Abstract
BACKGROUND AND PURPOSE: Surgically or conservatively treated brain abscesses may resolve, or pus may re-accumulate, requiring further intervention or treatment change. We hypothesized that diffusion-weighted (DW) imaging is useful in depicting features of abscesses related to therapeutic success or failure.
METHODS: Conventional contrast-enhanced T1- and T2-weighted imaging and DW imaging were performed in seven patients (aged 30–69 years) with proved pyogenic brain abscesses. The center of the abscess was qualitatively and quantitatively analyzed at initial and follow-up imaging in all patients. We correlated the signal intensity on trace DW images and the apparent diffusion coefficients (ADCs) with the clinical and laboratory data, particularly with respect to treatment failure and repeat therapy.
RESULTS: Surgical drainage was performed in six patients; one patient was treated with only antibiotics. All abscess cavities initially had high signal intensity (restricted diffusion) on DW images, with a mean ADC value of 0.52 × 10 −3mm 2/s. Low signal intensity at DW imaging with high ADC were seen on follow-up images in the patient receiving medication and in four patients in whom the abscesses were drained; this correlated with a good therapeutic response. Two patients underwent drainage; their second follow-up DW images showed areas of high signal intensity and low ADC values suggesting re-accumulation of pus. Increased C-reactive protein level and WBC count correlated well with DW image findings.
CONCLUSION: DW imaging was superior to conventional MR imaging in evaluating the success or failure of abscess therapy. Restricted diffusion in a drained abscess corresponded to pus.
The typical appearance of a brain abscess at conventional MR imaging is that of a ring-enhancing lesion, with high signal intensity on T2-weighted images and low or intermediate signal intensity on T1-weighted images. A mature abscess has a low-signal-intensity capsule on T2-weighted images (1).
However, the presence of a ring-enhancing lesion in the brain is not diagnostic of abscess and must be distinguished from a necrotic neoplasm and other cystic lesions. Data from recent studies suggest that diffusion-weighted (DW) imaging is more sensitive than conventional MR imaging in distinguishing brain abscesses and cystic tumors (2–8). Pus in brain abscesses is strongly hyperintense on trace DW images and has a reduced apparent diffusion coefficient (ADC). On the contrary, most necrotic or cystic brain tumors have intermediate signal intensity on DW images and elevated ADC values (2–10).
The management of brain abscesses varies. CT-guided stereotactic aspiration followed by intravenous antibiotic therapy is the favored treatment for solitary and multiple brain abscesses, but other abscesses may be treated with only antibiotics. Because treatment failure has considerable prognostic implications, early detection of pus re-accumulation is desirable. Unfortunately, laboratory parameters that measure inflammatory responses may lag behind actual relapse of the abscess.
We hypothesized that DW imaging is useful in the post-treatment follow-up of abscesses, as it depicts imaging features related to the success or failure of therapy.
Methods
Subjects
Seven patients with brain abscesses were prospectively enrolled in this study. The four men and three women had a mean age of 42.8 years (range, 30–69 years). Clinical signs, symptoms, and results of their laboratory tests are summarized in Table 1.. In six patients, stereotactic surgical drainage of the abscess cavities was performed, followed by intravenous antibiotics. Two of these patients underwent two surgical interventions. In one patient, the brain abscess was treated with antibiotics only.
Clinical signs and symptoms and laboratory results
MR Imaging Examinations
Brain MR imaging was performed by using clinical 1.5-T systems in two institutions. The following were performed in all patients: 2-mm coronal T2-weighted sequence (TR/TE/NEX,4000/90/1), 4-mm axial fluid-attenuated inversion recovery sequence (FLAIR; TR/TE/TI, 11000/80/2800), and axial 1.25-mm gradient-echo T1-weighted sequence (20/1.76/1; flip angle, 35 ο) before and after gadolinium administration.
