
Article Figures & Data
Figures
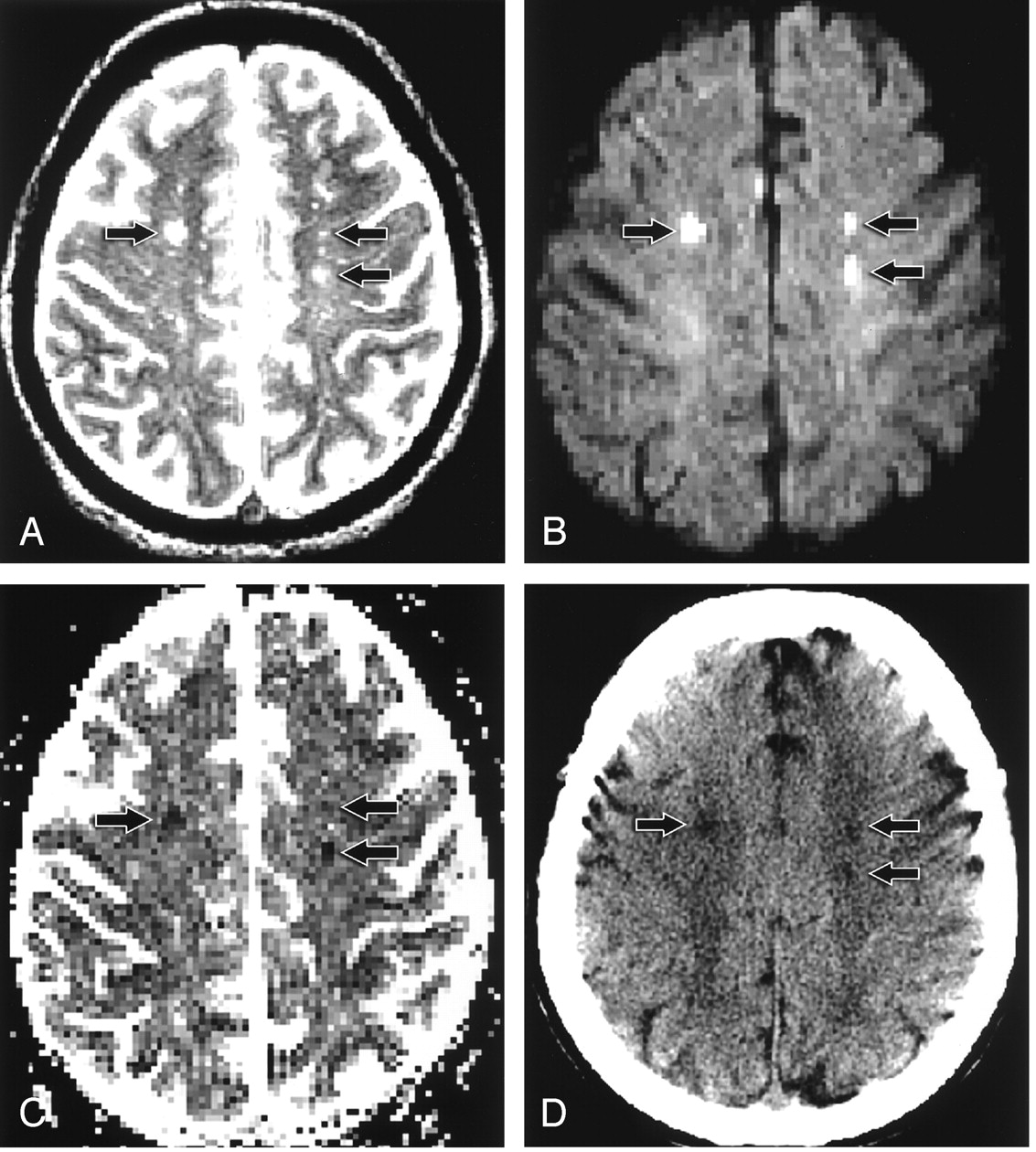
- Fig 1.
Patient 12. A 43-year-old woman with headache, blurred vision, and mental status change.
A, T2-weighted axial MR image shows bilateral centrum semiovale hyperintense foci (arrows).
B, On axial echo-planar DW image, the lesions (arrows) are hyperintense.
C, On axial ADC map, the lesions (arrows) are hypointense.
D, Follow-up axial CT scan shows low-attenuation foci (arrows), corresponding to the abnormalities on initial MR images, that are consistent with infarct.
