
Abstract
SUMMARY: Glioneuronal tumors are characterized exclusively by neurocytic elements (neuronal tumors) or a combination of neuronal and glial features (mixed neuronal-glial tumors). Most of these tumors occur in young patients and are related to epilepsy. While ganglioglioma, dysembryoplastic neuroepithelial tumor, and desmoplastic infantile tumor are common glioneuronal tumors, anaplastic ganglioglioma, papillary glioneuronal tumor, rosette-forming glioneuronal tumor, gangliocytoma, and central neurocytoma are less frequent. Advances in immunohistochemical and molecular diagnostics have improved the characterization of these tumors and favored the description of variants and new subtypes, some not yet classified by the World Health Organization. Not infrequently, the histologic findings of biopsies of glioneuronal tumors simulate low-grade glial neoplasms; however, some imaging findings favor the correct diagnosis, making neuroimaging essential for proper management. Therefore, the aim of this review was to present key imaging, histopathology, immunohistochemistry, and molecular findings of glioneuronal tumors and their variants.
ABBREVIATIONS:
- DNET
- dysembryoplastic neuroepithelial tumor
- GFAP
- glial fibrillary acidic protein
- MAP
- microtubule-associated protein
- rCBV
- relative CBV
- WHO
- World Health Organization
Neuronal and mixed neuronal-glial tumors (generically called glioneuronal tumors) are a heterogeneous group of lesions exhibiting different degrees of biologic behavior.1 Neuronal tumors are composed exclusively of ganglionic elements, and neuronal-glial tumors contain a combination of neuronal and glial features.1⇓⇓⇓-5 Glioneuronal tumors usually affect children and young adults with a predilection for the temporal lobe and frequently result in epilepsy, and most are cured with surgery.2,4 Some types present peculiar imaging findings that aid preoperative diagnosis and distinction from more common glial tumors, such as calcification, blood by-products, and absent perilesional edema or mass effect.2,3
Low-grade gliomas and glioneuronal tumors may present overlapping histologic findings; however, advances in immunohistochemical and molecular techniques have favored the distinction between these entities and led to the emergence of new subtypes of glioneuronal tumors.1,4,6 In the latest update of the CNS tumor classification, the World Health Organization (WHO) added multinodular and vacuolating neuronal tumor, myxoid glioneuronal tumor, and diffuse glioneuronal tumor with oligodendroglioma-like features and nuclear clusters to the glioneuronal tumors category (the latter provisionally, for lack of published characterizations; it is, therefore, not addressed in this review).6,7
The most common glioneuronal tumors of the brain are ganglioglioma, dysembryoplastic neuroepithelial tumor (DNET), and desmoplastic infantile tumor (they represent up to 2% of the CNS tumors).3,4,8 Conversely, anaplastic ganglioglioma, papillary glioneuronal tumor, rosette-forming glioneuronal tumor, gangliocytoma, and central neurocytoma are uncommon glioneuronal tumors whose incidence is still unknown.3,4,8 In general, glioneuronal tumors are low-grade lesions, with rare or absent mitotic figures and a low MIB1 labeling index (except in anaplastic subtypes).4 Immunohistochemistry may reveal glial elements by glial fibrillary acidic protein (GFAP) positivity; neuronal elements, by synaptophysin immunoreactivity; and glioneuronal progenitor cells, by CD34 positivity.4 Although some of these tumors are well-described, others have not been widely demonstrated. Therefore, this review discusses key MR imaging and pathologic findings of uncommon mixed neuronal-glial and neuronal tumors. Additionally, a table comparing the imaging aspects of different glioneuronal tumors is presented in the Online Supplemental Data. A flow chart presenting a simple diagnostic approach to suspected glioneuronal and low-grade glial tumors is available in Fig 1, and, finally, a brief discussion on imaging findings of the differential diagnosis of uncommon glioneuronal tumors can be found at the end of the article.

Diagnostic approach for glioneuronal and low-grade glial tumors with cystic components (high-grade glial neoplasms were not considered for the creation of this flow chart). Predominantly cystic tumors (A), cystic with mural nodule (B), and mixed solid and cystic tumors (C) are presented. PLNTY indicates polymorphous low‐grade neuroepithelial tumor of the young; mI, myo-inositol.
Anaplastic Ganglioglioma
Epidemiology.
