Abstract
Summary: We report two cases of epidermal nevus syndrome (ENS) involving the spine. MR imaging of the spine demonstrated intraspinal lipomas in both cases. Abnormal, enhancing, enlarged cervical and lumbosacral nerve roots were present in one patient. Spinal imaging for patients with ENS may help in the diagnosis of subtle intracranial manifestations, as it did in both of our cases. ENS has features similar to those of other neurocutaneous syndromes, such as neurofibromatosis type 1 and encephalocraniocutaneous lipomatosis.
Epidermal nevus syndrome (ENS) is a rare sporadic neurocutaneous disorder characterized by an epidermal nevus and cerebral anomalies (1). Central nervous system anomalies are typically severe and ipsilateral to the nevus. Imaging and autopsy reports of central nervous system involvement in children with ENS have predominately focused on the brain. The wide spectrum of central nervous system abnormalities includes those ranging from ventriculomegaly to severe migrational disorders (2–6). We report abnormalities of the spine in two cases.
Case Reports
Case 1
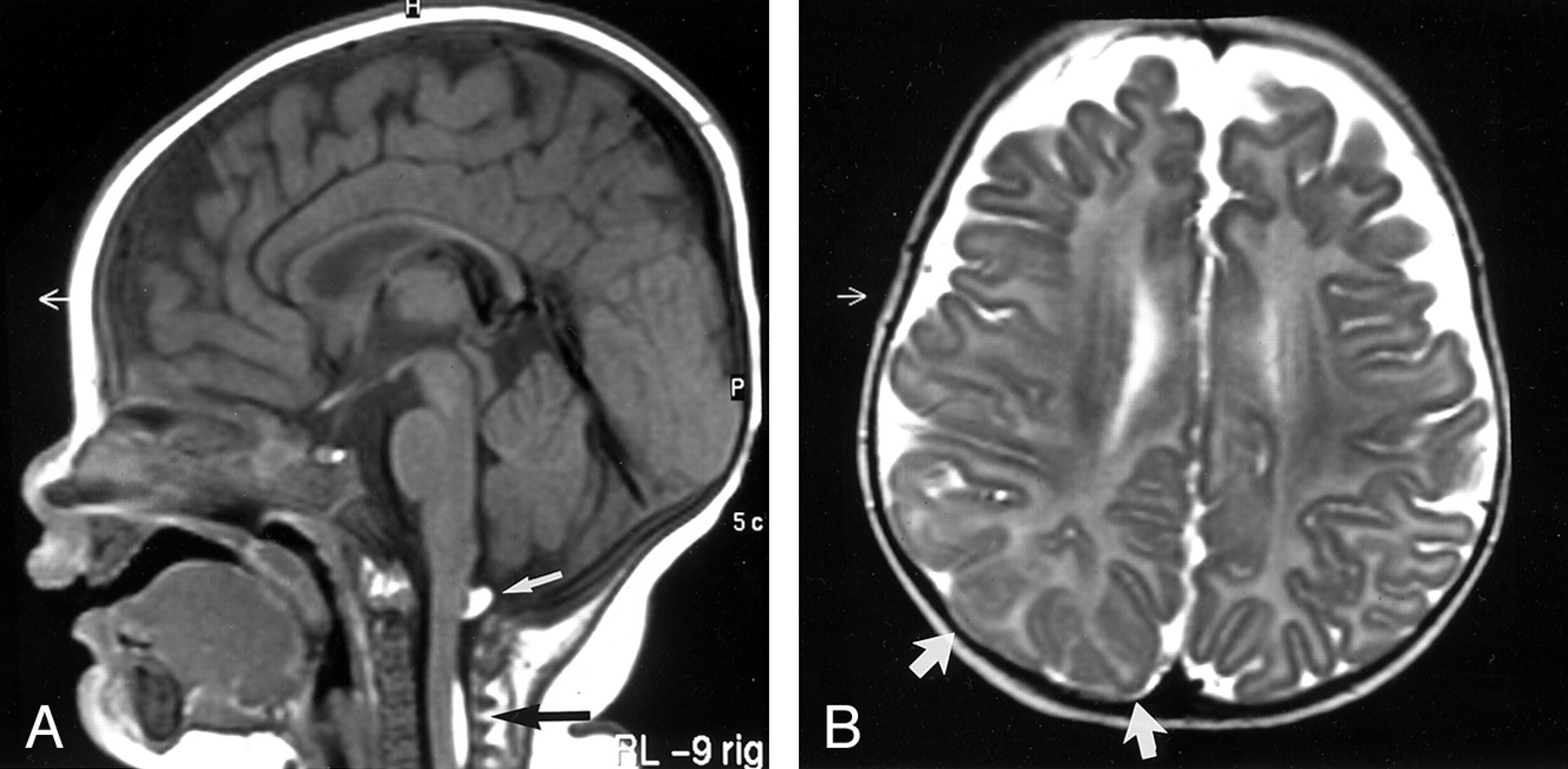
A 5-month-old female infant presented with a right-sided epidermal nevus (nevus unius lateralis) involving her right torso, arm, neck, and face. A right multicystic dysplastic kidney and refractory ectopic atrial tachycardia were noted at clinical examination. MR examination of the brain and spine were performed because of the presence of infantile spasms. A subpial lipoma was noted dorsal to the cervicomedullary junction, and a larger lipoma was present dorsal to the midcervical cord (Fig 1A). No symptoms of cord compression or associated osseous anomalies were present. The entire spine was imaged, and no additional abnormalities were found. Imaging of the brain revealed only one subtle region of suspected cortical dysplasia involving the right parietal and occipital lobes (Fig 1B).

