
Article Figures & Data
Figures
- Fig 1.
A, Time course of the signal intensity from 1 section of a multisection gradient-echo EPI dataset at 1.5T during gadopentetate dimeglumine passage, TR/TE = 1,125/49 ms. During the first pass, signal intensity decreases due to the microscopic field-strength variations and water diffusion through gradients created by the intravascular contrast agent. B, Signal intensity versus time for regions of interest in the gray and white matter. C, From these curves and an estimate of the AIF, maps of perfusion-weighted parameters such as CBV, CBF, MTT, and Tmax can be created. Note the prolonged MTT and Tmax in the left hemisphere, representing ischemic tissue within the left middle cerebral artery territory. Sec indicates seconds; au, arbitrary units. Image courtesy of Dr. Rexford Newbould, Stanford University.
- Fig 2.
Effects of bolus widening (“dispersion”) in the AIF on the tissue-concentration-versus-time curve. A, Residue function, which represents the probability of the tracer remaining in the voxel at time t. Note that this is a monotonically decreasing function, with a value of 1 at time t = 0. The residue function shown here represents a well-mixed single compartment with an MTT of 4 seconds, similar to that seen in brain. For the remainder of the examples, CBF is taken to be 50 mL/100 mL of brain per minute, again typical for brain. The area under the AIF is normalized to 1 arbitrary unit. B, Tissue concentration curve (solid line) for a “perfect bolus” AIF (dotted line), which arrives at t = 0. The tissue concentration curve is just the residue function multiplied by CBF. Note that CBF is equal to the first point of the tissue concentration curve, which is also the peak concentration. C, AIF is a 2-second bolus top hat function corresponding to “plug flow”: note the increase in the arrival time of peak contrast and the decrease in peak concentration, a consequence of the convolution of the AIF and the residue function. No longer is CBF equal to the first time point of the tissue curve or the peak concentration. D, AIF is a gaussian curve with full width at half maximum of 2 seconds, a more realistic model of a bolus that has widened before reaching the tissue. Note that for both C and D, deconvolution techniques are necessary to determine CBF and that the first moment of the tissue concentration curve is not equal to the MTT. Sec indicates seconds.
- Fig 3.
In ASL, upstream blood protons are either unperturbed (control) or inverted (label) on alternate applications of the pulse sequence, here demonstrated by the up arrows and down arrows, respectively. The signal intensity of the labeled images is approximately 1–2% lower than that of the control images due to the extraction of the negatively magnetized inverted spins into the tissue when they reach the capillary bed. Subtracting label images from control images creates a difference image proportional to CBF. Typically many such image pairs must be subtracted to achieve adequate SNR; the image of CBF in a healthy volunteer shown above was acquired in 5 minutes at 3T.
- Fig 4.
CBF errors due to prolonged arrival time in ischemic stroke with ASL. A, A contrast-enhanced MR angiogram shows right internal carotid artery occlusion. B, Diffusion-weighted image demonstrates abnormality of the right putamen, caudate, and a small area in the right frontal operculum. C, A PASL image of CBF demonstrates punctate high signal intensity (arrows) surrounding an area of apparent low flow in the right parietal lobe. The high signal intensity is probably due to delayed arrival of the label via collateral flow which is still within large vessels rather than in the parenchyma. The low measured CBF centrally is due to decay of the label before it enters the tissue. Normal flow was seen in this region on Xe-CT (images not shown). D, Follow-up CT 2 days later demonstrates infarction of the right caudate and putamen (arrow) but preserved gray-white contrast in the right parietal region that demonstrates low signal intensity on the ASL CBF map. CBF underestimation in the setting of collateral flow is a fundamental difficulty with the use of standard ASL in this patient population.
- Fig 5.
A basic model of the imaging voxel for permeability studies. The plasma volume, vp, is small compared with the EES (shown in gray) and the intracellular space, from which contrast is excluded. Observed relaxivity changes are a weighted average of the plasma and EES contrast concentration. The large black arrows signify isodirectional flux of contrast between these 2 spaces, with a rate constant equal to Ktrans. This flux is essentially zero in the presence of an intact BBB but is nonzero in many pathophysiologic conditions.
