mean preserved patent lumen with the 12 normal-sized stents (93% ± 1.0) was not significantly different from that of the 12 oversized stents (94% ± 1.1, P = .502).
CONCLUSION: Under experimental conditions, use of self-expanding stents oversized by 30–40% appeared to result in neointimal hyperplasia comparable to that caused by normal-sized stents. All three stent types appeared to have similarly low neointimal responses.
In the treatment of occlusive internal carotid artery (ICA) disease, stent placement has morbidity and mortality rates comparable to those of carotid endarterectomy (1). The long-term restenosis rate of carotid stent use is still unknown. Promising midterm follow-up restenosis rates of 4–4.9% in symptomatic ICA stenoses of 70% or greater have been published (2, 3). Self-expanding stents are now considered the devices of choice, because balloon-expandable stents have been associated with collapse of as much as 16% at follow-up (4, 5).
Typically, stents are placed in the ICA across the carotid bifurcation, because the disease usually involves both the common carotid arteries (CCAs) and the ICAs. Sizing the diameter of a self-expanding stent to the larger lumen of the CCA is necessary to ensure adequate apposition of the stent to the arterial wall and to cover the diseased vessel segment. The median diameter of the CCA in humans older than 50 years is 6.3 mm (range, 5.5–7.6 mm) in men and 5.5 mm (4.8–6.6 mm) in women (6). In practice, nominal stent diameters of 10 mm for most men and 8 mm for most women are used regularly; this practice leads to obvious oversizing of the stent relative to the lumen of the ICA (normal diameter, 4.93 mm ± 1.31), with a stent-to-ICA ratio of 1.5:2.0 (7).
This experimental study was conducted to define whether the higher radial force of the oversized self-expanding stent in the ICA is related to increased neointimal proliferation compared with that of a normal-sized stent.
Methods
Animals and Stents
The study was approved by the local animal ethics committee. All experiments were performed in accordance with the regulations for animal experiments.
The study was performed with six greyhound dogs (weight range, 23–31 kg; mean, 26.6 kg ± 3.2), and all interventions were performed with the animals under general anesthesia. From personal observation it was known that greyhound dogs have a long CCA (10–12 cm) with a constant diameter of 4–5 mm from the proximal end to the distal end. This fact was confirmed and measured on angiograms, with the outer diameter of the diagnostic angiography catheter used as a reference.
Two stents were inserted in each CCA, with a minimum of 4 cm separating each stent. The nominal normal-sized stent (diameter, 6 or 7 mm) was implanted distally, and the oversized stent (diameter, 10 mm), proximally (Fig 1A). The stents were matched for diameter and length as closely as possible and as limited by vendor specifications at the time of the study. A total of 24 self-expanding nitinol stents were implanted by using eight stents from three companies. The following stents and sizes (nominal stent diameter multiplied by length, maximally unrestrained) were used in the distal and proximal locations: 1) SMART stent (Cordis Endovascular, Miami, FL), 6 × 20 mm distal, 10 × 40 mm proximal (10 × 20-mm stent was not available at the time of the study); 2) Easy Wallstent (Schneider/Boston Scientific, Bülach, Switzerland), 6 × 20 mm distal, 10 × 20 mm proximal; and 3) Sinus-Flex stent (Optimed, Ettlingen, Germany), 7 × 40 mm distal 10 × 40 mm proximal (6 × 40-mm stent was not available at the time of the study).