Anaplastic ganglioglioma is a rare neuronal-glial tumor, defined as a grade III by the 2016 WHO Classification of Tumors of the CNS.1,3,5,8 It accounts for 6%–10% of all gangliogliomas, and it is still unclear whether it occurs through anaplastic transformation or is induced by radiation therapy, which may occur, on average, after 1 year and usually within 10 years of treatment.1,3,5 It mostly affects children and young adults, with no predilection for sex.1
Clinical Presentation.
The presentation is seizures, focal neurologic deficits, and increased intracranial pressure.3,5
Imaging Findings.
Imaging findings are a mixed solid and cystic lesion, mass effect, and perilesional edema (Fig 2).5 The solid component presents hypointense signal on T1-weighted images, hyperintense signal on T2-weighted images, calcification, diffusion restriction, high Cho peak, an increased lactate-lipid peak, increased perfusion (relative CBV [rCBV] > 1.75), and heterogeneous enhancement.1,5,9,10 Comparison of imaging aspects of different glioneuronal tumors is presented in the Online Supplemental Data.

An anaplastic ganglioglioma in a 15-year-old boy with treated cerebellar meduloblastoma 10 years ago. An infiltrative parieto-occipital mass lesion with heterogeneous enhancement and vasogenic edema, both extending to the contralateral hemisphere through the splenium of the corpus callosum. Also note blood by-products (C and D). Immunohistochemistry was positive for GFAP, p53, synaptophysin, and an MIB1 labeling index of 80% (not shown). Axial T2-weighted image (A). Axial T1-weighted fat-saturated contrast-enhanced image (B). Axial gradient-echo T2*-weighted image (C). Axial CT image (D).
Pathology Findings.
The pathology findings are dysplastic neuronal cells with an anaplastic glial component and increased cellularity, cellular pleomorphism, and vascular proliferation.3⇓-5 Mitoses are frequent, necrotic foci may be present, and the MIB1 labeling index is generally high.4 Immunohistochemistry depicts glial cells positive for GFAP, neurons positive for synaptophysin, and cells positive for CD34.4 Molecular study may identify BRAF V600E and H3 histone mutation.1,3
Papillary Glioneuronal Tumor
Epidemiology.
The papillary glioneuronal tumor is a WHO grade I, rare, neuronal-glial tumor and comprises 0.02% of all CNS tumors.4,8 It occurs in young adults, typically in the second decade, with no predilection for sex.3⇓-5
Location.
The location is deep periventricular white matter, adjacent to the lateral ventricles, in the frontal (40% of cases), temporal (30%), or parietal (30%) lobes.3,5,11,12
Imaging Findings.
The most common presentation is a well-circumscribed cyst, with an avid, enhancing wall or mural nodule; however, the morphology may vary from a purely cystic lesion to a completely solid mass (Fig 3).3⇓-5,11 The cystic component may be suppressed on FLAIR, and the solid component presents with hypo- to isointense signal on T1-weighted imaging, iso- to hyperintense signal on T2-weighted imaging, no diffusion restriction, an increased Cho/creatine ratio, and a low rCBV.5,13 Superficial siderosis, hemosiderin, and calcification may be present, mass effect is mild, and mild perilesional edema is rare.4,5,11,14

Papillary glioneuronal tumor in a 45-year-old man with migraine. A mixed solid and cystic periventricular tumor associated with vasogenic edema, blood products, and localized superficial siderosis. Microscopic findings are pseudopapillary structures composed of hyalinized vessels (long arrow) and surrounded by flattened/cuboidal glial cells. Round cells between pseudopapillae correspond to neurocytic cells (short arrow). Axial T2-weighted image (A). Axial T1-weighted fat-saturated contrast-enhanced image (B). Axial gradient-echo T2*-weighted image (C). Hematoxylin and eosin, original magnification ×100 (D).
Pathology Findings.
Pathologic findings are flat or cuboid glial cells (astrocytes and oligodendrocyte-like cells) in a pseudopapillary arrangement with interpapillary collections of neuronal elements (ganglioid, ganglion, or neurocytes).3⇓-5,11 Immunohistochemistry depicts GFAP; S-100 and nestin-positive glial cells lining hyalinized vascular pseudopapillae; synaptophysin, neuron-specific enolase, and neuronal nuclear protein–positive interpapillary neuronal cells; and OLIG2-positive oligodendrocyte-like cells.3,4,11,15 Molecular assessment may demonstrate t(9;17)(q(31;q24) translocation, resulting in the SLC44A1-PRKCA oncogene.4,15
Differential Diagnosis.