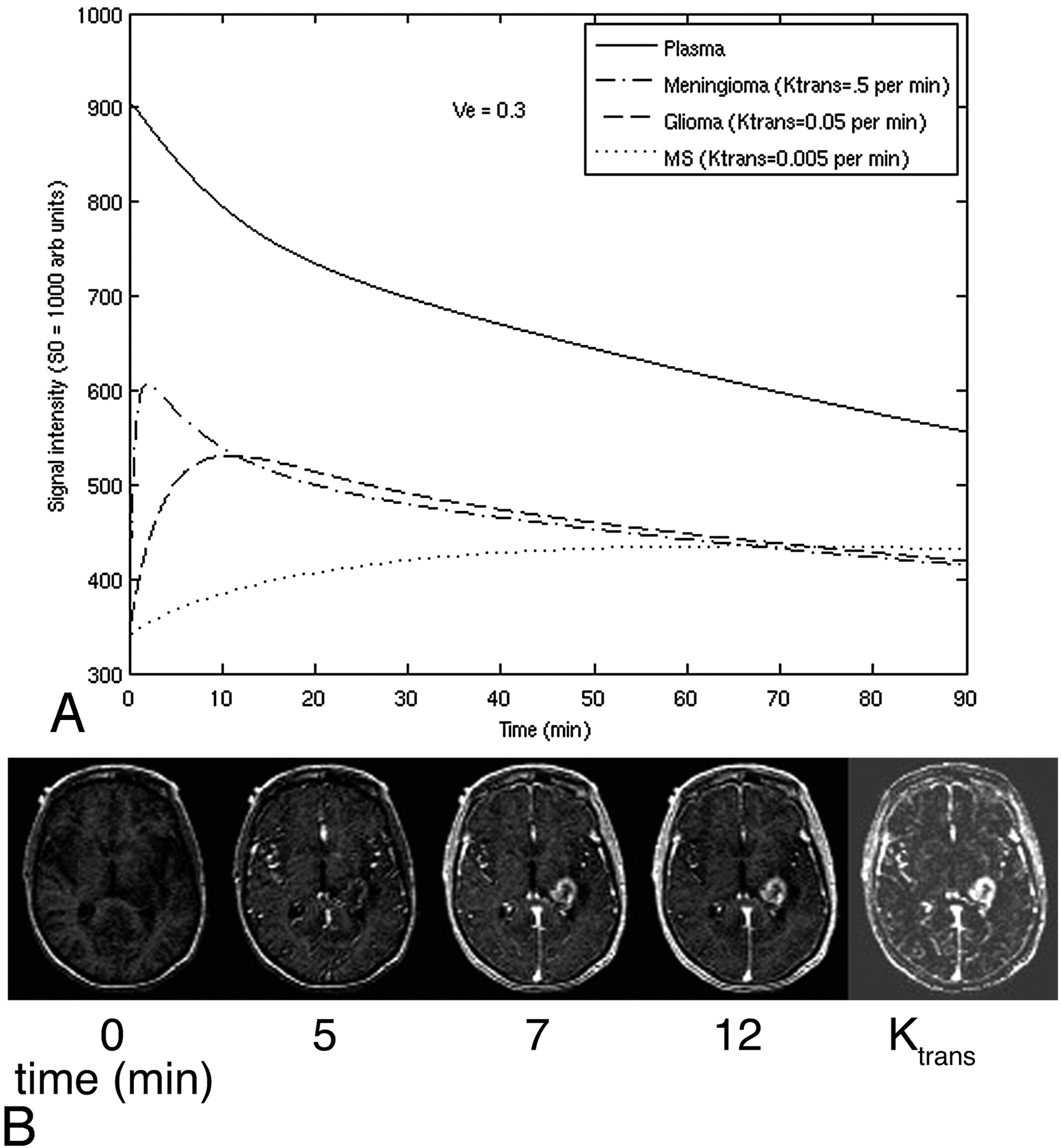
- Fig 6.
A, Simulated signal-intensity enhancement curve versus time by using the steady-state T1 method for tissue with different permeability, corresponding to a meningioma (Ktrans = 0.5/min), a glioma (Ktrans = 0.05/min), and a chronic multiple sclerosis (MS) lesion (Ktrans = 0.005/min). ve of 0.3 is assumed. Proton density is assumed to be 1,000 arbitrary units (au) for all tissue, T1 before contrast is 1.2 seconds, and a typical spin-echo T1-weighted sequence with a TR of 500 ms is assumed. Note the rapid rise and subsequent fall of signal intensity in the highly leaky meningioma compared with the more gradual onset of contrast enhancement in the MS lesion. As is typical for the ssT1 method, contribution from the intravascular space is neglected. B, An example of gradual enhancement on T1-weighted imaging in a high-grade glioma at several time points following contrast administration by using the ssT1 method. The fitted Ktrans permeability map is shown at the right. Image courtesy of Dr. Soonmee Cha, University of California, San Francisco.






In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MTT and Blood-Brain Barrier Disruption within Asymptomatic Vascular WM Lesions
- Clinical Value of Vascular Permeability Estimates Using Dynamic Susceptibility Contrast MRI: Improved Diagnostic Performance in Distinguishing Hypervascular Primary CNS Lymphoma from Glioblastoma
- Pretreatment blood-brain barrier disruption and post-endovascular intracranial hemorrhage
- White Matter Ischemic Changes in Hyperacute Ischemic Stroke: Voxel-Based Analysis Using Diffusion Tensor Imaging and MR Perfusion
- Advanced Magnetic Resonance Imaging of the Physical Processes in Human Glioblastoma
- Pretreatment Blood-Brain Barrier Damage and Post-Treatment Intracranial Hemorrhage in Patients Receiving Intravenous Tissue-Type Plasminogen Activator
- Assessment of Angiographic Vascularity of Meningiomas with Dynamic Susceptibility Contrast-Enhanced Perfusion-Weighted Imaging and Diffusion Tensor Imaging
- Differentiation of Primary Central Nervous System Lymphomas and Glioblastomas: Comparisons of Diagnostic Performance of Dynamic Susceptibility Contrast-Enhanced Perfusion MR Imaging without and with Contrast-Leakage Correction
- In Vivo Imaging of Neurovascular Remodeling After Stroke
- Quantitative Blood Flow Measurements in Gliomas Using Arterial Spin-Labeling at 3T: Intermodality Agreement and Inter- and Intraobserver Reproducibility Study