Case 1. A 5-month-old female infant with a right-sided epidermal nevus (nevus unius lateralis) involving her right torso, arm, neck, and face.
A, Sagittal T1-weighted (425/15/2 [TR/TE/NEX]) MR image shows two subpial lesions that are dorsal to the cervical cord (arrows). Both lesions are homogeneously hyperintense. The signal intensity was suppressed with chemical fat-saturation techniques (not shown).
B, Axial T2-weighted (4500/150/3) MR image shows subtle thickening and poor definition of the right parietal cortex (arrows), which likely represent a focal cortical dysplasia.
Case 2
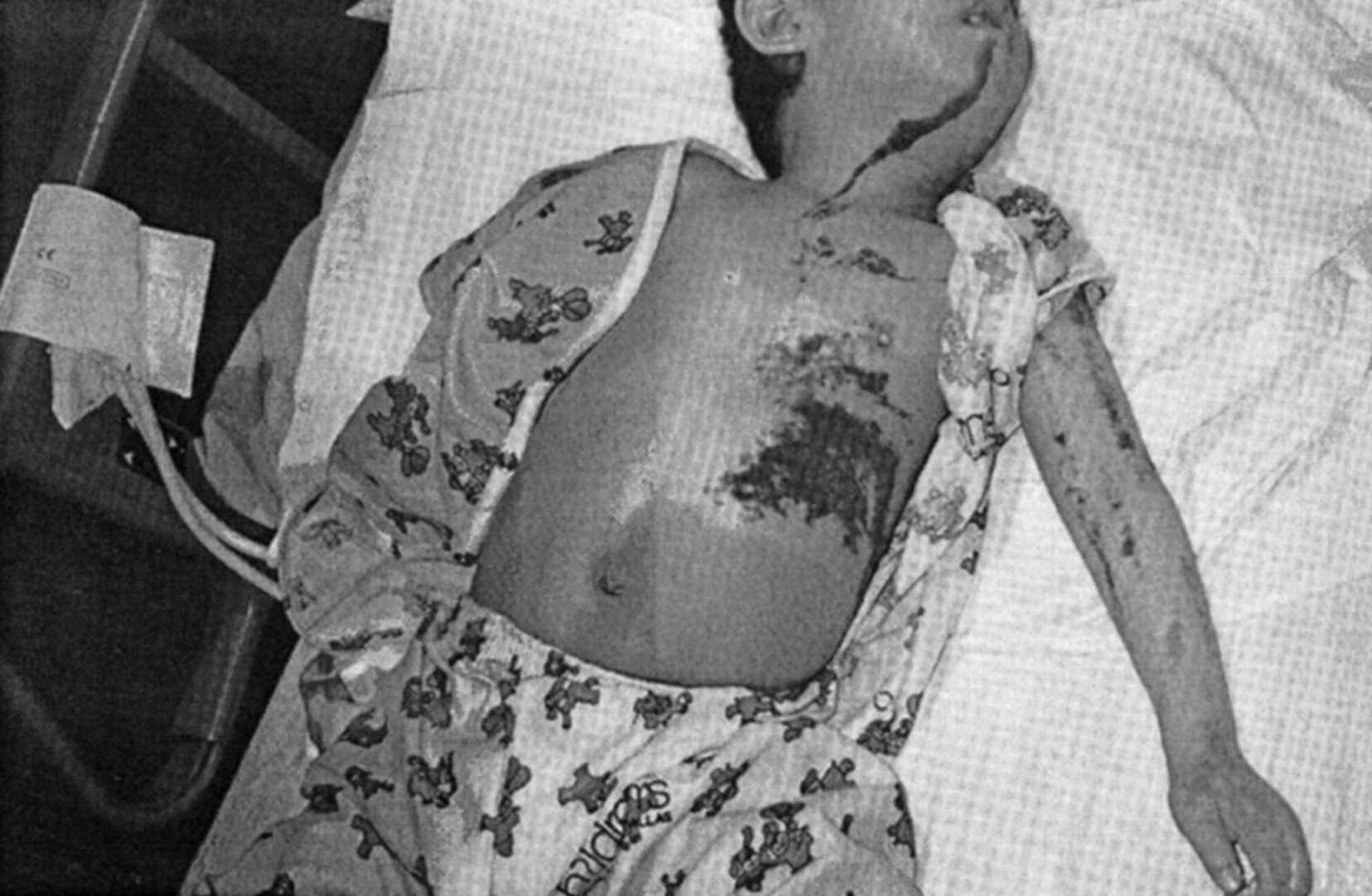
A 3-year-old boy presented with an epidermal nevus involving his left torso, extremities, neck, face, and head. The nevus was a linear, brown, verrucous plaque (Fig 2). Cardiac anomalies included a small ventriculoseptal defect and mild subaortic stenosis. Left simple renal cysts and a left cataract were also noted. Additionally, physical examination revealed hypertrophy of the left lower extremity. Radiographs of the lower extremity revealed a dysplastic femur, tibia, and fibula that had appearances similar to those seen in neurofibromatosis 1. CT examination of the lower extremity revealed enlargement of the leg with an increase in subcutaneous fat, as well as the presence of a nonlipomatous soft-tissue component (Fig 3A). Findings were thought to be most consistent with a plexiform neurofibroma or venolymphatic malformation. The more cephalic images depicted enlargement of lumbosacral nerve roots (Fig 3B), and MR imaging of the spine was recommended. Two subpial lipomas were incidentally noted dorsal to the cervical and upper