The differential diagnosis is gangliogliomas, polymorphous low‐grade neuroepithelial tumor of the young, pleomorphic xanthoastrocytoma, angiocentric glioma, and oligodendrocytoma.3
Treatment.
The treatment is an operation, and prognosis is good after complete resection.4
Rosette-Forming Glioneuronal Tumor
Epidemiology.
The rosette-forming glioneuronal tumor is a WHO grade I, rare, neuronal-glial tumor.3,4,8,18 It occurs in children and in young and middle-aged adults, with no predilection for sex.3⇓-5,18,19
Location.
The location is medial and infratentorial, often in the fourth ventricle/cerebellar vermis, secondarily in the pineal region, and rarely at the septum pellucidum, hypothalamus, and temporal lobe.1,3⇓-5,18⇓-20
Clinical Presentation.
The clinical presentation is headache, vomiting, visual disturbances, vertigo, ataxia, intracranial hypertension, and, rarely, epilepsy.1,3,5,19
Imaging Findings.
The imaging findings are a heterogeneous, circumscribed multicystic intra-axial mass with hypointense signal on T1-weighted imaging, hyperintense signal on T2-weighted imaging, hemorrhage, fluid levels, no diffusion restriction, mild Cho peak elevation, mild NAA peak reduction, an absent or rare lactate doublet, and septal and parietal wall enhancement (may resemble a green bell pepper cross-section) (Fig 4).3,5,19,21,22 Calcification (25% of cases), CSF dissemination, and multiple satellite lesions may occasionally appear.3,21

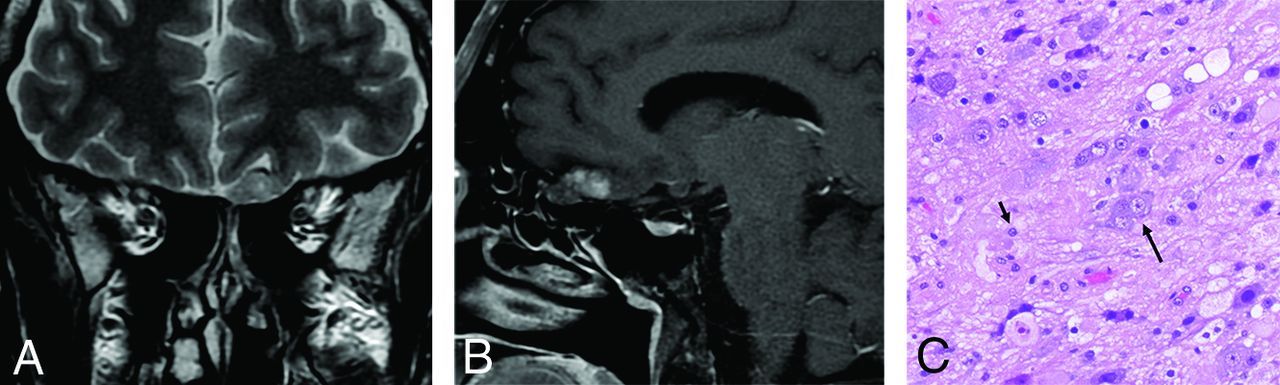
Rosette-forming glioneuronal tumor. A lobulated multicystic tumor in the tectal plate extending to the mesencephalic aqueduct, with nodular contrast enhancement (short arrow) and displacement of a supracerebellar vein (long arrow) (A and B). Microscopic findings are small, round cells (neurocytic cells) (short arrow) surrounding mucinous extracellular matrix (DNET-like morphology) (long arrow). Sagittal T2-weighted CISS image (A). Sagittal T1-weighted fat-saturated contrast-enhanced image (B). Hematoxylin and eosin, original magnification ×100 (C).
Pathology Findings.
Uniform neurocyte-forming rosettes or perivascular pseudorosettes and astrocytic elements (similar to pilocytic astrocytoma or oligodendroglioma).1,3⇓-5,18 Immunohistochemistry shows synaptophysin, MAP2, and neuron-specific enolase positive neuronal cells; and GFAP, OLIG2 and S-100 positive glial cells.4,18 Molecular studies may demonstrate PIK3CA, KIAA1549-BRAF, FGFR1, and NF1 variations.1,4,18,20
Myxoid Glioneuronal Tumor
Epidemiology.
