Abstract
BACKGROUND AND PURPOSE: Medulloblastoma is one of the most common posterior fossa tumors to occur in children. Our purpose was to document the frequency, location, and time of occurrence of intracranial calcifications in cranial CT studies of children with medulloblastoma.
METHODS: We retrospectively reviewed cranial CT studies of 56 patients diagnosed with medulloblastoma from 1983 through 1997 for the presence of intracranial calcifications. The findings were compared with 159 cranial CT studies of patients who were evaluated in the emergency department (control group). Thirty-two patients with medulloblastoma without shunts were compared with 118 patients from the control group without shunts. Similarly, 24 patients with medulloblastoma with shunts were compared with 41 patients from the control group with shunts.
RESULTS: Overall, three (9%) patients with medulloblastoma without shunts, four (16%) patients with medulloblastoma with shunts, and four (10%) patients from the control group with shunts had falx calcification. Only the two children carrying the diagnoses of medulloblastoma and nevoid basal cell carcinoma syndrome, however, had calcification of the falx cerebri shown on the cranial CT scans obtained during the peridiagnostic period. Both were diagnosed with medulloblastoma before the age of 3 years and later developed jaw cysts and multiple basal cell carcinomas in the radiation field.
CONCLUSION: Previous studies have shown that falx calcification is a major component of nevoid basal cell carcinoma syndrome. Our two cases illustrate the importance of considering the diagnosis of nevoid basal cell carcinoma syndrome when falx calcification is present in young patients with medulloblastoma. If the concomitant diagnosis of nevoid basal cell carcinoma syndrome is made, alternative types of therapy should be sought to minimize radiation therapy sequelae.
Medulloblastoma is the most common posterior fossa tumor in children and accounts for approximately 20% of all childhood brain tumors (1). The mean age at diagnosis is 6.3 years, and male children are affected more than are female children (1, 2). The treatment of medulloblastoma consists of surgery, radiation therapy, and chemotherapy, and the 5-year survival rate is between 60% and 80% (3–6).
A small percentage (<5%) of children with medulloblastoma carry the concomitant diagnosis of nevoid basal cell carcinoma syndrome, an autosomal dominant multisystem disorder. Nevoid basal cell carcinoma syndrome is characterized by multiple basal cell carcinomas, keratocysts of the jaw, palmar or plantar pits, and several radiologic abnormalities, including early calcification of the falx cerebri, vertebral anomalies, and flame-shaped lucencies of the hands or feet (7, 8). Because several of the major features of nevoid basal cell carcinoma syndrome (eg, basal cell carcinomas and jaw cysts) are most commonly observed starting in adolescence or young adulthood, the presence of early falx calcification may help to establish the diagnosis of nevoid basal cell carcinoma syndrome in children.
Intracranial calcifications in children can be classified as physiologic or pathologic. Physiologic calcification is very uncommon (2%) below the age of 9 years and increases severalfold as children approach 15 years of age. The most common areas of calcification are the pineal gland (5.8%), choroid plexus (4.9%), and dura (0.8%). Pathologic calcifications are most commonly intraparenchymal and have been described in association with tumors, neurocutaneous syndromes, infections, and neurodegenerative disorders. Parenchymal calcifications are seen as a result of radiation therapy for intracranial tumors. There are, however, no reports of falx calcification as a result of radiation therapy or chemotherapy. The reported causes of pathologic falx calcification in children are from children with lissencephaly and pseudopseudohypoparathyroidism (9–13).
We retrospectively reviewed cranial CT studies of 56 children with medulloblastoma to document the frequency, location, and time of occurrence of intracranial calcifications in relation to nevoid basal cell carcinoma syndrome. The findings were compared with 159 cranial CT studies of children who were seen in the emergency department at our institution.
Methods
The cranial CT studies of 56 children diagnosed with medulloblastoma from 1983 through 1997 were evaluated for presence of calcification of the falx cerebri, tentorium cerebelli, petroclinoid ligaments, basal ganglia, pineal gland, sella turcica, choroid plexus, brain parenchyma, leptomeninges, and dura. The presence of a ventriculoperitoneal shunt was also documented.