A single-shot, multisection, spin-echo echo-planar pulse sequence (TR/TE, 4116/89) was used for DW imaging. We collected DW images in three directions (x, y, and z) with b values of 0, 500 and 1000 s/mm 2, a field of view of 230 mm, a matrix of 128 × 128 or 256 × 256, and an acquisition time of 34 seconds. ADC maps were generated from the DW image datasets. First, we qualitatively evaluated the signal intensity from the abscess cavity on the trace DW image and then, round regions of interest were drawn manually; these were placed entirely within the abscess cavities and also in normal-appearing brain regions contralateral to the abscesses. ADC values were recorded from the baseline pretherapeutic studies and on all follow-up studies obtained during treatment. ADC ratios were calculated as the ratio of the mean ADC in the lesion to the mean ADC in normal white matter. On all follow-up MR imaging studies, we also qualitatively evaluated the appearance of the lesions (ie, signal intensity, size, pattern of enhancement, degree of surrounding edema) for any finding that suggested treatment failure (as evidenced by an increase in any of these parameters).
Clinical Examinations
All patients underwent neurologic and laboratory examinations for baseline values and during therapy on a daily and biweekly basis during 4-week intravenous antibiotic treatments. Afterward, patients received oral antibiotics for 4 weeks and were monitored weekly on an outpatient basis for indications of treatment failure.
Results
MR Imaging Findings
Five patients had one lesion, and two patients had multiple lesions. The mean diameter of the abscesses was 2.87 cm (range, 1.1–4.0 cm). Table 1 lists their locations. On T2-weighted images, all lesions showed central high signal intensity with capsules of low signal intensity. T1-weighted images showed central low-to-intermediate signal intensity in all lesions. On FLAIR images, the abscesses were isointense relative to gray matter. Perilesional edema and mass effect were always present. Contrast-enhanced T1-weighted images showed ring enhancement in all lesions consistent with mature cerebral abscesses. All follow-up images were obtained on a weekly basis. One patient underwent six follow-up imaging studies; one, five; one, four; and three, three. In four patients, follow-up MR images showed that the central signal intensity of the abscesses did not change with any sequence. The degree of mass effect, surrounding edema, and contrast enhancement decreased slightly but did not change substantially compared with the respective features on pretreatment studies. In three of these patients, therapy was successful; in one, therapy failed. In another patient, the abscesses mildly increased in size; this change corresponded to the clinical failure of treatment.
DW Findings
Table 2 summarizes the signal intensities of the lesions on DW images and the measured ADC values on initial and subsequent MR images in the six patients who underwent surgical drainage.
Signal intensities on DWI and ADC values
On initial DW imaging studies, all brain abscesses showed central high signal intensity, and low ADC values (mean, 0.52 × 10 −3 mm 2/s; range, 0.36–0.75 × 10 −3mm 2/s) indicating restricted diffusion. In patients 1, 6, and 7, who underwent surgical intervention, first follow-up trace DW images showed low signal intensity, and mean ADC values increased (from 0.47 × 10 −3 to 1.15 × 10 −3 mm 2/s). Subsequent follow-up demonstrated further increase in ADC and low signal intensity on DW images (Figs 1 and 2).