Myxoid glioneuronal tumor is a low-grade tumor with components resembling rosette-forming glioneuronal tumor and DNET.7,23⇓-25 As of the 2021 WHO classification, it is considered a different glioneuronal type.7,23⇓-25 It occurs in children and young adults, with no predilection for sex.24,25
Clinical Presentation.
The clinical presentation is asymptomatic, cognitive disturbance, or headache.23,25
Imaging Findings.
Imaging findings are a solid tumor, with hypointense signal on T1WI, hyperintense signal on T2WI, partial suppression and a peripheral rim of hyperintensity on FLAIR, no gadolinium enhancement, and mucin-filled small pseudocysts and a slight hypointense signal on susceptibility-weighted images (corresponds to hemosiderin-laden macrophages).23⇓-25
Pathology Findings.
Pathology findings are proliferation of oligodendrocyte-like cells with a columnar arrangement in a mucin-rich stroma, which may be associated with “floating” neurons, neurocytic rosettes, and perivascular neuropil.7,23⇓-25 Immunohistochemistry shows a pattern similar to that of rosette-forming glioneuronal tumor and DNET; however, the molecular profile lacks the typical variations of these tumors and presents as a PDGFRA p.K385L/I mutation.7,23⇓-25
Diffuse Leptomeningeal Glioneuronal Tumor
Epidemiology.
Diffuse leptomeningeal glioneuronal tumor is a WHO grade I, rare, neuronal-glial tumor (previously known as disseminated oligodendroglial-like leptomeningeal tumor of childhood).3,5,8,26 It occurs in children and adolescents, with a predilection for males.4,5,26
Clinical Presentation.
It presents as headache, nausea, vomiting, cranial nerve dysfunction, papilledema, and CSF abnormalities, including increased protein and lymphocytosis.3,5,26
Imaging Findings.
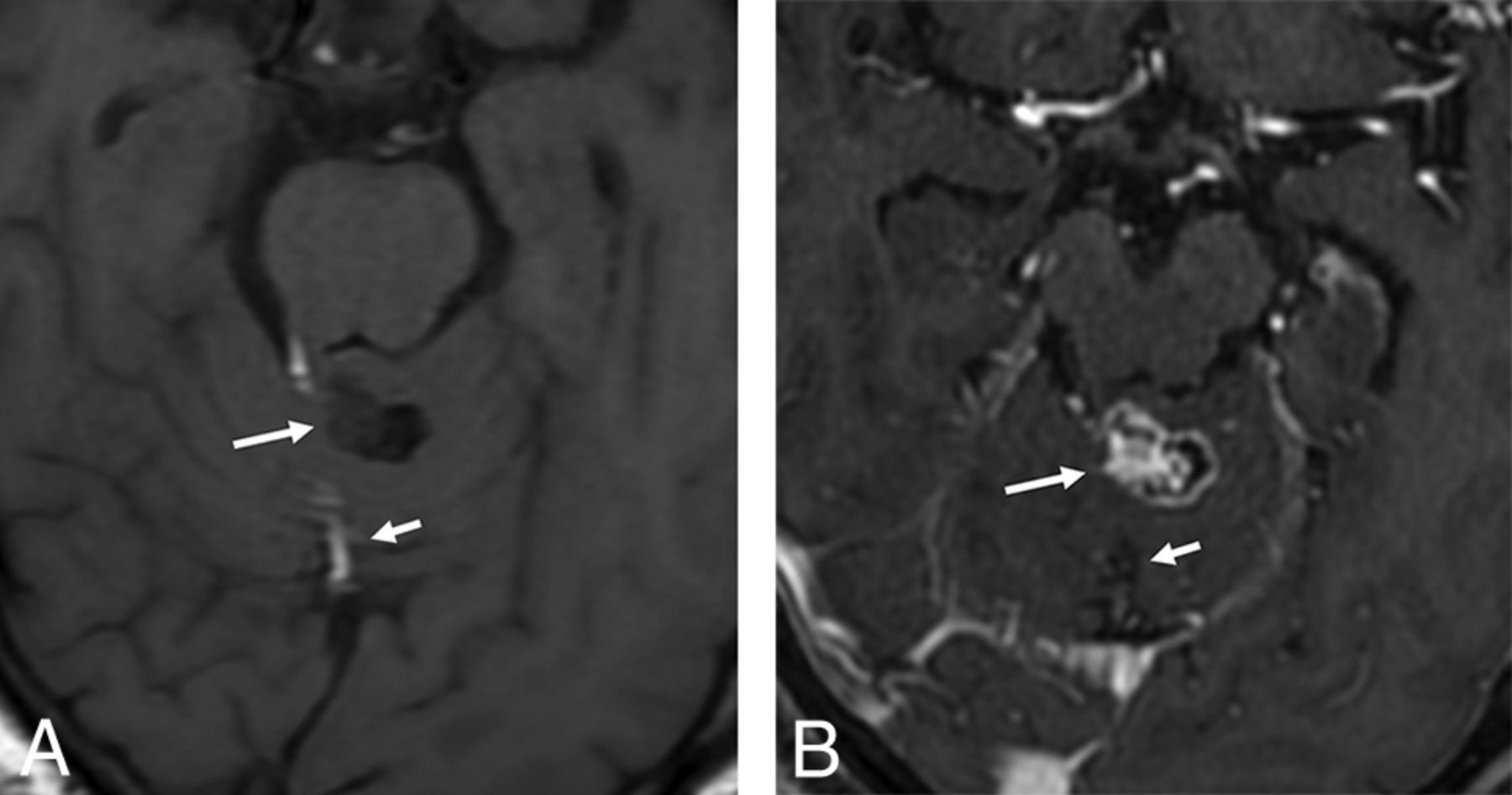
The imaging findings are widespread leptomeningeal thickening and intra-axial lesions.1,3,5,26⇓⇓-29 The leptomeningeal disease involves mostly the posterior fossa, spinal cord, nerve roots, and perivascular spaces and is characterized by leptomeningeal thickening and enhancement and leptomeningeal cystlike lesions (corresponding to mucin-rich nodular leptomeningeal