
Abstract
Summary: We describe a simple, inexpensive, and very effective method of achieving circumferential flow reduction during direct percutaneous cyanoacrylate embolization of a high-flow vascular malformation of the scalp. By using a plastic “cookie cutter” placed over the lesion and applying various degrees of pressure, both venous outflow from and arterial inflow into the lesion were limited. This flow reduction technique improved both the efficacy and safety of the procedure.
Direct percutaneous embolization is a well-established technique for the treatment of extracranial high-flow and low-flow vascular malformations. We looked for a suitable method of achieving circumferential flow reduction around a superficial high-flow vascular malformation of the scalp, not only to avoid inadvertent distal nontarget embolization, including possible occlusion of transorbital and intracranial venous drainage pathways, but also to trap the embolic material within the malformation, thereby improving the degree of penetration of the abnormal vascular channels within the lesion improving the efficacy of closure of the shunt.
Description of Technique
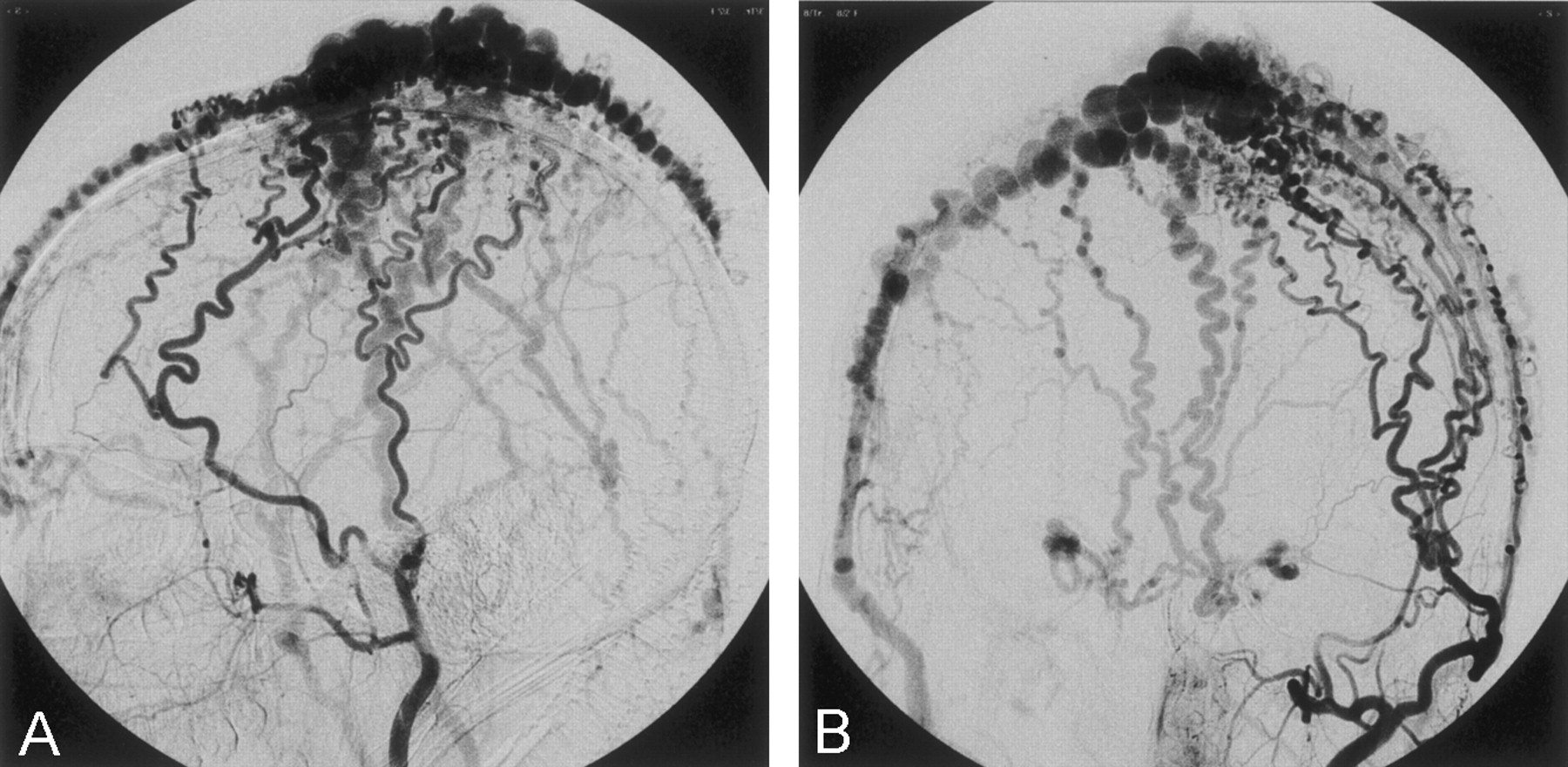
A 28-year-old female patient was referred to our unit for possible endovascular management of a large high-flow arteriovenous malformation (AVM) at the apex of the scalp. The lesion had ulcerated and hemorrhaged previously and was producing some local pain. The arterial supply to the lesion primarily involved branches of the two superficial temporal arteries with some supply from the occipital arteries and the ophthalmic arteries via their frontal or supratrochlear branches. All arteries fed into an elongated cirsoid collecting vessel, which in turn drained out through multiple superficial temporal and occipital scalp veins (Fig 1). Although no filling of the superior sagittal sinus was noted to indicate transcranial drainage through emissary veins, there was drainage anteromedially through supratrochlear veins into the superior orbital veins through to the anterior cavernous sinuses and then out through the pterygoid plexuses (Fig 2).

Composite arterial and venous phase arteriographic images of selective external carotid digital subtraction arteriograms, showing the extensive superficial temporal arterial supply, the site of the shunt, and the venous drainage.
A, Right external carotid artery, lateral projection.
B, Left external carotid artery, Towne’s projection.

Venous return phase image, selective left external carotid arteriogram, showing transorbital venous drainage.
Because of this drainage through the orbits, we initially debated the method of embolization and the embolic agent to be used. Two further significant factors considered were the extremely limited funds available for the procedure (being state sponsored) and risk that the patient may become lost to follow-up. We decided that the primary goal of treatment would be reduction of the shunt and prevention of rebleeding in the short term with initial embolization to be followed by either further intervention or surgery later, as required. We elected to use glue rather than alcohol or other sclerosant, because of better control of glue in a high-flow situation and the fact that the glue would be injected directly percutaneously into the large collecting vein without resorting to transarterial embolization to achieve some degree of initial flow reduction. The percutaneous procedure was performed under general anesthesia. A 5F Headhunter diagnostic catheter (William Cook