Abstract
Summary: We present a case of cerebellopontine (CP) angle ganglioglioma in a young child with developmental delay and no trigeminal nerve symptoms. MR imaging demonstrated a mass of homogeneous low signal intensity in the left CP angle on T1-weighted images with no enhancement with gadolinium, and of relatively homogeneous high signal intensity on T2-weighted images.
Ganglioglioma is an uncommon primary lesion of the CNS, constituting fewer than 2% of all intracranial tumors (1). Gangliogliomas are tumors of glial and neuronal elements that tend to grow slowly and produce focal symptoms, usually from expansion of the mass. They are most commonly seen in children and young adults and there is no gender preponderance (2, 3). The favorable prognosis associated with ganglioglioma makes early recognition important for treatment and patient counseling.
Ganglioglioma may be found at virtually any location of the CNS, such as the spinal cord, brain stem, and optic nerve (3). The common location of ganglioglioma is the temporal lobe, and other locations are the frontal, parietal, and occipital lobes. We present the MR imaging findings of a case of a cerebellopontine (CP) angle ganglioglioma.
Case Report
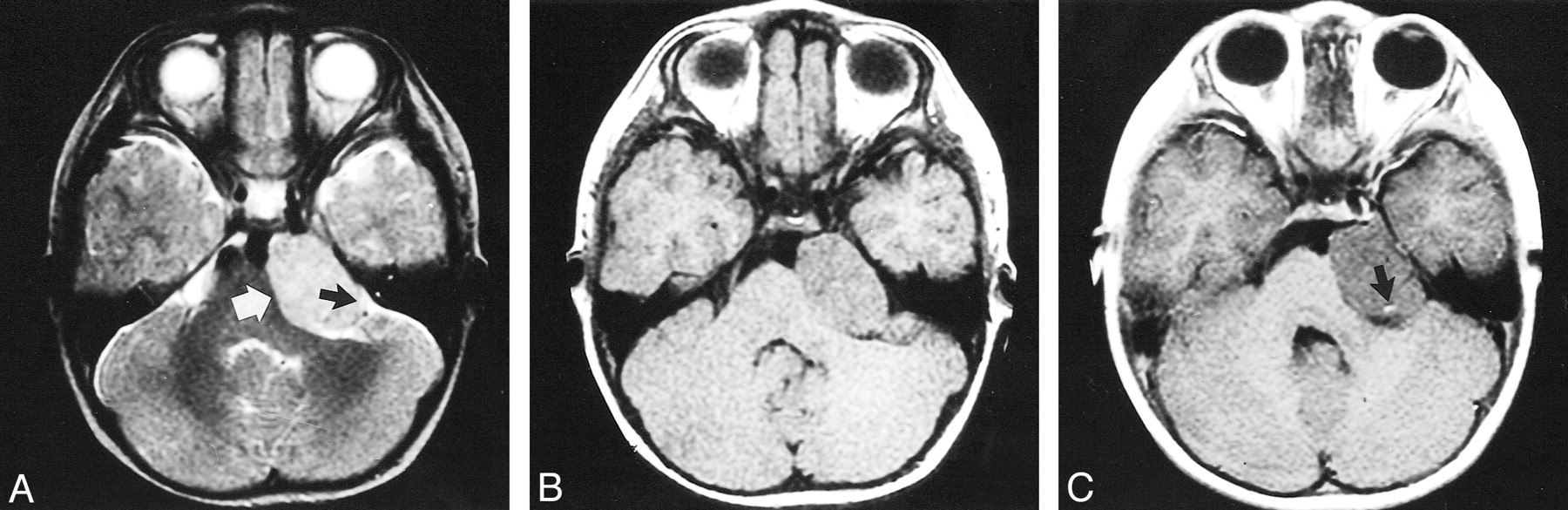
A 2-year-old boy was brought to the hospital because of developmental delay. He had no remarkable neurologic abnormalities. During the workup for the developmental status, a mass (3 × 4 × 3 cm) was found in the left CP angle, compressing the brain stem (Fig 1A–C). A CSF cleft between the mass and the brain stem suggested an extraaxial origin of the tumor. However, the tumor was adjacent to the cerebellum. The tumor was relatively well defined and homogeneous and showed relatively high signal intensity on T2-weighted images (Fig 1A), low signal intensity on T1-weighted images (Fig 1B), and only punctate enhancement on postcontrast images (Fig 1C).

MR imaging of a 2-year-old boy with CP angle ganglioglioma.