infiltration) with hypointense signal on T1-weighted imaging, hyperintense signal on T2-weighted imaging and FLAIR, and no contrast enhancement (Fig 5).1,3,5,26⇓⇓-29 Intra-axial lesions are present in up to 80% of patients; they occur mostly in the spinal cord and present with hyperintense signal on T2-weighted imaging, cystic areas (corresponding to fluid and cellular debris), reduced rCBV, and usually no enhancement.1,5,26,27,29 Hydrocephalus is common, and a large intramedullary mass without leptomeningeal disease may also occur.3,26,29,30 Despite the description of intra-axial lesions, it is not clear whether they really are primary intraparenchymal lesions or the result of invasion of leptomeningeal lesions along Virchow-Robin spaces.28

Diffuse leptomeningeal glioneuronal tumor in a 20-year-old man previously diagnosed 10 years earlier. Multiple superficial small cystlike lesions are seen in the brain sulci, basal cisterns, cerebellar folia, and filling the fourth ventricle (A and B). Also note extensive irregular leptomeningeal enhancement (C). Axial T2-weighted images (A and B). Axial T1-weighted fat-saturated contrast-enhanced image (C).
Pathology Findings.
The pathology findings are diffuse and multifocal leptomeningeal lesions with an oligodendroglial-like cytology in a desmoplastic or myxoid background.1,3,6,27,28 Immunohistochemistry shows OLIG2-, S-10-0-, MAP2-positive oligodendroglial-like cells; astrocytes positive for GFAP; and neuron cells positive for synaptophysin.1,3,4,26⇓-28 Molecular profiling may identify KIAA1549-BRAF fusion, BRAF duplication, the BRAF V600E mutation, 1p/19q codeletion or isolated 1p deletion, and no IDH mutation.1,3,4,6,26⇓-28,30 Diagnosis may be particularly difficult when the biopsy shows only hyperplastic meningothelial cells, inflammation, or low-grade glioma (in these cases, rebiopsy is recommended).28,31
Differential Diagnosis.
Other causes of leptomeningeal thickening, such as infectious meningitis, neurocysticercosis, primary diffuse leptomeningeal gliomatosis, leptomeningeal carcinomatosis, leukemia, and lymphoma leptomeningeal infiltration.3,26
Gangliocytoma
Epidemiology.
