Abstract
BACKGROUND AND PURPOSE: A preliminary report suggested that magnetization transfer ratio (MTR) was useful to lateralize epileptic foci in patients with refractory temporal lobe epilepsy (TLE). We attempted to confirm this finding in a larger group by investigating the relationship between MTR of mesial temporal structures and seizure lateralization in patients with refractory TLE.
METHODS: We compared the MTR of amygdalae and hippocampi of 10 patients with unilateral TLE to values obtained from 10 healthy control participants.
RESULTS: Three of 10 patients with TLE had MTR values that were 2 SD below the normal mean; the MTR abnormality was concordant with electroclinical lateralization in only one of the three.
CONCLUSION: We conclude that MTR measurements of amygdalae and hippocampi are not useful for lateralization of TLE.
MR imaging of the brain produces images that reflect the distribution of water among various chemical environments. Hydrogen nuclei associated with various semisolid (macromolecular) components have extremely short T2 values (less than approximately 100 ms) and are not directly detectable with MR imaging because minimum echo times on clinical scanners are typically two orders of magnitude longer. However, interaction between semisolid and bulk water protons results in a continuous exchange of magnetization, referred to as cross relaxation or magnetization transfer (MT) (1, 2). MT imaging detects this exchange by selectively saturating the semisolid magnetization pool and measuring the resulting decrease in the bulk water signal due to transfer of this saturation in regions undergoing exchange (3–7). A preliminary report assessing the lateralization value of MT measurements in patients with temporal lobe epilepsy (TLE) has shown promising results (8). Tofts et al (8) measured hippocampal MT ratios (MTR) in two control participants and in three patients with TLE with atrophic left hippocampus revealed by MR imaging and left temporal abnormality revealed by EEG. Side-to-side comparison of MTR through the hippocampi of the three patients with TLE showed reduced MTR values at the side of the abnormalities revealed by MR imaging and EEG. We further investigated whether MT measurement could be clinically useful in lateralizing seizure site in patients with refractory TLE.
Methods
Participants
We selected 10 consecutive patients (seven women and three men; mean age, 38 years; age range, 26–54 years) with unilateral, non-foreign tissue lesional TLE who were referred for preoperative evaluation (Table). The side of seizure origin and the syndromic classification were defined after a comprehensive workup that included prolonged video monitoring for seizure recording. Seven patients had aura suggestive of temporolimbic origin. Three others did not report aura (Table, patients 5, 7, and 8). Two patients (Table, patients 5 and 9) had febrile seizures, and one patient (Table, patient 6) had meningitis. None had a family history of seizure disorder. Three patients reported secondarily generalized tonicoclonic seizures (Table, patients 4, 10, and 11). Eight of the 10 patients had MR volumetric measurement abnormalities (four had unilateral hippocampal atrophy, three had unilateral amygdaline hippocampal atrophy, and one had asymmetry of the amygdalae) lateralized to the side of EEG focus. Only two patients (Table, patients 1 and 10) had normal volumes of amygdala and hippocampus. Surface interictal EEG showed epileptic activity predominantly over the anterior mesial temporal region with some occasional independent spikes in the homologous region in all patients. Surface ictal EEG showed unilateral anteromesial temporal lobe onset in all patients (six left-sided and four right-sided onsets).
Summary of clinical information, MTR, and volumetric data
Control participants were composed of 10 research staff (seven men and three women; mean age, 32 years; age range, 19–51 years). All were in good health, and none were receiving any medication at the time of imaging. There was no significant difference in age between patients and participants (t test, P = .18).