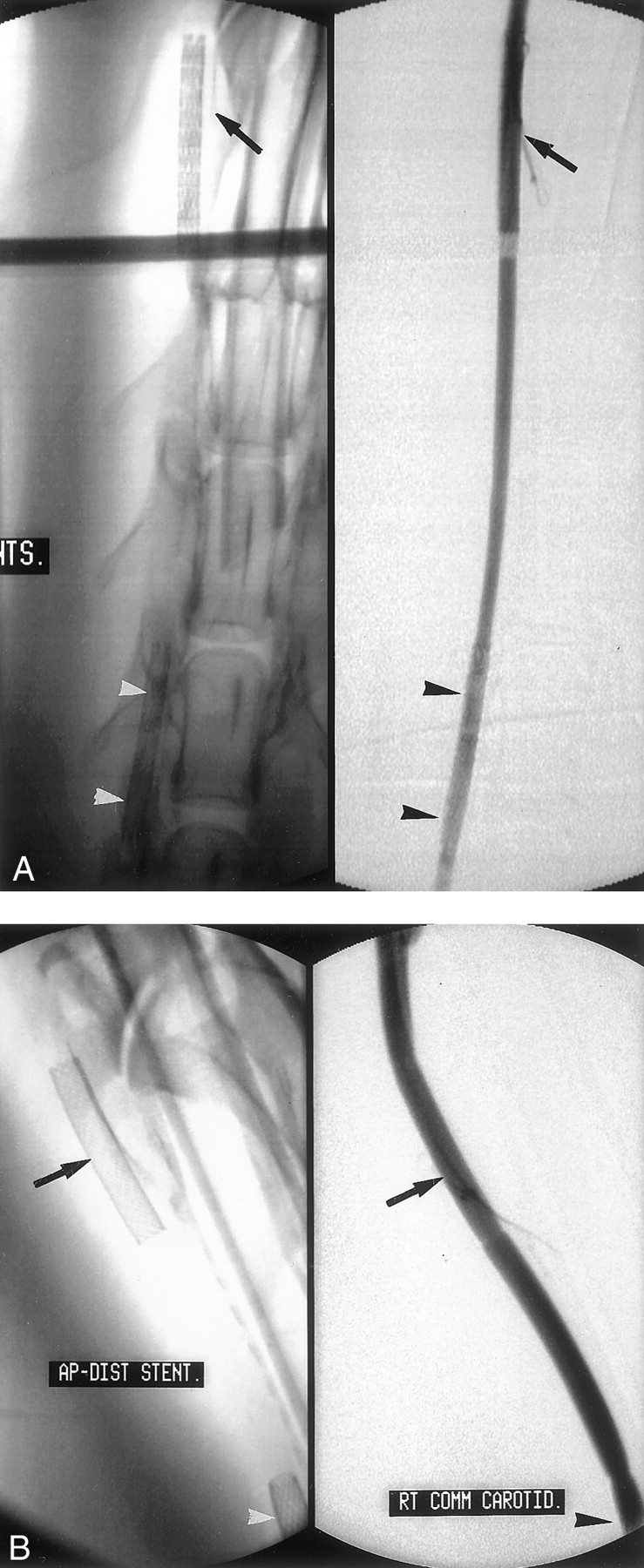
Unsubtracted (left) and subtracted (right) digital angiograms show the stents in the right CCA after implantation.
A, The normal-sized stent (6 mm) is implanted in the distal position (arrows); the oversized stent (10 mm), in the proximal position (arrowheads).
B, Control angiograms of a distally implanted stent obtained after 4 months show no obvious luminal narrowing (arrows). Note the partially depicted proximal stent (arrowheads) in these magnified views.
Surgical Procedure and Histologic Examination
For each dog, anesthesia was induced by means of IV administration of barbiturate (thiopentone 25 mg/kg; Abbott, Fronulla, Australia). After endotracheal intubation, anesthesia was maintained with a mixture of halothane, nitrous oxide, and oxygen. The animals were allowed to breathe spontaneously throughout the procedure. All procedures were performed under fluoroscopic guidance with a digital subtraction angiographic system (Philips Medical Applications, Sydney, Australia).