Gangliocytoma is a WHO grade I, rare, neuronal tumor.4,8 It occurs in children and young adults, with no predilection for sex.3,4 Most articles address gangliocytomas (a purely neuronal tumor) in conjunction with gangliogliomas (a neuronal-glial tumor), and research focused specifically on the former is rare.32
Location.
These are located in the periphery of the temporal (75% of cases), frontal, or parietal lobes; they are occasionally exophytic and rarely extra-axial.2⇓-4,33
Imaging Findings.
The imaging findings are a mixed, solid, and cystic lesion with iso- to hypointense signal on T1-weighted imaging, hyperintense signal in T2-weighted imaging, a high Cho peak, a low NAA peak, variable contrast enhancement (from none-to-intense), and calcification (33% of cases) of the solid component (Fig 6).2⇓-4,34 Mass effect and perilesional edema are minimal or absent.4 A dural tail signal may be seen in superficially located tumors.2

Gangliocytoma in a 40-year-old man with epilepsy. A lobulated tumor extending along the course of the left olfactory bulb and tract with foci of contrast enhancement (A and B). Microscopic findings are tumor composed of large (long arrow) and small (short arrow) ganglioneuronal cells, haphazardly distributed. Coronal T2-weighted image (A). Sagittal T1-weighted fat-saturated contrast-enhanced image (B). Hematoxylin and eosin, original magnification ×100 (C).
Pathology Findings.
The pathology findings are clusters of mature and often dysplastic (binucleated) neurons and nonneoplastic glial stroma, unlike gangliogliomas.2,3 Perivascular lymphocytic infiltration is common, and mitotic figures are rare.3,4 Immunohistochemistry may demonstrate cells positive for CD3.3 To date, there are no genetic variations specifically described for gangliocytomas.3
Differential Diagnosis.
The differential diagnosis is ganglioglioma (imaging may be indistinguishable), DNET, and pleomorphic xanthoastrocytoma.2⇓-4
Variant.
Lhermitte-Duclos disease or dysplastic cerebellar gangliocytoma may be considered a subtype of gangliocytoma; however, it is still unclear whether it is a true neoplasm, hamartoma, or malformation.3,5 It is considered a WHO grade I tumor and may be sporadic (60% of cases) or related to Cowden syndrome (multiple hamartoma autosomal-dominant phacomatosis caused by PTEN mutations).3⇓-5,35 Young adults are mainly affected, with no predilection for sex.2⇓⇓-5,35 It usually is located in the cerebellar hemisphere, vermis, or both (particularly on the left side).2,3,5 Imaging findings are quite characteristic: nonenhancing grossly thickened cerebellar folia with the “tiger-striped” pattern (alternating layers of signal intensity on T1-weighted and T2-weighted imaging) and prominent venous channels (flow voids on susceptibility imaging with contrast enhancement) (Fig 7).2⇓⇓-5,35 Histopathology depicts disruption of the normal cortical layers, dysplastic neurons, vacuoles, diffuse hypertrophy and increased myelination of the granular and molecular layers, and reduction or absence of the Purkinje layer.2,3,5 Immunohistochemistry demonstrates dysplastic neurons positive for synaptophysin and negative for PTEN.4 Molecular assessment may show a PTEN germline mutation when related to Cowden syndrome.3,4,35

Dysplastic gangliocytoma of the cerebellum in a 19-year-old man with Cowden syndrome. Grossly thickened cerebellar folia with a tiger-striped pattern and rare patchy enhancement in the superior vermis and left cerebellar hemisphere. Axial T2-weighted image (A). Axial T1-weighted fat-saturated contrast-enhanced image (B).
Multinodular and Vacuolating Neuronal Tumor
Epidemiology.
Multinodular and vacuolating neuronal tumor is a rare lesion recently categorized as a glioneuronal tumor in the 6th edition of the WHO Classification (in the previous edition, it was considered a unique architectural pattern, whose nature may be related to neuronal tumors or malformative abnormalities).3,5,7,8,36 Identification of clonal genetic abnormalities favors a neoplastic rather than a malformative origin, hence, the status update in the WHO classification.6,7 It occurs in adults older than 30 years of age, with no predilection for sex.5,36
Location.
The location is the superficial parietal, frontal, or temporal lobe and, rarely, in the posterior fossa.4⇓-6,36⇓-38
Imaging Findings.