thoracic cord (Fig 3C). The regional osseous structures were normal. Cervical nerve roots were diffusely enlarged and revealed intense enhancement (Fig 3D and E). In addition, extensive thickening and abnormal enhancement of the lumbar and sacral nerve roots were identified (Fig 3F–H). Imaging findings were thought to be consistent with those of either neurofibromas or possibly hypertrophic neuropathy. Biopsy was not performed. The patient underwent MR examination of the brain because of seizures and severe developmental delay. A subtle cortical dysplasia involved the left temporal lobe (Fig 3I).

Case 2. A 3-year-old boy presented with an epidermal nevus involving the left side of his torso, extremities, neck, face, and head. Linear, brown, verrucous, plaquelike epidermal nevus involves the left side of the neck, face, and body.

{kind=link}
{kind=link}
{kind=link}
Case 2.
A, Axial contrast-enhanced CT scan obtained at the level of the distal femur shows marked enlargement of the leg with a lipomatous and soft-tissue component (arrow).
B, Delayed axial CT scan obtained at the midpelvis shows that the nerve roots in the spinal canal and sacral foramina are enlarged (arrows).
C, Nonenhanced midline sagittal T1-weighted (450/20/2) MR image shows two subpial lipomas dorsal to the cord (arrows).
D, Nonenhanced off-midline T1-weighted (450/20/2) MR image shows that the cervical nerve roots are enlarged at the level of the neuroforamina (arrowheads).
E, Axial fat-suppressed contrast-enhanced T1-weighted (450/20/3) MR image at the C2-C3 level shows that the enlarged nerves are abnormally enhancing. Mass effect on the adjacent thecal sac is present.
F, Coronal T1-weighted (450/20/2) MR image of the lumbar spine shows thickened lumbar nerve roots. No lipomatous component is present.