A 7F introducer sheath (Super Arrow-Flex; Arrow International, Reading, PA) was inserted after cutdown of the right femoral artery. The sheath was flushed continuously with a pressurized heparin and isotonic sodium chloride solution (5000 IU of heparin per L). Heparin was administered intraarterially as a 5000-U bolus after sheath insertion, with an additional 2500-U bolus administered before initial stent placement. A 5F catheter (Softouch; Mallinckrodt Medical, Angelton, TX) was placed in each CCA, and diagnostic cervical angiography was performed. An exchange was performed by using a 0.035-inch Amplatz heavy-duty guidewire (Cook, Brisbane, Australia), and the stents were implanted with road-map guidance. The distal stent was always placed first, so that passage through an already placed stent would not occur. After stent placement, a selective carotid angiogram was obtained to confirm patency. The sheath was removed, and the femoral artery ligated. After recovery, the dogs received daily acetylsalicylic acid (80 mg orally) for 4 weeks. No postoperative anticoagulation was used.
After 4 months, control angiography and stent harvesting were performed. Each animal underwent anesthesia, as just described. A 10F introducer sheath (Super Arrow-Flex) was inserted in the left common femoral artery, and a 7F sheath (Super Arrow-Flex), in the right common femoral vein. The animal received heparin, as previously described. Arch angiography (Royal Flush; Cook, Brisbane, Australia) and selective CCA angiography (Softouch; Mallinckrodt Medical) were performed proximal to the stents to document patent arteries and free flow. An angioplasty catheter (PE-MT 15 mm/2 cm; Medi-Tech/Boston Scientific, Watertown, MA) was placed in the superior vena cava through the 7F sheath and connected to a collecting system maintained under negative pressure. An occlusive balloon catheter (PE-MT 20 mm/3 cm; Medi-Tech/Boston Scientific) was then placed in the aortic arch through the 10F sheath distal to the origin of the left subclavian artery.
The animals then were sacrificed with an overdose of barbiturate. After inflation of the venous and thoracic aorta occlusive balloons, the supraaortic vessels were flushed continuously with a pressurized heparin and isotonic sodium chloride solution (0.9%, 5000 IU heparin per L) that was introduced through the lumen of the thoracic angioplasty balloon until relatively clear backflow from the venous drainage system was achieved. The supraaortic vessels were then pressure fixed in situ by means of infusion through the arterial side to achieve proper fixation of the vessels in their usual tone. The fixative, consisting of 10% formalin in 0.1 mol/L sodium phosphate buffer (pH 7.3) was infused for 30 minutes at a pressure of 120 mm Hg (8).
Both perfusion-fixed carotid arteries were removed en bloc and further fixed in the same solution for another 24 hours. The stent specimens were then dehydrated, cleared, and embedded in Araldite in a cylindrical mould with their long axis perpendicular to the cutting plane. Transverse sections (30–100 μm) were cut with a diamond wafering blade at three different levels (proximal, middle, distal) through each stent. The stent wires were left in situ in the sections to minimize potential artifact caused by removal of the stent wires. Sections were mounted on glass slides and stained with hematoxylin-eosin (Fig 2).

Light microscopic image of a representative transverse section (thickness, approximately 50 μm) through a stent shows a smooth and asymmetric, developed neointima in this CCA segment (arrowheads). Note that the stent wires were left in place (hematoxylin-eosin, original magnification ×10).
Morphometric Analysis, Definitions, and Statistical Analysis
Morphometric analysis of the sections was performed by using a Leica Orthoplan microscope with a camera (CCD; Minitron Enterprise). This was connected to an image analysis system (Quantimet 520; Leica, Cambridge, England).
To define the amount of neointimal hyperplasia, two cross-sectional areas were measured: the vessel lumen and the stent lumen. The cross-sectional area (inner diameter) enclosed by the endothelium of the patent vessel lumen defined the vessel lumen. The cross-sectional area (inner diameter) between the stent struts of the fixed and embedded stent specimen defined the stent lumen. Vessel and stent luminal areas (in mm2) were measured on three sections through each stent. Mean values for vessel and stent areas were then calculated for the three measured sections from the same stent-artery graft. This procedure was based on the assumption that, as the tissue was fixed at a normal perfusion pressure, the cross-sectional area is representative of a uniform circular profile. Finally, the amount of neointimal hyperplasia was determined as the proportion of the two cross-sectional areas, vessel lumen and stent lumen, with the area of the stent lumen being defined as 100%.