Imaging findings are multiple, small, and coalescent cortical and subcortical nodules, isointense to gray matter on T1-weighted imaging, hyperintense on T2-weighted imaging and FLAIR, with no mass effect, perilesional edema, calcification, diffusion restriction, and contrast enhancement (though faint enhancement may occasionally be present) (Fig 8).3,5,36,38 Spectroscopy and perfusion are usually normal.3⇓-5,36,38

Multinodular and vacuolating neuronal tumor of the cerebrum in a 33-year-old asymptomatic woman. Confluent, small, round lesions in a subcortical location with hypersignal in a T2-weighted FLAIR image (A). They clearly show different signal from the adjacent CSF in a T2-weighted FIESTA image, differentiating them from perivascular spaces (B).
Pathology Findings.
Pathology findings are ambiguous neuronal cells or dysplastic glial cells with cytoplasmic and stromal vacuolation.3⇓-5,36 Immunohistochemistry demonstrates HuC/HuD neuronal antigens, OLIG2, and cells positive for internexin-a and cells weakly positive or negative for synaptophysin and neurofilament.3,36 Molecular studies may identify MAP2K1, FGFR2, and non-BRAF V600E variations.6,39
Central Neurocytoma
Epidemiology.
Central neurocytoma is a WHO grade I, rare, neuronal tumor.1,3,5,8 It occurs in young and middle-aged adults, with no predilection for sex.1,3,5
Clinical Presentation.
It presents with headache, mental status change, visual disturbance, and intracranial hypertension.1,3,5
Imaging Presentation.
The presentation is an intraventricular, heterogeneous, and “bubbly” mixed, solid and cystic lesion, with a solid component presenting heterogeneous signal, isointense to gray matter on T1-weighted imaging, hyperintense on FLAIR, with flow voids, calcification (50% of cases) with hemorrhage, diffusion restriction, a decreased NAA peak, a moderately elevated Cho peak, and the presence of glycine and alanine peaks, increased rCBV, and moderate-to-intense enhancement (Fig 9).1⇓-3,5,19

Central neurocytoma. An intraventricular bubbly lesion adjacent to the septum showing honeycombing contrast enhancement and extensive signs of calcification and hemorrhage (A–C). Microscopic findings are sheets of round cells with scant cytoplasm. Neurocytic rosettes are present (arrows). Axial T2-weighted image (A). Axial T1-weighted fat-saturated contrast-enhanced image (B). Axial gradient-echo T2*-weighted image (C). Hematoxylin and eosin, original magnification ×200 (D).
Pathology Findings.
It presents with uniform, mature, neurocytic elements arranged in sheets or lobules.1,3 Immunohistochemistry identifies cells positive for synaptophysin and neuron-specific enolase and cells negative for OLIG2.2,3 Molecular profiling depicts N-MYC, IGF2, PTEN, PDGFD, and NRG2, WNT, 1p/19q, and Tp53 variations.1,4
Differential Diagnosis.
The differential diagnosis is subependymoma, ependymoma, subependimal giant cell astrocytoma, meningioma, and intraventricular oligodendroglioma.2,3
Treatment.
The treatment is an operation and adjuvant radiation therapy if there is subtotal resection or a high MIB1 labeling index.1,3 The prognosis is usually favorable, though rare recurrence may occur, especially if increased mitoses or MIB1 labeling index higher than 2% is observed.1⇓⇓-4
Variants.
Variants are extraventricular and cerebellar liponeurocytoma. Extraventricular neurocytoma is histologically similar to central neurocytoma, except for necrosis, vascular proliferation, and increased mitoses.1,3⇓-5,40 It is located outside the ventricular system, usually in the cerebral hemispheres, and imaging depicts hemorrhage, perilesional edema, and a low or absent NAA peak.1,3⇓-5,40 Cerebellar liponeurocytoma is composed of neurocytic elements and lipomalike features, usually with a low MIB1 labeling index.1,3⇓-5,40 Imaging may depict fat areas on T1-weighted images, confirmed with fat-suppression, chemical shift imaging, or a prominent lipid peak (Fig 10).1,3⇓-5,40

Cerebellar liponeurocytoma in a 71-year-old woman with transient neurologic deficits. A heterogeneously enhancing nodule (long arrow) in the superior vermis associated with a linear component compatible with macroscopic fat (short arrow). Axial T1-weighted image (A). Axial T1-weighted fat-saturated contrast-enhanced image (B).
Differential Diagnosis.