MT Acquisition and Data Analysis
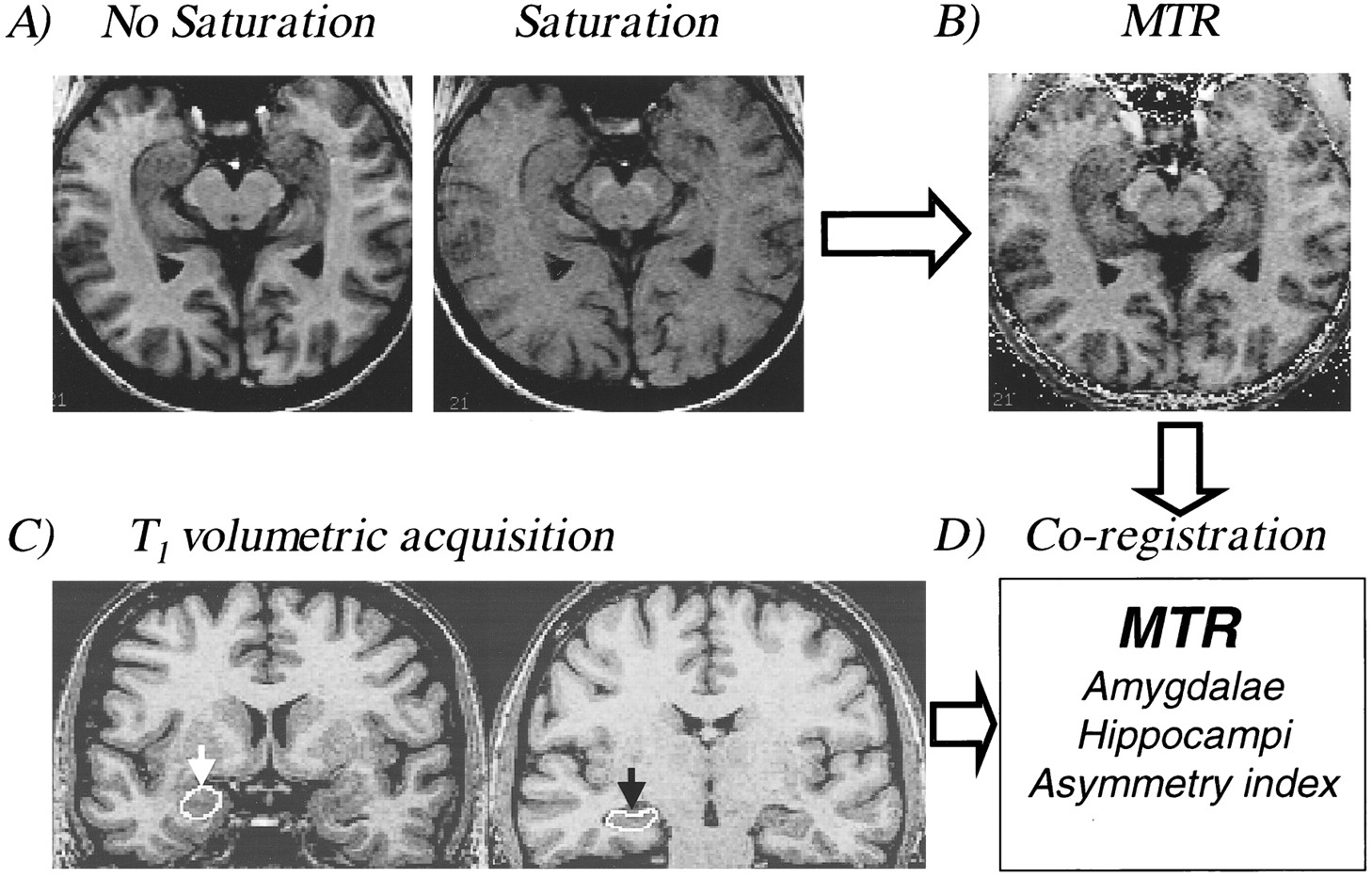
MT images were obtained using a Philips Gyroscan ACS-II (Best, The Netherlands) with a field strength of 1.5 T. Fifty transverse sections (3-mm-thick) covering the whole brain were acquired, angled along the temporal plane. T1-weighted and MT images were obtained using a pair of 3D gradient-echo acquisitions, without (No Sat) and with (Sat) MT saturation pulses, respectively, using 35/10/1 (TR/TE/ excitations) and a flip angle of 40 degrees. Semisolid spin saturation was achieved using 1.2 ms on-resonance |2| binomial pulses (|B1| = 19 μT) placed just before each section selective excitation. Percentage difference (100 × [No Sat—Sat]/No Sat) MT images were calculated after thresholding above the noise background (Fig 1).

{kind=link}
Computation of MTR in amygdala and hippocampus.>>A, Fifty transverse sections (3 mm) covering the whole brain and angled along the temporal plane by use of a pair of 3D gradient-echo acquisitions, without (No Sat) and with (Sat) MT saturation pulses, respectively, were obtained using 35/10/1 and a flip angle of 40 degrees. Semisolid spin saturation was achieved using 1.2-ms on-resonance 121 binomial pulses (|B1| = 19 μT) placed just before each section selective excitation.