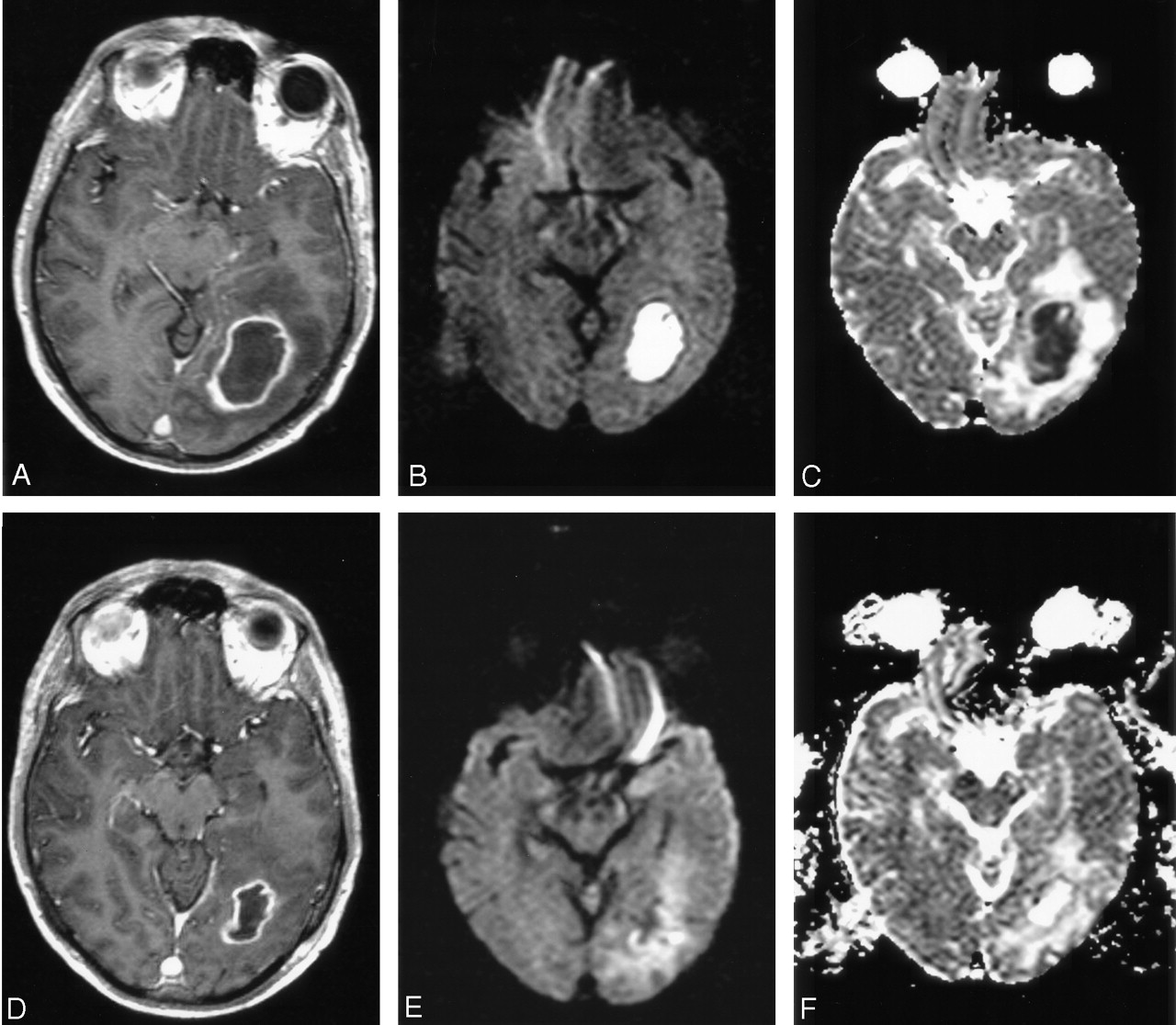
Patient 1. A 40-year-old man with mild ataxia and homonymous hemianopia. CRP level was initially 0.5 mg/dL and did not change in the clinical course. WBC count was mildly increased initially and decreased soon after surgical drainage. DW images were well correlated with conventional MR images, showing no re-accumulation of pus.
A, Axial contrast-enhanced T1-weighted image shows a ring-enhancing lesion in the left occipital region, with perifocal edema.
B and C, Trace DW images show a hyperintense lesion and a low ADC indicating restricted diffusion. Clinical and imaging findings were consistent with brain abscess.
D–F, Four days after surgical drainage, contrast-enhanced T1-weighted image (D) shows that the lesion is diminished, with predominantly low signal intensity on a DW image (E) and a high ADC on ADC map (F); these finding suggest clear fluid in the abscess cavity.

Patient 1. Additional images.
A–C, Follow-up images obtained 9 days later (2 weeks after drainage) show further decrease in the size of the abscess (A), persistence of low signal intensity on DW imaging (B), and a high ADC (C).