Europe, Bjaeverskov, Denmark) was used to obtain initial diagnostic arteriograms of the internal and external carotid arteries and was then left in the proximal left external carotid artery to permit check arteriography during the embolization. To achieve circumferential flow reduction around the lesion, we used an oval-shaped “cookie cutter” held in place over the dilated collecting vein with three rubber bands. Initially, we had struggled to obtain a suitable plastic cookie cutter from the local baking stores, but a visit to a local toy store yielded a packet of suitable cutters of different shapes that are used as children’s modeling clay. Among the different shapes were circular and oval ones (Fig 3). They were sterilized before use.

Photograph showing the oval plastic cookie cutter held manually in place over the scalp malformation. This was fixed to the skull by means of three elastic bands during glue injections.
The lesion was punctured by using a 21-gauge butterfly needle. Contrast material injected though this needle showed no distal escape beyond the edge of the cookie cutter, indicating adequate venous compression. It was found that when more pressure was applied to the cookie cutter, the arterial inflow could also be reduced, thereby achieving complete flow reduction in the area within the cutter’s circumference. Unfortunately, this entailed some degree of irradiation of the operator’s hand while this additional compression was applied. Leaving the cookie cutter attached by the rubber bands, 4 mL of a 50% cyanoacrylate-Lipiodol mixture was injected into the collecting vein. The cookie cutter was left in situ for 2 minutes and then removed. Slight escape of some glue into one of the anterior scalp draining veins beyond the cookie cutter occurred during the first injection as a result of slipping of one of the securing rubber bands (Fig 4). No further escape of glue from the collecting vein was noted before or after removal of the cutter and needle. Check arteriography showed some residual shunt filling anterior to the area injected initially, which included the drainage through the orbit and cavernous sinus. The cookie cutter was replaced in a more anterior position around the persistent shunt, and the bands were reapplied. A second butterfly needle was placed into the patent collecting vein, and check venography again confirmed no contrast material reflux beyond the cutter. Two milliliters of a 50% glue mixture were then injected into this anterior part of the collecting vein again, with no escape of glue during the injection or after removal of the cutter. A third injection was made in a similar manner, followed by a fourth limited to a small area of residual shunt to the left of the embolized collecting vein, which was injected with 3% sodium tetradecyl sulfate solution (Fibro-Vein 3%, STD Pharmaceutical Products, Hereford, England) instead of glue. Final control digital subtraction angiography of the external carotid arteries showed occlusion of most of the malformation with only small areas of residual shunt seen at the periphery of the lesion (Fig 5). Having achieved the goal of significant shunt reduction and protection against future hemorrhage from the ulcerated area, we stopped the procedure at this stage. The patient was awakened from the anesthesia and experienced a mild initial localized headache easily managed with an oral nonsteroidal anti-inflammatory drug for 12 hours. She has since been discharged after the procedure pending further angiographic follow-up and possible repeat intervention or follow-up surgery.