Cranial CT studies of 118 children who were seen at our institution's emergency department and who had undergone cranial CT for various reasons were also reviewed. This group included all children seen in the emergency department during the last 3 months of 1998 who required CT studies for the following reasons: headaches (n = 22), head trauma (n = 72), new onset seizures (n = 13), skull malformation (n = 3), behavioral disorder (n = 1), gait imbalance (n = 2), vomiting (n = 3), and dizziness (n = 2). Cranial CT studies of 41 patients with ventriculoperitoneal shunts were also evaluated for the presence of calcifications. These children were seen in the emergency department between June and December of 1998 and required CT studies for several reasons, most commonly to rule out shunt malfunction or infection. In these children, the ventriculoperitoneal shunt was placed early in life because of congenital hydrocephalus (aqueductal stenosis [n = 9], Chiari II malformation [n = 20], Dandy-Walker malformation [n = 6], other [n = 6]). The patients seen in the emergency department served as a control group for the patients with medulloblastoma and had the same general age distribution.
All examinations were performed on General Electric 8800, 9800, or Hilight CT scanners (General Electric Medical Systems, Milwaukee, WI). Five-millimeter axial scans were acquired through the posterior fossa and 10-mm scans through the supratentorial space.
One neuroradiologist reviewed all of the radiologic studies. Positive results and negative results that had some questionable aspect were confirmed in a blinded review by a second neuroradiologist. There were no disagreements between the two interpreters. Radiologic differences between patient groups were evaluated using either a χ2 test or Fisher exact test.
Results
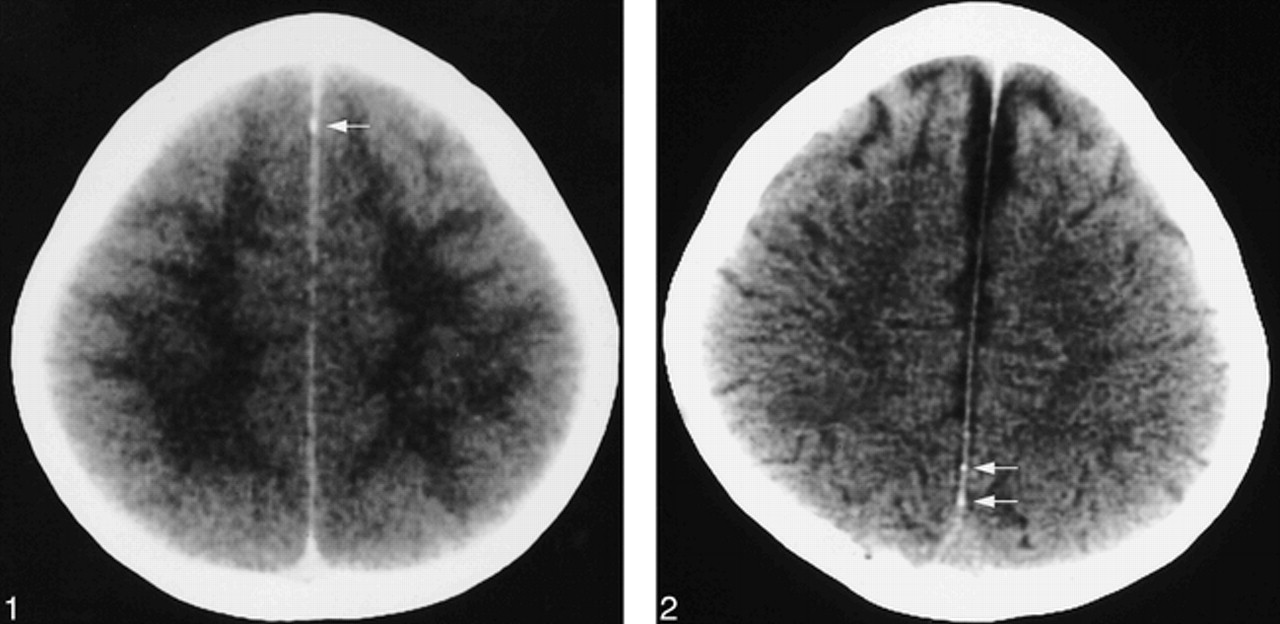
Thirty-two patients with medulloblastoma without shunts were compared with 118 patients from the control group without shunts (Table 1). A total of three (9%) patients with medulloblastoma who did not require shunt placement during the postoperative period had calcification of the falx cerebri (Table 2). One of these patients was diagnosed with medulloblastoma at the age of 13 years, and he developed falx calcification at the age of 20 years. The other two patients had falx calcification documented by cranial CT at the ages of 2.5 and 2 years, respectively (Figs 1 and 2). These were the only patients who also carried the diagnosis of nevoid basal cell carcinoma syndrome. The two patients both presented with medulloblastoma at a young age (<3 years); one underwent gross total resection and received radiation therapy, and the second underwent incomplete resection and was treated with radiation therapy and chemotherapy. Both patients exhibited other manifestations of nevoid basal cell carcinoma syndrome, including the presence of palmar and plantar pits and jaw cysts 3 and 2 years, respectively, subsequent to medulloblastoma diagnosis. They also developed multiple basal cell carcinomas in the radiation field 6 and 3 years, respectively, after radiation therapy. Falx calcification was not seen in any of the 118 patients from the control group, and this difference was statistically significant (P = .009).