A, T2-weighted axial MR image (4300/110/2 [TR/TE/excitations]). The mass shows relatively homogeneous high signal intensity (white arrow). The CSF cleft (black arrow) between the mass and the brain stem suggests the extraaxial origin of the tumor.
B, Precontrast T1-weighted axial MR image (366/11/3) shows a homogeneous low signal intensity mass in left CP angle compressing the brain stem.
C, Contrast-enhanced axial T1-weighted imaging shows no enhancement within the mass and a peritumoral vessel is visible (arrow).
At surgery, the tumor was found to be well encapsulated and vascular. The lesion encased the trigeminal nerve and was adherent to the cerebellum. The lesion was extraaxially located and the surgical impression was a schwannoma originating from the trigeminal nerve. A gross total resection of the tumor was accomplished.
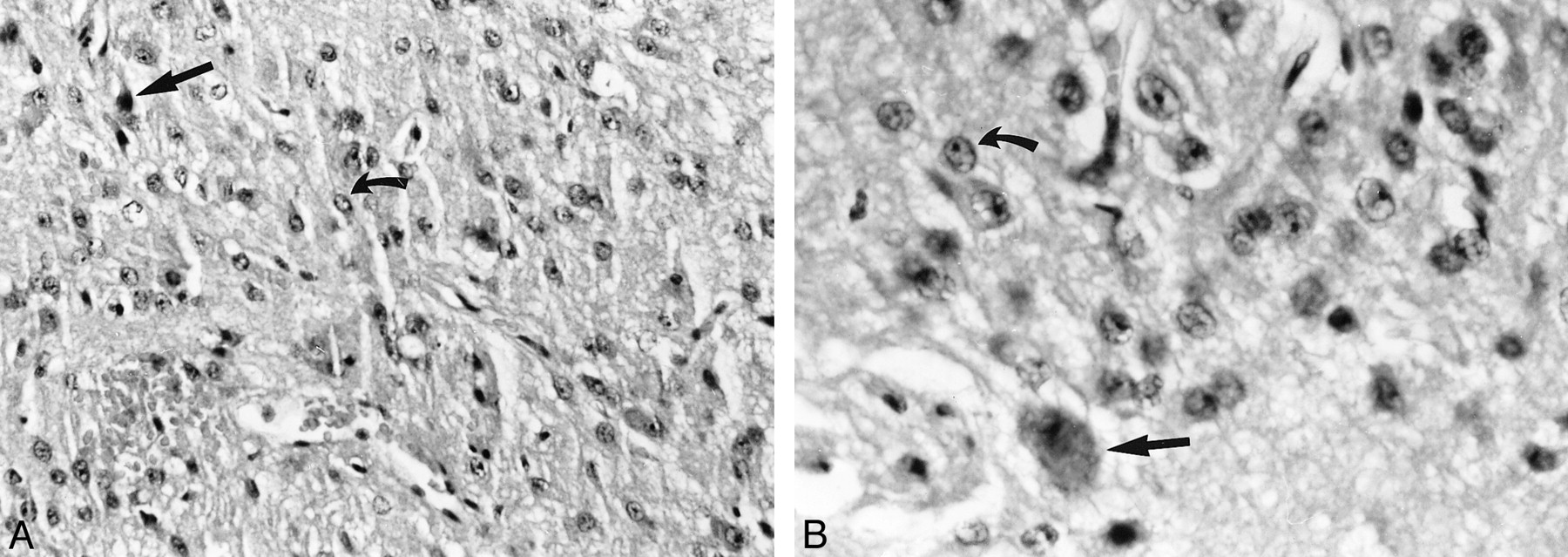
Tumor biopsy demonstrated predominantly a low-grade astrocytoma with haphazard clusters of ganglion (Fig 2A and B). Histologic diagnosis was ganglioglioma (1).

{kind=link}
{kind=link}
Histologic sample.
A and B, The neoplastic nature of the ganglion cell tumor's large neuron (straight arrow) is readily apparent when abnormal clustering and cytologic abnormalities, such as multinucleation and hyperchromaticia, are in evidence. Elsewhere this example harbored many atypical glial elements (curved arrow). Hematoxylin and eosin stain, light microscopy ×200 (A) and ×400 (B).