- Fig 2.
Patient 9. A 31-year-old man with mental status changes and seizure activity.
A, T2-weighted axial MR image shows bilateral frontal and right parietal hyperintense foci (arrows).
B, On axial DW image, the lesions (arrows) are hyperintense.
C, On axial ADC map, the lesions (arrows) are hypointense.
D, Follow-up T2-weighted axial MR image shows no abnormality in the bilateral frontal and right parietal regions (arrows), consistent with interval resolution of the previous abnormalities.
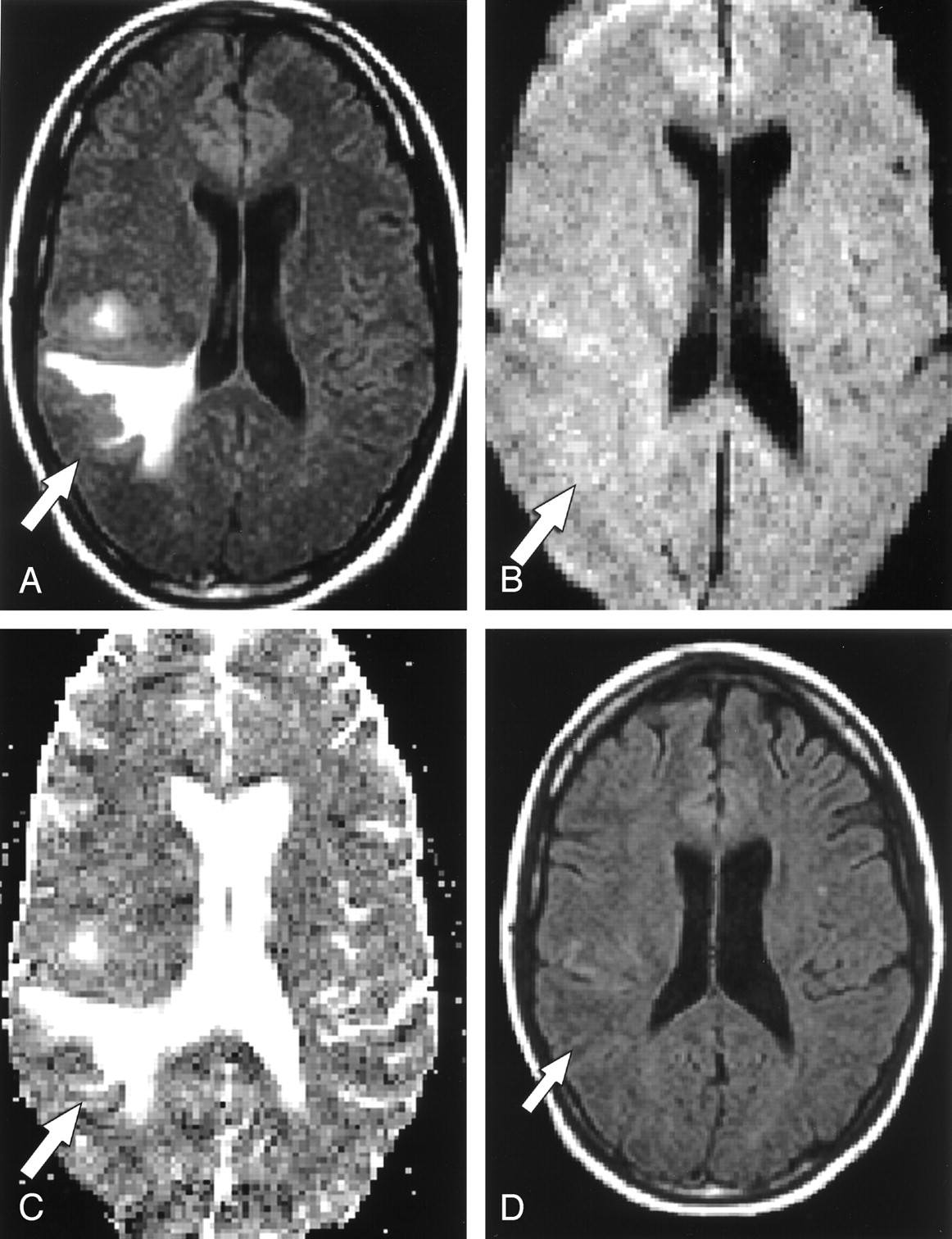
- Fig 3.
Patient 4. A 25-year-old woman with headache and left-sided weakness.