The nominal stent diameter was the maximally unrestrained diameter of a stent. The stent-to-artery ratio was the proportion of the stent diameter divided by the reference ICA diameter. An oversized stent had a high stent-to-artery ratio, which meant a high radial force. A nominal normal sized stent had a low stent-to-artery ratio, with a lower radial force on the vessel wall. The amount of neointimal hyperplasia was expressed in mm2 and as the percentage of preserved patent vessel lumen. All data are expressed as the mean ± SEM. To define the relationship between the vessel lumen and the stent lumen, the data were analyzed by using analysis of variance tests (ANOVAs), and a P value of .05 or less was considered to indicate a statistically significant difference.
Neither the manufacturer nor the stent type was identified for the observer (E.C.K.) in the quantitative histologic analysis. Specimen identity was not decoded until after the statistical analysis of the measurements had been performed. None of the authors have a financial interest or stock in any of the products mentioned. None of the sponsors were involved in the composition of this article.
Results
No complications were encountered with stent implantation. No dissection, early thrombus formation, or marked vasospasm was noted. No animal was lost in or around the 4-month follow-up period. At 4 months, all 24 stents remained widely patent at angiography (Fig 1B). On unsubtracted images, no migration or kinking of the stents was noted. No distinct difference in the amount of luminal narrowing could be detected at angiography when either stent types or diameters were considered.
The oversized stents had a stent-to-artery ratio of 2.0:2.5. A total of 66 sections from 24 stents were analyzed. Six sections had to be excluded, because they were damaged during the cutting process. On all sections, the stents were completely covered by endothelium after 4 months.
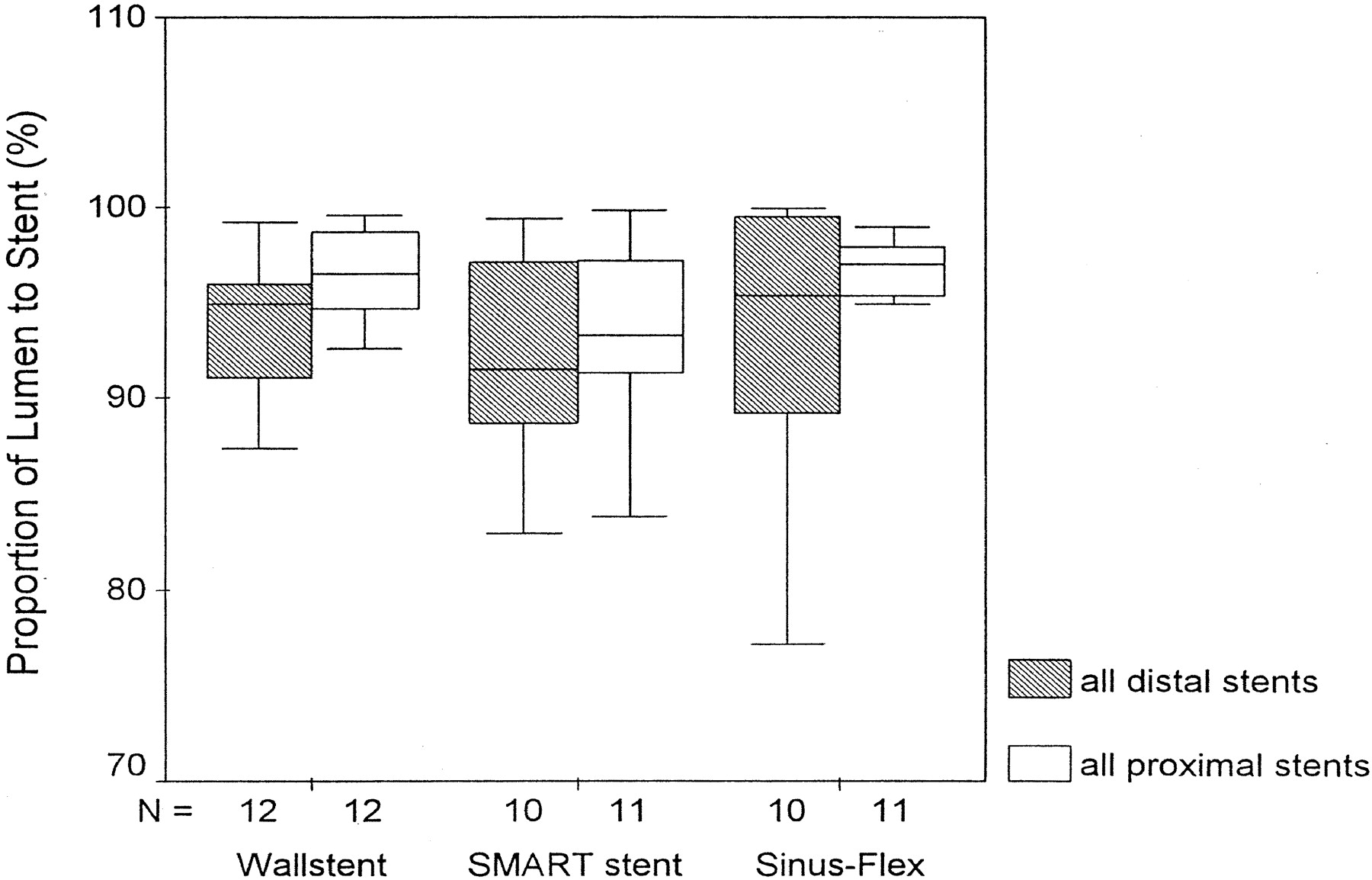
