Abstract
Summary: Dural sinus malformation is an extremely rare congenital cerebrovascular malformation. We report serial antenatal sonographic findings in two patients with dural sinus malformation. Sonography can reveal dural sinus malformation at 24 weeks’ gestation. Correct and early diagnosis may help determine the appropriate place, timing, and mode of delivery, which may result in a better therapeutic course and patient outcome.
Congenital cerebrovascular malformations, which can be diagnosed antenatally, are either dural sinus malformations (DSMs) or vein of Galen aneurysmal malformations (VGAMs) (1, 2). DSM is an extremely rare congenital cerebrovascular malformation with dural arteriovenous fistula and a huge dural lake, which is rarer than VGAM (1–3). The huge dural lake is usually located at the transverse sinus, superior sagittal sinus, or torcular herophili. We report two cases of DSM that were diagnosed on the basis of antenatal sonography findings and confirmed subsequently by use of cerebral conventional angiography. The clinical significance of antenatal sonographic diagnosis of DSM is discussed.
Case Reports
Case 1
A 27-year-old woman (gravid 1, para 0) was referred to our hospital after sonography (SONOVISTA-if, MEU-1590; Mochida Pharmaceutical, Tokyo) revealed an intracranial vascular lesion in the fetus (gestational age [GA], 35 weeks 6 days) (Fig 1). The patient’s medical history was unremarkable, and her husband was also healthy and without any remarkable medical history. Antenatal MR imaging at GA 37 weeks 5 days showed a large signal intensity void in the posterior portion of the brain (Fig 1D). Because sonography showed cardiomegaly, tricuspid regurgitation, and enlarged neck veins, indicating cardiac failure in utero, caesarean section was performed under spinal anesthesia at GA 38 weeks 6 days. A boy was born with a birth weight of 2801 g. Apgar scores were 4 at 1 minute and 9 at 5 minutes. In retrospect, sonography had shown an abnormal cystic lesion as early as GA 23 weeks 6 days (Fig 1C).

{kind=link}
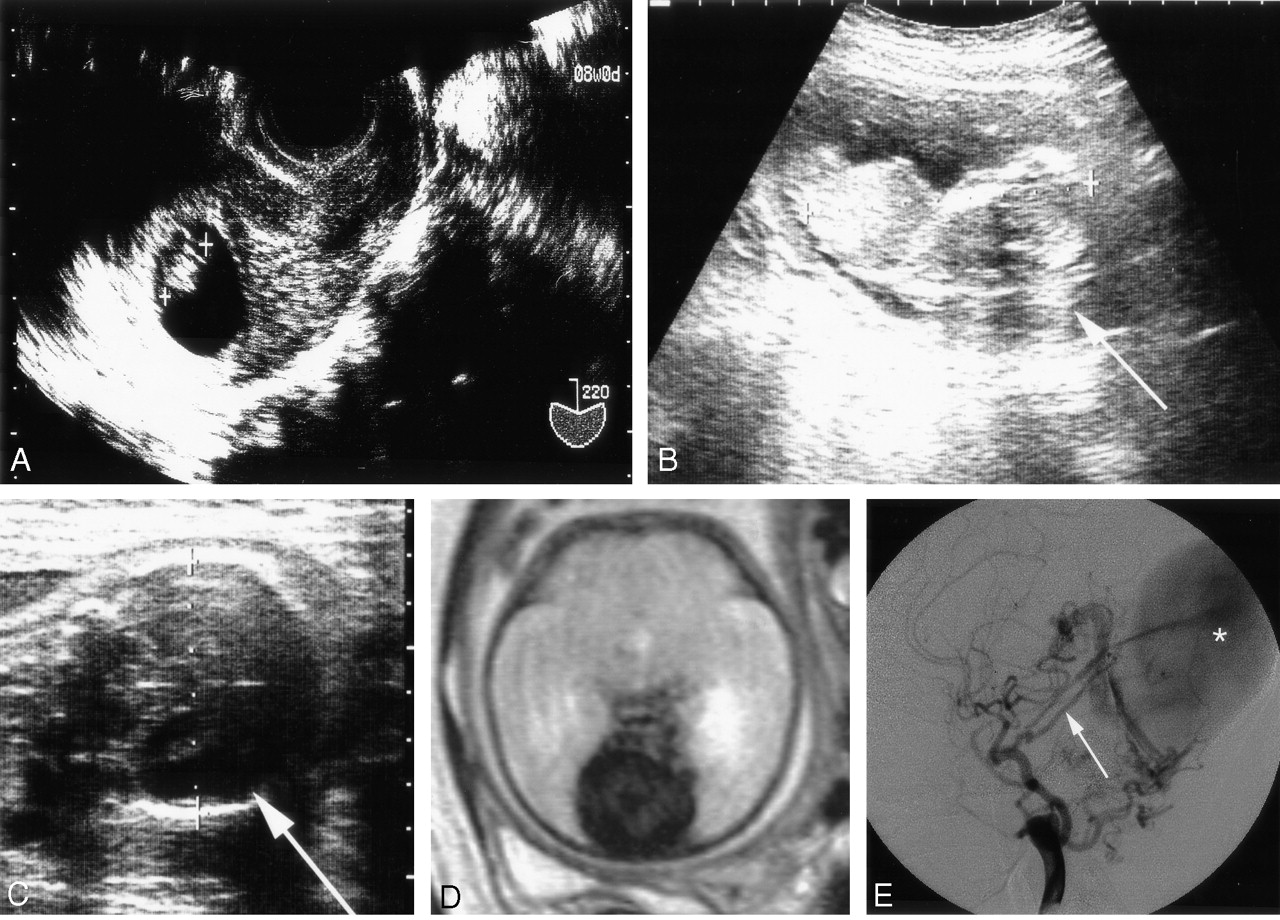