A, FLAIR axial MR image shows a right parietal T2 hyperintense focus (arrow).
B, On axial echo-planar DW image, the lesion (arrow) is slightly hyperintense.
C, On axial ADC map, the lesion (arrow) is hyperintense.
D, Follow-up FLAIR axial MR image shows no abnormality, consistent with interval resolution of the previous abnormality.
- Fig 4.
Patient 5. A 24-year-old woman with headache and left-sided sensory loss.
A, T2-weighted axial MR image shows central (arrowhead) and peripheral (arrow) right thalamic T2 hyperintense foci.
B, On axil echo-planar DW image, the central lesion (arrowhead) is hyperintense and the peripheral lesion is isointense (arrow).
C, On axial ADC map, the lesions are hypointense (arrowhead) and hyperintense (arrow), respectively.
D, Follow-up CT scan shows central right thalamic infarct (arrowhead) and no abnormality in the peripheral region (arrow).




Tables
Patient No./Age/Sex Initial Symptoms Venous Sinuses Intravenous Therapy CVT Cause Status at Discharge Seizure 1/71/F Unresponsive. Superior sagittal, L transverse. Heparin Unknown Died No 2/34/F Headache, confusion, R upper extremity weakness, behavior change, fatigue, somnolence. Superior sagittal. Heparin Lupus, vitamin B12 deficiency Normal Yes 3/39/M L Hemiplegia, headache, nausea. Superior sagittal, B transverse, R straight, R cortical. Heparin, urokinase Unknown Slight L facial droop, upper extremity weakness, pronator drift. Yes 4/25/F Headache, L upper extremity weakness. Superior sagittal, R transverse. Heparin Oral contraceptives Improved headache, weakness resolved. No 5/24/F Headache. Superior sagittal, B deep. Heparin Unknown Unknown No 6/30/F Headache, L hand weakness, memory and speech difficulties. Superior sagittal straight, R transverse, R internal cerebral. Urokinase, heparin Metastatic choriocarcinoma Resolved Yes 7/52/F Headache, L hand and facial weakness, speech difficulties. Superior sagittal, R sigmoid, R transverse, R jugular vein. Heparin Unknown Resolved No 8/49/M Headache, nausea, disorientation, speech difficulties, urinary incontinence. R transverse, R sigmoid, R straight, R internal cerebral, VOG. Heparin Factor V Leiden Speech difficulties and disorientation improved, remaining symptoms resolved. No 9/31/M Seizure, headache, L weakness. Superior sagittal, R transverse. Urokinase, Heparin Dehydration, TB mastoiditis L weakness improved, headache resolved. Yes 10/17/F Headache, fatigue, nausea, confusion, L hemiparesis. Inferior sagittal, B straight, B deep. Heparin Dehydration, oral contraceptives L weakness improved, other symptoms resolved. No 11/67/M Headache, speech and vision difficulties. Superior sagittal, R transverse. Heparin, Lovenox (SC) Dehydration L field cut persisted, other symptoms resolved. No 12/43/F Headache, visual difficulties, decreased mental acuity, vague paresthesias. Superior sagittal, R straight, R transverse, R jugular vein. Heparin Hyperviscosity Died No 13/41/M L arm numbness and weakness. R cortical veins. Heparin Unknown Weakness improved. No Note.—B indicates bilateral; L, left; R, right; SC, subcutaneous; TB, tuberculosis; VOG, vein of Galen.