B, Percentage difference (100 × [No Sat—Sat]/No Sat) MT images were calculated after thresholding above the noise background.
C, Amygdala (white arrow) and hippocampus (black arrow) were outlined on volumetric T1-weighted 1-mm isotropic voxel acquisition.
D, Volumetric T1-weighted images, with outlined mesial temporal structures, and MT images were coregistered. The MTR of amygdalae, hippocampi, and asymmetry index were computed.
Coronal images reformatted from the transverse 3-mm-thick No Sat MT images were not of sufficient resolution for segmentation of the mesial temporal structures. Thus, we outlined amygdalae and hippocampi on 1-mm-thick contiguous T1-weighted images (18/9/1; flip angle, 30°; field of view, 256; matrix, 256 × 256) using a previously described segmentation protocol (Fig 1) (9, 10), registered the MT images with the 1-mm T1-weighted image volume (11), and computed the mean MTR values for the outlined structures by use of locally developed software. MTR values that were more than 2 SD below the normal mean were considered abnormal.
Results
Clinical information and mean MTR are shown in the Table. Volumetric measurements of amygdalae and hippocampi showed abnormal values in seven of 10 patients, and these were concordant with the side of seizure origin. MTR in control participants were very symmetrical and had a relatively narrow distribution for amygdalae and hippocampi (Table). MTR were more than 2 SD below the normal mean in three patients (Table, patients 1, 8, and 10) and were concordant with electroclinical diagnosis in patient 1 only and discordant in the remaining two patients. There was no difference between the three patients with abnormal MTR and the seven patients with normal MTR regarding the duration of epilepsy and the age of seizure onset (Mann-Whitney U test, P > .05) or the presence of aura or secondarily generalized tonicoclonic seizures, associated risk factors (febrile seizure, meningitis), and presence of amygdaloid or hippocampal atrophy (Fisher's exact test, P > .05, two-tailed).
Discussion
The results indicate that MTR measurements in amygdalae and hippocampi are not useful in the lateralization of temporal lobe epilepsy. We do not think that the low sensitivity observed is due to the MT acquisition and processing. Although our MT protocol is different from that used by Tofts et al (8), the methods are well established (3, 7) and produced very similar MTR measures with low coefficients of variation in our control group for both amygdala and hippocampus. Nevertheless, the variation observed in our control group was larger than that reported previously (8), which is not surprising considering the very small sample size in that report. Even if we had considered a 5% difference to be abnormal for hippocampus, we would have detected only one more patient (Table, patient 6) with an abnormal MTR.
Our patients had electroclinical and MR evidence of mesial temporal lobe epilepsy, and eight had severe hippocampal atrophy. Mesial temporal structures play an important role in seizure generation; however, the reason that MTR of amygdala and hippocampus was not decreased in our series is not clear. It could be that although in hippocampal sclerosis there is preferential selective neuronal loss in the hippocampal subfields, mossy fiber sprouting, and astrogliosis leading to volume decrease, the relative cell density in the outlined MR imaging region of interest might not change enough to cause a significant drop in the MTR. Of interest is that two of the three patients with abnormal MTR had normal volumes. Regarding the relationship between MTR abnormality observed in three patients and their seizure lateralization, only one had concordant MTR and EEG lateralization, whereas in the other two, the MTR lateralized to the side opposite that of EEG.
Although MTR is very sensitive to white matter pathologic abnormalities in multiple sclerosis, this seemed not to be the case in epileptic lesions, which might reflect different underlying pathophysiologic mechanisms of neuronal versus axonal damage. If this is the case, it is possible that measurement of MTR in the white matter of patients with epilepsy may be abnormal because of axonal damage secondary to neuronal loss (Wallerian degeneration) or the presence of microdysgenesis seen in some patients with refractory TLE.
Acknowledgments
This study was funded by the Medical Research Council of Canada. Dr. Li is a recipient of a Jeanne-Timmins-Costello Fellowship. We are grateful for Drs. Alan Evans and Louis Collins of the McConnell Brain Imaging Center for providing data analysis software.
References
- Received November 15, 1999.
- Accepted after revision April 19, 2000.
- Copyright © American Society of Neuroradiology