The imaging findings of glioneuronal tumors are quite varied, and the number of differential diagnoses is high. The identification of a focal lesion with a cystic component in the CNS should signal the possibility of glioneuronal and low-grade glial tumors. The diagnostic approach can be facilitated with a flow chart organized according to the morphology of the lesion, its location, and ancillary findings (Fig 1). Next, imaging features of the main differential diagnosis of uncommon glioneuronal tumors will be summarized.
Ganglioglioma, DNET, and desmoplastic infantile tumors are common WHO grade I neuronal-glial tumors that usually affect the superficial temporal or frontal lobes of children and young adults.1⇓⇓⇓-5,8 Ganglioglioma presents as a mixed solid and cystic lesion with calcification, increased rCBV, and homogeneous enhancement of the solid portion; however, atypical finding, such as heterogeneous enhancement and superficial siderosis may also occur (Online Supplemental Data).1⇓⇓⇓-5 DNET is characterized by a cortically based bubbly wedge-shaped lesion with an increased myo-inositol peak, heterogeneously reduced rCBV, usually no contrast enhancement, and a thin halo of hyperintense signal in FLAIR (Online Supplemental Data).1⇓⇓⇓-5 Calvarial remodeling, adjacent focal cortical dysplasia, and displacement of white matter tracts rather than disruption in tractography may also be present in both, mass effect is minimal if present, and perilesional edema is usually absent.1⇓⇓⇓-5 Desmoplastic infantile tumor presents as a large multilobar mixed solid and cystic lesion with a deep cystic component and a superficial solid plaquelike or dural-based portion, with the dural tail sign, diffusion restriction, avid heterogeneous enhancement, mass effect, and mild perilesional edema (Online Supplemental Data).2,3,5
Polymorphous low‐grade neuroepithelial tumor of the young is a rare and recently described entity, the categorization of which is not well-defined. It is not yet graded by the WHO and may be considered a low-grade neuroepithelial or a glioneuronal tumor.6,41,42 The temporal lobe is the most frequent site, and seizures are the major clinical presentation.41,42 Imaging depicts a superficial, solid tumor with isointense-to-hyperintense signal on T1-weighted imaging, hyperintense signal on T2-weighted and FLAIR imaging, calcification, cystic degeneration, and irregular or nodular contrast enhancement (Online Supplemental Data).41⇓-43 Small nodular diffusion restriction foci and focal high rCBV may rarely occur; however, mass effect and perilesional edema are absent.41⇓-43 Pathology and molecular diagnostics are characterized by oligodendroglioma-like cellular features, an infiltrative growth pattern, pseudorosette formation, intense CD34 immunopositivity, BRAF p.V600E mutation, or FGFR2/3 fusion.6,41,42
Pleomorphic xanthoastrocytoma and angiocentric glioma are low-grade glial epilepsy-related tumors that usually affect the superficial temporal, frontal, or parietal lobes of children and young adults.3,4,8,44 Pleomorphic xanthoastrocytoma is characterized by a cyst and a leptomeningeal-based mural nodule with avid contrast enhancement and an adjacent dural tail sign (Online Supplemental Data).3,4 Angiocentric glioma presents as a diffusely infiltrating and noncircumscribed lesion, with increased ribbonlike signal on T1-weighted imaging, hyperintense signal on T2-weighted and FLAIR imaging, a high Cho peak, a low NAA peak, reduced rCBV, and no contrast enhancement (Online Supplemental Data).44 Additionally, although pilocytic astrocytoma is not an epilepsy-related tumor, it still is the most common low-grade glioma of young patients and also is a differential diagnosis of glioneuronal tumors, especially papillary.3 Pilocytic astrocytoma is commonly seen in children and characterized by a posterior fossa solid-cystic tumor with a marked enhancement of the solid portion.13
CONCLUSIONS
Glioneuronal tumors are an uncommon group of brain tumors with heterogeneous pathologic, radiologic, and prognostic features. With the growing description of immunohistochemistry and molecular findings of these tumors, new subtypes are being reported. The typical imaging findings of some glioneuronal tumors may facilitate the distinction from low-grade glial tumors and guide the pathologic investigation with targeted immunohistochemistry and molecular research. Therefore, neuroimaging may play a pivotal role in the correct diagnosis and management of glioneuronal tumors.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received October 15, 2021.
- Accepted after revision December 18, 2021.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.