Patient No. Lesion Locations Anatomic Involvement T2WI DWI ADC ADC Mean (×10−3 mm2/s) Follow-up MR or CT Hemorrhage Follow-up Sinus Patency 1 1. B occipital G/W Hyperintense Hyperintense Hypointense Not done Not done No Not done 2. Cerebellum G/W Hyperintense Hyperintense Hypointense Not done 3. B frontal G/W Hyperintense Hyperintense Hypointense Not done 4. B parietal G/W Hyperintense Hyperintense Hypointense Not done 2 1. L frontal G/W Hyperintense Hyperintense Hypointense 0.54306 Resolution (MR) No No change 2. R frontal G/W Hyperintense Hyperintense Hypointense 0.55513 Resolution (MR) 3 1. R parietal (central) G/W Hypointense Hypointense (susceptibility) Hypointense (hemorrhage) Not done Hemorrhage (MR) Yes No change 2. R parietal (peripheral) G/W Hyperintense Isointense Hyperintense 1.6038 Resolution (MR) 4 1. R frontal (central) G/W Hypointense Hypointense (susceptibility) Hypointense (hemorrhage) Not done Hemorrhage (MR) Yes Recanalized 2. R frontal (peripheral) G/W Hyperintense Hyperintense Hyperintense 1.0605 Resolution (MR) 3. R parietal G/W Hyperintense Isotense Hyperintense 1.5659 Resolution (MR) 5 1. R thalamus (central) DG Hyperintense Hyperintense Hypointense 0.43744 Infraction (CT) No Recanalized 2. R. thalamus (peripheral) DG Hyperintense Iso/Hyperintense Hyperintense 1.075 Resolution (CT) 6 1. R thalamus DG Hyperintense Hyperintense Isotense Hypointense (central) 0.45055 Infarction (MR) No Recanalized 2. R thalamus DG Hyperintense Hyperintense 1.204 Resolution (MR) 3. R putamen DG Hyperintense Hyperintense Hyperintense (peripheral) 0.41378 Resolution (MR) 4. L thalamus DG Hyperintense Hyperintense 0.47527 Resolution (MR) 5. L frontal G/W Hyperintense Hyperintense Hypointense 0.42851 Resolution (MR) 6. L caudate DG Hyperintense Hyperintense Hypointense 0.44393 Resolution (MR) 7. L putamen DG Hyperintense Hypointense 0.39336 Resolution (MR) 7 R parietal G/W Hyperintense Hyperintense Hyperintense Not done Resolution (MR) No Recanalized 8 1. R thalamus (central) DG Hypointense (hemorrhage) Hypointense (susceptibility) Hypointense Not done Hemorrhage (MR) Yes Recanalized 2. R thalamus (peripheral) DG Hyperintense (edema) Hyperintense Hyperintense 1.0134 Resolution (MR) 3. L thalamus DG Hyperintense Hyperintense Hyperintense 0.89987 Resolution (MR) 4. R corona radiata W Hyperintense Hyperintense Hyperintense 0.88926 Resolution (MR) 9 1. R frontal G/W Hyperintense Hyperintense Hypointense 0.2545 Resolution (MR) No Recanalized 2. L frontal G/W Hyperintense Hyperintense Hypointense 0.15438 Resolution (MR) 3. L parietal W Hyperintense Hyperintense Hypointense 0.25045 Resolution (MR) 10 1. R thalamus (central) DG Hyperintense Hyperintense Hypointense Not done Hemorrhage (MR) Resolution (MR) Yes No change 2. R thalamus (peripheral) DG Hyperintense Iso/hyperintense Hyperintense Not done Infarction (MR) 3. L thalamus DG Hyperintense Hyperintense Hypointense Not done 11 1. R centrum W Hyperintense Hyperintense Hypointense Not done Not done No Not done 2. R temporal G/W Hyperintense Isotense Hyperintense Not done 3. R occipital G/W Hyperintense Isotense Hyperintense Not done 12 R centrum G/W Hyperintense Hyperintense Hypointense 0.56893 Infarction (MR) No No change L centrum G/W Hyperintense Hyperintense Hypointense 0.54106 Infarction (MR) 13 L frontal G/W Hyperintense Hyperintense Hypointense Not done Not done No Not done Note.—B indicates bilateral; CT, nonenhanced CT with CT venography; DG, deep gray; DWI, diffusion-weighted imaging; G, gray matter; G/W, gray and white matter; L, left; MR, MR imaging; R, right; T2WI, T2-weighted imaging; W, white matter.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular treatment for cerebral venous thrombosis: current status, challenges, and opportunities
- Current endovascular strategies for cerebral venous thrombosis: report of the SNIS Standards and Guidelines Committee
- Imaging Characteristics of Venous Parenchymal Abnormalities
- Transient Global Amnesia, Cerebral Veins, and the Need to Find the 'Smoking Gun'
- Diagnosis and Management of Cerebral Venous Thrombosis: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association
- Compromise of Brain Tissue Caused by Cortical Venous Reflux of Intracranial Dural Arteriovenous Fistulas: Assessment With Diffusion-Weighted Magnetic Resonance Imaging
- Neonatal Cerebral Sinovenous Thrombosis From Symptom to Outcome
- MR Imaging Features of Isolated Cortical Vein Thrombosis: Diagnosis and Follow-Up
- Are Steroids Useful to Treat Cerebral Venous Thrombosis?