Case 1. Serial sonographic images, an MR image, and an angiogram show a DSM.
A, Transvaginal sonogram at GA 8 weeks shows the 15-mm-long fetus.
B, Sonogram at GA15 weeks 5 days. Arrow indicates the head. Crown-rump length is 87 mm.
C, Sonogram at GA 23 weeks 6 days definitively shows a huge cystic lesion (arrow).
D, MR image at GA 37 weeks 5 days shows a huge dural lake in the posterior fossa with signal intensity void.
E, Right common carotid angiography (lateral view) shows a dural lake (asterisk) fed by tentorial artery (arrow), middle meningeal artery, and occipital artery.
Except for cardiac failure and bruits heard over the cervical and occipital regions, the neonate was neurologically normal. CT performed the day after birth did not show brain damage or hydrocephalus. Digital subtraction angiography showed that the main feeding arteries were bilateral middle meningeal arteries, occipital arteries, tentorial arteries, cerebellar arteries, and a huge dural lake at the torcular herophili, confirming the diagnosis of DSM (Fig 1E). Because of progressive heart failure, the patient underwent four sessions of endovascular treatment on postnatal days 4, 10, 12, and 17. This patient was 5 years old at last follow-up and had moderate developmental delay (developmental quotient, 67).
Case 2
A 30-year-old healthy woman (gravid 1, para 0) was referred to us for a complicated pregnancy at GA 36 weeks 4 days. Her medical history was unremarkable. Her husband was also healthy without any remarkable medical history. A local obstetrician performed regular biweekly sonographic examinations from GA 5 weeks onward. At GA 24 weeks, an intracranial mass lesion was detected, which was not detected at the examination 2 weeks earlier. At GA 27 weeks, MR imaging revealed the huge space-occupying lesion in the left posterior cerebral hemisphere, which was interpreted as a brain tumor in a local hospital. The patient was referred to us for the management of the delivery. We interpreted the previous sonography and MR images as showing a DSM, not a brain tumor.