D-F, Last DW images (E) (1 month after drainage) show no enhancement and no abnormality.
Patient 3 had two lesions, one that was surgically drained and showed low signal intensity on trace images and increased ADC (from 0.53 × 10 −3 to 0.81 × 10 −3 mm 2/s) at first follow-up. The second lesion was not aspirated and showed increased ADC (from 0.81 × 10 −3 to 2.76 × 10 −3 mm 2/s) at first follow-up. At second follow-up, the abscess that was not drained increased in size and showed a decrease in ADC value (from 1.12 × 10 −3 to 0.46 × 10 −3 mm 2/s); this finding suggested the persistence of purulent fluid and an insufficient therapeutic response to antibiotics. This abscess was not drained, but the antibiotics were changed.
In patients 2 and 5, first follow-up images obtained after drainage showed decreased mean ADC in the abscess cavity (from 0.5 × 10 −3 to 2.75 × 10 −3 mm 2/s). At second follow-up in patient 2 (13 days after surgical drainage), trace DW images showed increased signal intensity, and ADC decrease (from 2.56 × 10 −3to 1.16 × 10 −3 mm 2/s) was documented (Figs 3 and 4). Surgical drainage was repeated; the findings confirmed the presence of pus. Subsequent images (7 days after the second intervention) showed persistence of high signal intensity on trace DW images and a further decrease in ADC value (0.76 × 10 −3 mm 2/s). After a change in antibiotics, a follow-up image obtained 11 days after second drainage showed an increase in ADC (1.17 × 10 −3 mm 2/s) and low signal intensity on trace DW images, suggesting improvement. In patient 5, third follow-up studies showed high signal intensity on DW images and decreased ADC, suggesting relapse of purulent fluid. After repeat intervention, follow-up MR study showed low signal intensity on DW images and an increase in ADC value.

Patient 2. A 31-year-old man with fever, seizures, and weakness of the left upper extremity. DW images were superior to conventional MR images showing re-accumulation of pus and well correlated with increased CRP levels and WBC counts.
A–C, Axial contrast-enhanced T1-weighted shows a peripheral enhancing lesion with a hypointense center in the right parietal region. Hyperintensity at DW imaging (B) and a low ADC (C) suggest abscess formation with restricted diffusion due to pus.
D–F, One day after surgery, images show decreased size of the abscess (D), hypointensity at DW imaging (E), and a high ADC of 2.56 × 10 −3mm 2/s (F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient 2. Additional MR images.
A–C, Follow-up image (A) obtained 15 days after surgical intervention shows reduced size of the abscess cavity. Corresponding DW image (B) shows hyperintensity in the abscess cavity with a decreased ADC to 0.76 × 10 −3mm 2/s (C), indicating reappearance of pus. Second drainage was performed 1 day later.
D–F, Forty days after second intervention, follow-up images show resolution of the abscess cavity, with residual hypointensity on contrast-enhanced T1-weighted image and no abnormality on DW images.
In patient 4, who was treated with antibiotics only, the first and all subsequent trace DW images demonstrated low signal intensity, with a corresponding increase in ADC. These findings suggested no pus and, therefore, a good therapeutic response.
Clinical Findings
Six patients initially underwent surgical drainage of the abscesses. One procedure was done via open craniotomy, and five, with stereotactic guidance. After the pus was drained, all cavities were washed with artificial CSF solution containing vancomycin. In three patients, pathogens were established (S intermedius, S aureus, Nocardia species, and P nigros). In three other patients, cultures grew no organisms. In the patient who did not undergo surgical drainage, findings of multiple blood cultures were negative, and the abscess was conservatively treated on an empirical basis. All patients received combination intravenous antibiotics for 4 weeks followed by oral antibiotics for 4 weeks. Patients 2 and 5 underwent second surgical interventions. In both patients, CRP levels increased, and their clinical symptoms worsened. DW images showed high signal intensity in the abscess cavity, with decreased ADC in both cases. Contrast-enhanced T1-weighted images showed decreased size of the abscesses, with an enhancing capsule. A second aspiration was done on the basis of the DW imaging, clinical, and laboratory findings; pus was recovered from both abscesses.