Intracranial calcifications in patients without shunts
Characteristics of falx calcification in medulloblastoma patients

{kind=link}
Male patient, diagnosed with medulloblastoma at age 2.5 years, underwent gross total resection and received radiation therapy. Other manifestations of nevoid basal cell carcinoma syndrome that developed subsequent to the diagnosis of medulloblastoma included palmar and plantar pits, numerous jaw cysts, and many basal cell carcinomas in the radiation field. The basal cell carcinomas developed 6 years after radiation therapy. Diagnostic axial CT scan obtained at age 2.5 years reveals one calcification of the anterior interhemispheric falx (arrow).fig 2. Male patient, diagnosed with medulloblastoma at age 2 years, underwent incomplete resection and was treated with radiation therapy and chemotherapy. Other manifestations of nevoid basal cell carcinoma syndrome that developed subsequent to the diagnosis of medulloblastoma included palmar and plantar pits, numerous jaw cysts, and many basal cell carcinomas in the radiation field. The basal cell carcinomas developed 3 years after radiation therapy. Axial CT scan obtained within 3 months of medulloblastoma diagnosis and surgery reveals two calcifications along the posterior interhemispheric falx (arrows)
The following calcifications were also noted in the patients with medulloblastoma without ventriculoperitoneal shunts: choroid plexus (28%), tentorium cerebelli (9%), pineal gland (12%), parenchymal (6%), leptomeningeal (3%), and dural (3%). In the patients from the control group without shunts, only choroid plexus (22%) and pineal gland (13%) calcifications were documented.
A comparison was also made between 24 patients with medulloblastoma and 41 patients from the control group with shunts (Table 3). Four (16%) patients with medulloblastoma who required shunt placement during the postoperative period had falx calcification that was observed at a mean age of 13.5 years (Table 2). Similarly, there were four (10%) patients with falx calcification in the control group who required ventriculoperitoneal shunt placement early in life (Table 4). The mean age of the development of falx calcification in these patients was 10 years. No statistically significant difference in the frequency of falx calcification was observed between the two groups (P = .5).
Intracranial calcifications in patients with VP shunts
Characteristics of falx calcification in control subjects
The group of patients with medulloblastoma with ventriculoperitoneal shunts also showed calcifications in the following areas: choroid plexus (33%), tentorium cerebelli (21%), basal ganglia (12%), pineal gland (8%), parenchymal (4%), and dural (8%). In the control group with shunts, calcifications were documented in the choroid plexus (17%) and pineal gland (7%).
With the exception of the two patients with nevoid basal cell carcinoma syndrome, there was one other patient with calcification of the falx (3%). In the medulloblastoma group with shunts, there were four patients (16%) who had falx calcification. When these groups were compared, the difference was not statistically significant.