The amount of neointimal hyperplasia produced in each stent type demonstrated no differences with regard to the stent characteristics (ie, normal sized or oversized). The detailed results are listed in Table 1 and shown in Figure 3. The differences in neointimal hyperplasia produced by oversized and normal stent diameters were not statistically significant (Table 1).

Graph shows the amounts of neointimal hyperplasia with normal-sized (distal position; size, 6–7 mm) and oversized (proximal position; size, 10 mm) stents in the CCA. N indicates the number of sections.
Neointimal hyperplasia in normal- and oversized stents in the CCA at 4 months
Interestingly, all oversized stents had a statistically insignificant trend to produce less neointimal hyperplasia than that of the normal-sized stents (amounts with normal-sized and oversized stents, respectively: Easy Wallstent, 0.85 and 0.56 mm2; SMART stent, 1.64 and 1.46 mm2; and Sinus-Flex stent, 1.23 and 1.14 mm2).
The total amount of neointimal hyperplasia produced with each stent type, regardless of stent diameter, was assessed; findings revealed minor differences (Table 2). The Wallstent had the lowest total amount of neointimal hyperplasia (0.71 mm2), and the Sinus-Flex stent had a somewhat higher mean amount of neointimal hyperplasia (1.18 mm2), as did the SMART stent (1.64 mm2). These differences, however, were not statistically significant (P = .532).
Total amount of neointimal hyperplasia by stent type, not diameter
No significant difference existed when the neointimal hyperplasia produced by normal-sized stents were compared with that produced by oversized stents, regardless of vendor. The detailed results are listed in Table 3. The absolute amount of neointimal hyperplasia in all normal-sized stents was 1.22 mm2 compared with 1.14 mm2 in all oversized stents (Fig 4). Again, these differences were not statistically significant (P = .502).

Graph shows the mean neointimal thickness with the 24 stents, when normal-sized (distal position; size, 6–7 mm) and oversized (proximal position; size 10 mm) stents are compared. Data are a summary of that of all stent types studied. N indicates number of sections.