Discussion
A ring-enhancing lesion in the brain is a nonspecific finding, and a variety of inflammatory and neoplastic processes can have a similar appearance. Moreover, it is important to differentiate between a pyogenic brain abscess and a necrotic neoplasm, as both have different treatments and prognoses.
Several studies have addressed the utility of DW imaging in distinguishing cerebral abscesses from necrotic tumors (2–10). DW imaging is based on the microscopic motion of water molecules and depends mostly on the water located in the extracellular space (11). To quantify the degree of water motion, ADC maps are needed (11). Necrotic material in cerebral abscesses contains inflammatory cells, a matrix of proteins, cellular debris, and bacteria in high-viscosity pus; all of these factors restrict water motion. Additionally, water molecules are bound to amino acid groups on the surface of macromolecules, further restricting their motion. Therefore, restricted water motion in cerebral abscesses has increased signal intensity on trace DW imaging and low ADC values. Conversely, necrotic material in tumors contains cellular debris, serous fluid, and fewer inflammatory cells; thus, water molecules have a greater freedom of motion (12). Most necrotic tumors show mildly increased diffusion with low-to-intermediate signal intensity on trace DW images and high ADC values. In one in vitro study, DW imaging of extracellular purulent and serous fluids was performed (13). ADC values of serous fluids were close to those of free water, whereas ADC values for purulent fluids were significantly lower.
In 1996 Ebisu et al (14) reported restricted diffusion in a cerebral abscess. Guo et al (3) confirmed these DW findings in large abscesses while showing that smaller abscesses had nearly normal ADC values. A possible explanation for this observation is that the small size leads to difficulties in region-of-interest positioning and ADC measurements. Another explanation is that the content of small abscesses results in a normal rate of water diffusion. Other investigators (4) have suggested that variable concentrations of inflammatory cells and bacteria are present with different pathogenic organisms and that the host immune response and the age of an abscess might influence the viscosity of the pus, resulting in variations in ADC values. In our patients, all abscess cavities initially had high signal intensity on trace DW images and low ADC values consistent with restricted diffusion.
After the first optimistic reports about using DW imaging to distinguish brain abscesses from necrotic neoplasms were published, other studies (14,15) showed that restricted diffusion in a ring-enhancing lesion might be characteristic but not pathognomonic of brain abscess. Hartmann et al (16) found restricted diffusion in one metastatic adenocarcinoma and unrestricted diffusion in one postoperative abscess cavity. The reasons for restricted diffusion in this particular metastasis remain unclear. Possible explanations for high signal intensity on trace DW images of processes other than pyogenic brain abscess include high cellularity and reduced extracellular space, as seen in lymphomas and medulloblastomas (16). In two cases of lymphoma, restricted diffusion was demonstrated as high signal intensity on trace DW images and low ADC (16). Tung et al ( 15) reported restricted diffusion in two cases of metastases and in one case of radiation necrosis. Hemorrhagic metastasis had high signal intensity on DW images in another report (17).