Discussion
The age at the time of onset of physiologic falx calcification has not been well established. In our control population of children without shunts, no falx calcifications were seen. This result is consistent with a previous report showing an incidence of less than 1% in a pediatric population (11). An early onset and higher frequency (85%) has been described in adult and pediatric patients with nevoid basal cell carcinoma syndrome (7).
The incidence of nevoid basal cell carcinoma syndrome in patients with medulloblastoma is estimated to be between 1% and 2% overall and between 4% and 5% in patients younger than 5 years (14). The most frequent diagnostic findings of nevoid basal cell carcinoma syndrome include the presence of multiple basal cell carcinomas, jaw cysts, palmar or plantar pits, and calcified falx cerebri (7, 15, 16). Basal cell carcinomas can be seen in children but are most commonly observed in adolescents and young adults. Jaw cysts are more common during the second and third decades of life (7). Because of the age-related onset of many features of nevoid basal cell carcinoma syndrome, assessment of family history of other relatives, physical examination of the parents, and presence of early calcification of the falx cerebri can help establish the diagnosis of nevoid basal cell carcinoma syndrome in young children with medulloblastoma.
In our patients with medulloblastoma, calcification of the falx cerebri occurred in the majority of the cases at age 12 years or older (five of seven patients). The other two patients, for whom initial falx calcification was shown at a much earlier age, are the only ones known to carry the diagnosis of nevoid basal cell carcinoma syndrome. In one of these patients, the calcification was present on the diagnostic CT scan (Fig 1). The other patient had falx calcification shown within 3 months of diagnosis and surgery (Fig 2). His diagnostic CT scan was not available for review. Both of these patients presented with medulloblastoma before they were 3 years old, and they later exhibited other manifestations of nevoid basal cell carcinoma syndrome, including the presence of palmar and plantar pits, multiple jaw cysts, and many basal cell carcinomas. Significant morbidity was observed in these two cases because of the development of many basal cell carcinomas in the irradiated areas.
There have been no previous reports showing statistically significant evidence for increased incidence of falx calcification after ventricular shunt placement. The observed statistically significant difference between patients from the control group with shunts and patients from the control group without shunts (P = .004) indicates that falx calcification is likely to occur after shunt placement. The same statistical difference was not observed between patients with medulloblastoma with shunts and patients with medulloblastoma without shunts.
There was a higher frequency of basal ganglia and tentorium cerebelli calcifications in the patients with medulloblastoma with shunts when compared with patients from the control group with shunts (P = .05 for basal ganglia and P = .005 for tentorium cerebelli). This difference could likely be attributed to treatment-related side effects. Parenchymal calcifications have been identified previously in children who have received radiation therapy (13).
The frequency of identifying pineal and choroid calcifications has been estimated to be 2% in children up to the age of 8 years and 9% to 11% in older children when EMI scanners (EMI Medical Ltd., Hayes, Middlesex, UK) are used (11). The higher incidence of pineal and choroid calcifications seen in our group of patients may be related to higher resolution of the recent CT scanners compared with the EMI scanners used in earlier studies.
Conclusion
Our finding of early falx calcification in young patients with medulloblastoma suggests that it could be used as an indicator of the concomitant diagnosis of nevoid basal cell carcinoma syndrome. Because many of these patients are known to develop numerous basal cell carcinomas in the irradiated areas, alternative types of treatment, such as chemotherapy alone or alternate focal radiation with chemotherapy, should be considered to minimize treatment-related sequelae.
Footnotes
1 Presented at the Annual Meeting of the American Society of Neuroradiology, San Diego, CA, May 1999.
2 Address reprint requests to Alisa M. Goldstein, PhD, Genetic Epidemiology Branch/National Cancer Institute/National Institutes of Health, Executive Plaza South MSC 7236, 6120 Executive Boulevard, Bethesda, MD 20892-7236.
References
- Received June 3, 1999.
- Copyright © American Society of Neuroradiology