Mean neointimal thickness with the 24 CCA stents (summary data in stents of all vendors)
Discussion
Restenosis of a vessel segment with a stent is the main long-term complication of vascular stent placement. Because occlusive carotid artery disease normally involves the CCA and ICA, stents usually are placed over the bifurcation. Stent vendors recommend use of a self-expanding stent with a diameter that is 2 mm larger than that used for the normal vessel. This sizing ensures proper apposition of the stent to the arterial wall. When a stent is placed from the distal CCA across the carotid bifurcation to the proximal ICA, the stent diameter must be sized to the diameter of the CCA. This stent-sizing technique results in oversizing of the stent in relation to the diameter of the ICA, which can result in a higher residual radial force in the ICA wall relative to the forces exerted on the CCA wall by the stent.
Neointimal hyperplasia is the histopathologic correlate of in-stent restenosis (9). In experimental studies with stents implanted in animal (10) and human (11, 12) coronary arteries, investigators suggested that increased stretch in the inner layer of the vessel is associated with an increased response of neointimal hyperplasia. Additionally, localized inflammation could be a contributor to neointimal formation (13). As chronic stimuli to the vessel wall, permanent stent placement and stent oversizing were characterized as important stimulating factors of neointimal hyperplasia, because both increase the stretch forces on the vessel wall (10, 11, 14, 15).
In our experimental study, however, we found that the amount of neointimal hyperplasia was not correlated to stent oversizing or overstretching of the vessel wall. In our study, the stents were oversized by a factor of 2.0–2.5. At 4-month follow-up after stent implantation, no significant difference existed when the neointimal hyperplasia of the normal-sized nitinol stents and that of the oversized stents (regardless of vendor) were compared. All of the stents used, regardless of vendor and diameters, had differences in neointimal hyperplasia that were not statistically significant (P = .502).
Moreover, in our study, the oversized stents of all vendors, compared with the normal-sized stents, had a statistically insignificant trend toward less neointimal formation. The mechanisms of these findings remain unclear. In our study, we implanted two stents in the same vessel, with the stent edges separated by at least 4 cm, to minimize any stent interference. Little is known about the influence of two stents implanted in the same vessel with regard to patency, neointimal formation, and interference. Schürmann et al (16) found no significant difference in lumen and neointimal thicknesses when they compared single and tandem stents implanted in the iliac arteries of sheep. In their study, the stents were inserted at a distance of less than 10 mm of each other. They concluded that tandem stents did not adversely affect patency and neointimal hyperplasia when compared with a single contralateral stent, if a small distance is maintained. However, recent studies performed in vivo and in vitro have revealed that, soon after stent implantation, varying changes in pulsatile blood flow, arterial compliance, and arterial wall mechanics, as well as flow disturbances and pressure gradients were elicited (17, 18). The possibility that these hemodynamic and arterial wall changes, induced by the proximal larger stent, might have had an influence on the slightly pronounced development of neointimal hyperplasia in the nominally sized, distally implanted stents cannot be excluded.
Piamsomboon et al (7) had similar findings with stent placed in human carotid arteries. The authors used a quantitative analysis of 6-month angiograms in 63 carotid bifurcations obtained after stent placement. They found that the amount of neointimal hyperplasia in the groups with a high stent-to-artery ratio (oversized stent, ≥2.0) was significantly lower than that of the groups with a low stent-to-artery ratio of 1.4 (normal-sized stent). They concluded that the process of deploying oversized self-expanding stents in the ICA in humans does not appear to be associated with late restenosis. A high stent-to-artery ratio (oversized stent) seemed to be associated with an even lower amount of neointimal hyperplasia.
Using different vessels, Vorwerk et al (19) published similar results from an experimental study of self-expanding stents placed in the femoropopliteal arteries in dogs. They compared two types of stents with different radial forces and concluded that a reduced radial force did not result in a reduced neointimal formation. In this study, the two types of self-expanding Wallstents induced a comparable neointimal response of less than 100 μm. Therefore, in smaller arteries, the effect of neointimal response in lumen narrowing is more marked than that of larger arteries. Additionally, it seems that arteries in different anatomic locations react differently to stent insertions because of structural wall differences and hemorrheologic conditions (20).