G and H, Sagittal contrast-enhanced fat-suppressed T1-weighted (450/20/3) MR images show thickening and abnormal enhancement of the lumbar and sacral nerves within both the thecal sac (arrows in H) and the foramina (arrowheads in I).
I, Coronal T2-weighted (3000/120/3) MR image obtained through the temporal lobes shows slight thickening of the left temporal cortex with poor arborization of the inferior white matter tracts (arrow).
Discussion
ENS is diagnosed on the basis of a variety of skin lesions associated with developmental as well as acquired abnormalities of the central nervous system. Characteristic skin lesions include nevus sebaceous of Jadassohn, nevus unius lateris, linear epidermal nevus, and inflammatory linear verrucous epidermal nevus. The presence of these nevi initially suggests the diagnosis. Neurologic examination reveals cranial nerve palsies, developmental delay, and seizures. Ocular abnormalities such as colobomas, optic nerve hypoplasia, micro-opthalmia, and cataracts are also common. Systemic involvement with skeletal, cardiac, and renal abnormalities is common (7).
Imaging and autopsy findings in the central nervous system reveal both acquired and developmental abnormalities associated with epidermal nevi. The reported central nervous system abnormalities have been limited to the brain exclusively. Hydrocephalus, heterotopias, hemimegalencephaly, and hamartomas have been observed (2, 4, 6, 8). The classic neurologic variant consists of hemimegalencephaly, facial hemihypertrophy, and pachygyria or polymicrogyria (4). In addition to an increased risk of malignancy in the nevus, cerebral neoplasms, including gliomatosis cerebri, are described (9). Vascular abnormalities reported include infarction, porencephaly, cortical calcification, and vascular dysplasia (2, 10). The two cases presented were unique because of the presence of very subtle dysplasias involving the cerebral cortex. The lesions in both patients were ipsilateral to the nevus; this finding has been inconsistently stated in the literature (6).
MR imaging of the spine demonstrated obvious abnormalities in both patients. These abnormalities were much more readily identified than were the cortical dysplasias. In both patients, large lipomas were present in the spinal canal. Intracranial and intraspinal lipomas have not been reported in ENS. However, lipomas have been described outside the central nervous system. In the literature, ENS has been noted to have features that overlap with those of Proteus syndrome and encephalocraniocutaneous lipomatosis (ECCL) (6). ECCL is a neurocutaneous syndrome characterized by unilateral lipomas of the cranium, face, and neck. Ipsilateral ventriculomegaly, intracranial lipomas, dysplastic cortex, and corticopial calcifications are characteristically associated with the syndrome (11). Similar findings have been reported in ENS, both in the literature and in the two presented cases. The presence of lipomas links ECCL to our two cases of ENS. In addition, corticopial calcifications and abnormal pial enhancement have been described in both syndromes (2, 11). The possibility that these syndromes may represent a continuum with a common pathogenic process and branching pathways has been raised. A common somatic mutation, which could lead to the clinically encountered mosaicism, has been hypothesized (6, 11).
MR imaging of the spine in patient 2 also revealed abnormally enhancing and enlarged cervical and lumbosacral nerve roots. These findings have been reported in neurofibromatosis type 1, hereditary motor and sensory neuropathy type 1, and now ENS. Both neurofibromatosis type 1 and hereditary motor sensory neuropathy type 1 have been linked to an abnormality on chromosome 17 (12). The presence of skeletal dysplasia and an infiltrative soft-tissue mass in this patient had many similarities to abnormalities commonly seen in neurofibromatosis type 1. The overlapping features of ENS and neurofibromatosis 1 in this patient may be the result of similar chromosomal aberrations. Chromosomal studies were not performed in either patient.
Conclusion
In the future, neuroimaging examination of patients with ENS should include an evaluation of the brain and entire spine. Careful assessment of the cerebral cortex is required to detect subtle cortical dysplasia. MR imaging of the spine is recommended, even in asymptomatic patients. The presence of abnormalities may confirm the diagnosis in a patient with minimal or no intracranial abnormalities. Imaging the spine in cases of ENS will allow further characterization of the spectrum of spinal abnormalities. This additional information may establish more concrete links between ENS and other neurocutaneous syndromes.
Footnotes
Presented at the 39th annual meeting of the American Society of Neuroradiology, Boston, MA, 2001.
References
- Received March 21, 2002.
- Accepted after revision June 5, 2002.
- Copyright © American Society of Neuroradiology