Lateral nonsubtracted digital skull radiograph showing the opaque glue cast contained within the area demarcated by the cookie cutter (arrow). Some initial escape of glue under the edge of the cookie cutter is seen, because of slipping of one of the retaining elastic bands during the glue injection. No further inadvertent glue loss was seen.

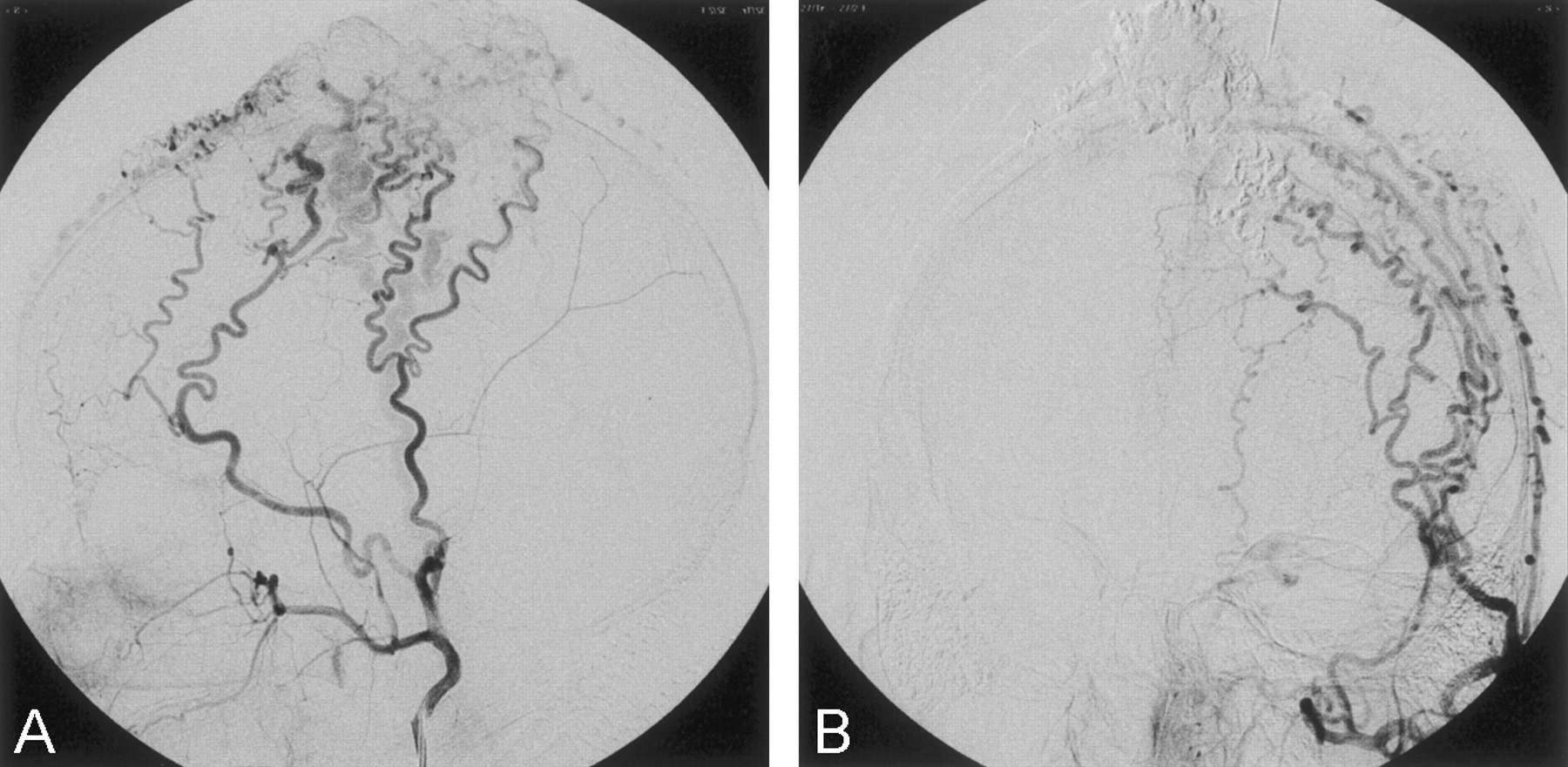
Composite arterial and venous phase arteriographic images following completion of the embolization, showing very little residual shunt surgery related to the otherwise extensively embolized scalp malformation.