After a cerebral abscess is diagnosed, the decision for surgical versus medical treatment is made immediately. However, the management of brain abscesses remains somewhat controversial, mainly because of discordant results from studies in small patient groups. CT-guided stereotactic aspiration of brain abscesses is minimally invasive, it results in minimal morbidity and mortality, and it is currently a valid alternative to the traditional surgical methods (18). Published results indicate a combined surgical and medical approach is optimal for the treatment of brain abscesses (19). Most authors advocate aspiration of small solitary abscesses for diagnostic purposes, followed by a 6–8-week course of intravenous antibiotics and surgical drainage of all abscesses larger than 2.5 cm in diameter and combined with 6–8 weeks of intravenous antibiotics (20). CT scanning or MR imaging performed biweekly or with any sign of clinical deterioration is needed to closely monitor for evidence of abscess growth or treatment failure that prompts another intervention. This imaging interval is based on the results of a study of 102 patients with brain abscesses that were monitored with weekly CT scans (21). Abscess size substantially decreased at a mean of 2.1 weeks after the initiation of therapy. The resolution of ring enhancement and the disappearance of the low-signal-intensity capsule on T2-weighted images indicate a sufficient therapeutic response. Repeated surgical drainage is recommended if an abscess enlarges after 2 weeks of antibiotic therapy or if it fails to resolve after 3–4 weeks of antibiotic treatment. In one study, 43 surgical procedures were performed in 13 patients, eight (62%) of whom required more than one surgical procedure (20). Therefore, treatment failure is not unusual.
To our knowledge, no published reports have described DW image findings of treated brain abscesses or their appearance on follow-up DW images. All surgically drained abscesses in our study showed a signal intensity change on trace DW images at first follow-up study. They changed from initial high signal intensity to low signal intensity, indicating the disappearance of purulent content. In one patient who was treated with only medication, follow-up DW images and MR images showed similar changes, indicating a good therapeutic response. Our study clearly showed the value of DW imaging in the surveillance of therapy for brain abscesses; two abscesses showed persistent high signal intensity on trace images and low ADC values suggesting the presence of pus despite therapy (one treated surgically, and one treated with medication only). Laboratory parameters were well correlated with these imaging findings (and also in patients whose findings showed unrestricted diffusion in the cavities of successfully treated abscesses).
The imaging, clinical, and laboratory findings altered patient care. In two patients in whom DW images suggested re-accumulation of pus, a second surgical intervention was performed and confirmed the presence of pus. With contrast-enhanced T1-weighted imaging, the differentiation of purulent fluid from serous fluid inside the abscess cavity is not possible. On visual inspection of the postcontrast T1-weighted images in these patients with relapse, the decrease in size of the abscess cavities suggested a good therapeutic response, but this was not the case. In one patient, the size of the abscess remained stable, and in the other, growth was observed. In a partially treated cavity, the continuous accumulation of a substantial amount of pus might be necessary before the abscess enlarges again.
Limitations of our investigation include the small number of patients; therefore, our imaging findings and conclusions should be interpreted as preliminary and subject to further investigation. Additionally we cannot exclude the possibility that postsurgical blood and antibiotic solution in the abscess cavities may alter their signal intensity on DW images. However, blood products and the free water and antibiotic-containing solutions should result in lower signal intensity on DW images and not restricted diffusion. Therefore, it is also possible that magnetic susceptibility effects of blood might have obscured a small amount of residual pus in the immediate postdrainage period, resulting in signal intensity loss. This would have resulted in the loss of signal intensity on trace DW images and ADC maps, an appearance not seen in any of our patients. With regard to follow-up intervals, weekly MR imaging studies are indicated during antibiotic therapy and in the week afterward (or sooner if the patients experience clinical deterioration).
Conclusion
Our preliminary experience indicates that trace DW imaging and ADC maps are useful in the post-treatment follow-up of brain abscesses. Decreased signal intensity on trace DW images and increasing ADC values in the abscess cavity correlated with successful treatment. Conversely, persisting or reappearing high signal intensity in the abscess cavity on trace DW images and low ADC values indicating restricted diffusion were seen in cases of treatment failure and were correlated with pus re-accumulation. Findings in successfully and unsuccessfully treated brain abscesses were similar on conventional MR images and did not allow for their differentiation; therefore, we believe that DW imaging may play an important role in evaluating treated brain abscess. Further studies with a larger number of abscesses managed with ongoing medical or surgical therapy and imaged in different stages are needed to make solid conclusions. The degree of viscosity, the causative organism, and the level of protein in the abscess cavity may affect DW image findings and ADC values.
References
- Received December 30, 2003.
- Accepted after revision March 12, 2004.
- Copyright © American Society of Neuroradiology