Discussion
Gangliogliomas are tumors of the CNS that are composed of atypical ganglion cells and astrocytes. Gangliogliomas account for 0.4% to 7.6% of pediatric CNS neoplasms and up to 1.3% of those in adults (3). Gangliogliomas are usually located intraaxially, and the temporal lobe is the most common location of gangliogliomas. Other less frequently involved sites within the cerebral hemispheres are (in order of decreasing frequency) the frontal, parietal, and occipital lobes; involvement of junctional zones between two lobes is not uncommon. Gangliogliomas may be found at virtually any location of the CNS, such as the spinal cord, brain stem, third and fourth ventricles, cerebellum, pineal region, thalamus, sella, and optic nerve (3). Our case is unusual in that it was located in the CP angle and arose from the trigeminal nerve. Previously, two cases of CP angle ganglioglioma were reported and were found to have originated from the cerebellum (4). Axial tumors sometimes appear extraaxial because of the exophytic nature of some brain stem and cerebellar tumors (1, 4).
Most patients with gangliogliomas present with long histories of seizures, whereas focal neurologic deficits or increased intracranial pressure are unusual. The extent of resection is thought to be the main prognostic factor in the treatment of gangliogliomas (3). For most gangliogliomas, radiation therapy seems to be of no benefit. Most authors recommend that radiation therapy should be reserved only for those patients with tumor progression (3).
On plain skull films, a ballooned and thinned calvarium, enlargement of the middle cranial fossa, and floccular calcification may be observed. Cerebral angiography shows an avascular space-occupying lesion. The CT features are not specific; the mass is usually hypodense or isodense, with calcification present in 10% to 31%. Contrast enhancement of the noncalcified solid components of the ganglioglioma is observed in about one half of cases. MR findings also are not characteristic. The tumor appears as a well-defined lesion with variable mass effect and occasional perifocal edema. Gangliogliomas usually have low signal on T1-weighted images but some are isointense. Contrast enhancement may be present. On T2-weighted images, solid lesions show increased signal (1). The variable signal in cystic components depends on whether the contents are proteinaceous, hemorrhagic, or contain CSF. Calcified areas are sometimes visible as low signal on all sequences (5). In our case, there was no definitive calcification. Our case was found to be vascular at surgery but did not enhance with contrast medium administration. Only enhancing peritumoral vessel (Fig 1C) was visualized. Histologic analysis revealed the tumor was not very vascular. We do not have a clear explanation for this discrepancy.
Although CT or MR imaging may suggest the diagnosis, the differential diagnosis must include gangliocytoma, dysembryoplastic neuroepithelial tumor, low-grade astrocytoma, and oligodendroglioma. In the CP angle, schwannoma, hemangioma, and meningioma should be considered in the differential diagnosis, but unlike our case, these usually enhance intensely on postcontrast MR imaging. Epidermoid tumor also may be located in the CP angle. Epidermoid tumors are usually high in signal, similar to CSF, but can occasionally have signal intensity that is different from CSF.
Ganglioglioma is thought to be a tumor of low malignancy potential with a benign clinical course (1). Histologically, gangliogliomas are mixed tumors composed of relatively mature neoplastic glial and ganglion cells in varying proportions (Fig 2A and B). Both components usually exhibit low grades of malignancy, but it is the grade of the gliomatous element that predicts the biological behavior of the tumor. The cell of origin of each component has long been a clinicopathologic mystery. Many mechanisms could account for the presence of neoplastic glial and neuronal cells in gangliogliomas. These two components could arise independently, with either independent expansions of glioblasts and apolar neuroblasts within the same tumor, or through interaction between these precursors in a paracrine fashion. Alternatively, the two components could be derived from a single abnormal progenitor cell, such as a neuroepithelial cell, which then differentiates into both glial and neuronal elements during pathogenetic development (6). Some findings support the hypothesis that gangliogliomas represent developmental lesions. These include histopathologic evidence of associated disordered neuronal migration and a long clinical history in many patients (3). Histologic diagnosis may be complicated because of difficulty in determining whether the ganglion cells are truly neoplastic, or simply “trapped” neurons in an infiltrating glioma (1). Ganglioglioma was named for its histologic components of differentiated nerve cells, in the form of ganglion cells, with a glial background that is typically astrocytic (1). Malignant transformation is unusual and, when it occurs, most often involves glial cells (glioblastoma) and, less frequently, ganglion cells (neuroblastoma). Leptomeningeal extension is rare (5).
In conclusion, although the diagnosis of CP angle ganglioglioma is rarely made prior to surgery, MR imaging may suggest the diagnosis by demonstrating a lesion with low intensity on T1-weighted images with no contrast enhancement, and high intensity on T2-weighted images involving the CP angle region.
Footnotes
1 Address reprint requests to In-One Kim, MD, Department of Radiology, Seoul National University Hospital, 28, Yongon-Dong, Chongno-Gu, Seoul, 110-744, Korea.
References
- Received December 1, 2000.
- Accepted after revision March 20, 2001.
- Copyright © American Society of Neuroradiology