A, Right external carotid artery, lateral projection
B, Left external carotid artery, Towne’s projection.
Discussion
One of the great dangers with the endovascular treatment of any high-flow arteriovenous shunt is inadvertent loss of the embolic material through to the venous side of the shunt and possibly even into the pulmonary circulation (1) (2–4). In our experience of more than 120 cerebral and head and neck AVMs treated with cyanoacrylate, to date we have had one death, probably attributable to excessive penetration of glue through the nidus of a cerebral arteriovenous malformation and closure of a vein probably partly draining from another area of nonembolized nidus. This patient had a massive intracerebral hemorrhage 48 hours after the embolization procedure. We have had three cases of transient symptomatic pulmonary embolism after closure of three high-flow shunts (one after cerebral AVM embolization, one after coronary artery fistula closure, and one after endoscopic variceal glue injection). A more recent case involving a superficial temporal arteriovenous fistula involved inadvertent loss of glue into the external jugular vein with some transient localized neck pain.
Flow reduction during embolization is desirable for two main reasons. First, reduction of afferent flow in a high-flow situation allows a more controlled delivery of an embolic agent to the target site with less risk of distal embolization into the veins. This flow reduction can be achieved by partial occlusion within a vessel, compression outside of the vessel, or a reduction in blood pressure. Second, flow reduction or, more often, flow arrest allows certain embolic agents such as glue, alcohol, or other sclerosing agents to remain in contact with the target area for a longer period, thereby achieving a better occlusive result. Prime examples of the latter technique would include endovascular renal ablation with absolute alcohol (5) and varicose vein ablation with compression sclerotherpy (6). The problem with many vascular malformations, whether low flow or high flow, is that they often drain centrifugally in several different directions from the shunt or nidus and manual external flow arrest is often difficult to achieve.
We have shown that a suitable cylindrical device placed around the shunt or nidus can be made to produce flow arrest within the draining veins and supplying arteries, depending upon the amount of pressure applied to the device. Compression of veins proved easy by simply applying rubber bands, but arterial occlusion necessitated more forceful pressure application by hand, resulting in irradiation of the operator’s hand during fluoroscopy and check arteriography. Having demonstrated the potential value of this technique, we intend to have the oval and round cookie cutters fixed to a perspex bar in order that pressure can be applied without unnecessary operator exposure to the x-ray beam. Cutters or similar devices not only of different shapes, but also of different diameters could be used, depending on the size of the target to be embolized. By the ability to trap the embolic agent within an area, this technique will also allow better penetration of the fistula or nidus by the embolic agent to achieve a more complete degree of target vessel obliteration. When using alcohol or other sclerosing agents, these liquids can be drained or aspirated from the lesion before release of pressure and restoration of flow in and around the lesion with less fear of distal venous phlebitis or occlusion. Great care must be taken to ensure that no liquid embolic agent would be forced intracranially through emissary veins or other collateral pathways lying within the circumference of the device.
Conclusion
We foresee a use for this simple flow reduction technique for suitable superficial high-flow and low-flow vascular malformations, increasing both the safety and efficacy of direct percutaneous embolization procedures employed in the management of these abnormalities.
- Received February 4, 2003.
- Accepted after revision February 16, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.