Interestingly, similar experimental results were found in venous bypass grafts with stents. In a porcine model of arteriovenous bypass grafting, the use of an oversized, nonrestrictive, external Dacron velour stent to support the graft resulted in suppression of intimal and medial hyperplasia that was equal to that achieved with normal-sized stents (21).
In our study, the total amount of neointimal formation or lumen narrowing in all self-expanding stents was low. Similar results were found in other experimental studies (22, 23). Previous studies (20, 24) have shown that significant endothelial cell proliferation is known to occur when the internal elastic lamina is disrupted. This disruption may be caused by balloon angioplasty or even the persistent radial force of self-expanding stents. Our results indicated that a high radial force to the vessel wall, per se, is not associated with a high amount of neointimal hyperplasia. The use of oversized stents may even have a protective factor for restenosis, because these stents may lead to overdilatation of the arterial wall to more than twice its original diameter (23).
For our study, the canine model was selected for the following reasons: 1) From personal observations, the authors knew that greyhound dogs have a long CCA (10–12 cm). Therefore, two stents could be implanted in one vessel, with a good separation. 2) The vessel lumen width of the CCA is comparable to that of a human ICA, with a constant diameter of 4–5 mm from the proximal end to the distal end. 3) The neointimal hyperplasia in human beings and in commonly used animal models, such as those of pigs and dogs, have similarities. The number of cells, their composition, and the accompanying proteoglycan matrices essentially are the same (24). The reason to prefer the canine model was the differences in the vessel wall layers. The normal dog and pig coronary arteries, which were examined histologically, have a comparable intimal and medial layers. The major difference arises in the adventitia. Similar to those in humans, the canine coronary artery has a single layer of external elastic lamina, whereas in pigs, this structure is rich in elastic fibers and is several layers thick, with interspersed collagen, which normally leads to an exaggerated proliferative response (24, 25).
We performed autopsy after 4 months to achieve an adequate time to allow neointimal response. Smooth muscle cell proliferation, matrix formation, and inflammation are the major factors related to neointimal formation. In a proliferating (26) model of restenosis after coronary stent placement, the evolution of neointimal formation had maximal smooth muscle cell proliferation at 7 days, with a decline to low levels by 28 days. In another study with stent placement in porcine coronary arteries (27), mild inflammation was seen in the first 4 weeks and as long as 12 weeks after stent insertion.
Some limitations of this study have to be mentioned. First, because the study was performed in healthy animals with nonatherosclerotic arteries, the applicability of the experimental results to humans may be limited. Second, the stent sizes selected were appropriate to the diameter of the typical canine CCA. The stents of the three manufacturers had small differences in length and diameter. These were unavoidable, because we used the stents available from the vendors at the time of the study that matched most closely. Some variations in the data may have been due to these differences. Third, in this study, the stents were not subjected to balloon angioplasty, which may be an additional stimulating factor to neointimal hyperplasia after stent insertion.
Conclusion
These experimental study findings demonstrate that the use of oversized self-expanding stents in carotid arteries appears to be associated with a low rate of neointimal formation that is comparable to that associated with normal-sized stents.
Acknowledgments
The authors gratefully acknowledge the excellent laboratory work of Carina Forslund, the generously shared expertise of Wojciech Cwikiel, MD, both of whom are from the University of Lund, Sweden, and the precise statistical work from Andreas Schoetzau. The authors thank the staff of both the Interventional Radiology Department and the Research Centre for their invaluable assistance.
Footnotes
Supported by Boston Scientific, Botany, Australia; Cordis, North Ryde, Australia; and Optimed, Epping, Australia. E.C.K. was supported in part by the Swiss Society of Medical Radiology.
Presented in part at the RSNA 86th Annual Meeting and Scientific Assembly at Chicago, November 2000.
References
- Received April 17, 2001.
- Accepted after revision August 6, 2001.
- American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}