At GA 36 weeks 4 days, because of cardiac failure in utero, the neonatal boy was delivered by elective caesarian section under spinal anesthesia. Birth weight was 2135 grams. Apgar scores were 1 at 1 minute and 7 at 5 minutes. The neonate required immediate endotracheal intubation and mechanical ventilation. Conventional angiography confirmed the diagnosis of DSM with feeding arteries of bilateral middle meningeal arteries and occipital arteries, left anterior and middle cerebral arteries, and a huge dural lake in the left parietooccipital region. The patient underwent four sessions of endovascular treatment on days 1, 7, 23, and 42 for severe heart and respiratory failure. The patient’s general condition improved markedly with these embolizations. The patient underwent ventriculo-peritoneal shunt for hydrocephalus at 8 months and had minimal right hemiparesis and moderate developmental delay (developmental quotient, 59) at the last follow-up at 1 year.
Discussion
Sonography is the imaging technique of choice for the assessment of fetal abnormalities and allows serial noninvasive observation of the lesion and associated changes. Color Doppler imaging is especially useful for the detection of blood flow in the lesion; however, until GA 7 weeks, the brain cannot be well recognized by the sonographic technology currently in use. Major diseases of the brain can be diagnosed starting at GA 12–13 weeks by using transvaginal scanning (4).
VGAM is demonstrated as a posterior, midline supratentorial lesion with round or ovoid shape. Sonographic findings of DSM include a huge cystic structure, which is attached to the dura mater, with turbulent blood flow. Blood flow in DSMs is generally slower than that of VGAMs (5). The DSM has not been emphasized so far, simply because of its rarity (3, 6). The concept that all antenatally diagnosed cerebral vascular lesions are VGAMs is incorrect and should be revised, and a DSM should be included in the differential diagnosis. Lack of knowledge of DSMs might result in failure of proper recognition of the lesions, as happened in our cases. The midline lesion such as that in case 1 was misdiagnosed as a VGAM, and a laterally located lesion such as that in case 2 was regarded as multicystic brain tumor. Differentiation between a VGAM and DSM is possible because of the comparative locations of the lesions.
Diagnosis of the cerebral arteriovenous shunts in utero is established in the third trimester in most cases, and rarely, in the second trimester (3, 7, 8). Ballester et al (9) reported the earliest antenatal sonographic diagnosis of VGAM at GA 25 weeks, and the fetus died in utero at GA 28 weeks because of severe progressive heart failure. Ximenes et al (10) also reported a fetus with normal sonographic findings at GA 16 weeks, but a VGAM was detected at GA 25 weeks. Ordorica et al (11) reported a fetal VGAM diagnosed at GA 27 weeks. Worswick et al (12) described a case in which sonographic findings were normal at GA 18 weeks but in which VGAM was discovered at GA 29 weeks. These reports show that VGAM can be diagnosed as early as GA 25 weeks, and heart failure commonly deteriorates along with the progression of pregnancy.
Lee et al (13) reported a “fetal arteriovenous malformation with atypical presentation,” which was diagnosed by sonographic examination because of cystic lesion in the frontoparietal region at GA 23.5 weeks. The pregnancy was terminated, and autopsy showed a normal vein of Galen and a large “arteriovenous malformation” with markedly dilated superior sagittal and transverse sinuses. Comstock and Kirk (7) reported a fetus that had normal sonographic images at 20 weeks, but a 5-cm frontoparietal lesion was detected at GA 34 weeks. This fetus died of heart failure soon after birth. Although these authors (7, 13) did not specify the angioarchitecture of the lesions, their reported cases were possibly DSMs.
In light of the embryology (14, 15), the pathologic process may begin earlier in VGAMs than in DSMs. Sonographic detection in utero of these two diseases, however, may take place in a different order. In our series, a DSM could be diagnosed as early as GA 23 weeks 6 days. This means that both DSMs and VGAMs become apparent as early as GA 24–25 weeks.
Conclusion
When proper diagnosis of a DSM or VGAM is established, strict sonographic monitoring of the size of the lesion, flow in the lesion, size of the head, and cardiac status is necessary. Although no recommended mode of delivery exists, elective caesarian section is recommended instead of spontaneous vaginal delivery in case of macrocrania or hydrocephalus. Neonatal care should start immediately after delivery. Early diagnosis may allow counseling of the upset parents when they are informed that a fetus has a congenital cerebrovascular lesion with a grave prognosis (7).
References
- Received July 24, 2003.
- Accepted after revision January 14, 2004.
- Copyright © American Society of Neuroradiology