Abstract
BACKGROUND AND PURPOSE: Apolipoprotein E (apoE) genotype plays an important role in the development, maintenance, and response to injury of the central nervous system. It has been suggested that apoE ε4 genotype is a risk factor for several neurologic disorders. We investigated the correlation between the apoE genotype and radiologic data in patients with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
METHODS: T1-weighted, dual fast spin-echo, T2*-weighted gradient echo, and fluid-attenuated inversion recovery MR imaging scans were obtained from 36 CADASIL patients (21–59 years of age). The number of lacunar infarcts and microbleeds and the presence of subcortical lacunar lesions were determined. The amount of white matter hyperintensities was assessed by using semiautomated segmentation software. The relation between the radiologic endophenotype of CADASIL and the apoE genotype was assessed by using a Student t test for unpaired data and Fisher exact test.
RESULTS: White matter hyperintensities, lacunar infarcts, microbleeds, and subcortical lacunar lesions were not found to be associated with the presence of an ε4 allele.
CONCLUSION: The variability of structural MR imaging lesions in CADASIL is independent of apoE genotype and other processes must underlie the variable natural history of the disease.
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a hereditary small-artery vasculopathy caused by mutations in the notch3 gene on chromosome 19.1 The disease is clinically characterized by transient ischemic attacks, strokes, progressive subcortical dementia, migraine with aura, and mood disturbances. In general, death follows at an age of 55–65 years after a mean disease duration of 20 years.2 MR imaging findings in CADASIL are present in symptomatic, as well as asymptomatic, mutation carriers and consist of diffuse white matter hyperintensities (predominantly in the subcortical areas) and lacunar infarcts (in the centrum semiovale, thalamus, basal ganglia, and pons). Recent MR imaging studies have established microbleeds and subcortical lacunar lesions as additional radiologic features of CADASIL.3
The phenotypic and radiologic expression of CADASIL is variable, both between and within families. The mean age of onset is in the late 30s to early 40s, with a wide range. Some individuals develop microbleeds and subcortical infarcts, whereas others do not. On MR imaging, the extent of white matter hyperintensities and lacunar infarction is variable. This suggests modulation by additional genetic and/or environmental factors. We postulated that the apolipoprotein E (apoE) gene is a candidate genetic modifier in CADASIL.
apoE is a glycoprotein that transports cholesterol and other lipids.4 The apoE gene is located on chromosome 19 and has ε2, ε3, and ε4 alleles. It has been suggested that apoE-dependent uptake of lipoproteins may play an important role in the development, maintenance, and response to injury of the central nervous system.5 In recent studies, the apoE ε4 genotype has been consistently associated with severe neurodegeneration and seems to constitute a risk factor for several neurologic disorders. The ε4 allele has turned out to be a major risk factor for Alzheimer disease and lobar hemorrhages caused by amyloid angiopathy.6 Adverse recovery after head trauma or other injury of the brain has also been linked to the ε4 allele.5
The aim of this study was to assess whether the radiologic endophenotype of CADASIL is correlated to the apoE genotype. We hypothesized that ε4 allele carriers have more white matter hyperintensities, lacunar infarcts, microbleeds, and subcortical lacunar lesions than those with the ε2 and ε3 genotype.
Methods
Patients
Members of 15 unrelated CADASIL families were asked to participate in a study on the clinical, radiologic, and genetic aspects of CADASIL. In each family, the index patient had a proved notch3 mutation. Patients were referred from various medical centers to our institution, which serves as a CADASIL referral center. Patients were referred with the suspicion of CADASIL on the basis of clinical signs and symptoms, a family history consistent with autosomal dominant inheritance, or suggestive MR imaging changes. The diagnosis CADASIL was confirmed by direct sequencing analysis of the notch3 gene, according to techniques described elsewhere.7
A total of 36 DNA-confirmed CADASIL mutation carriers were studied (19 women and 17 men, 21–59 years of age; mean age, 45 years). Symptomatic as well as asymptomatic mutation carriers were included. ApoE genotype in all mutation carriers was determined as described by Haan et al.8
MR Imaging
MR imaging was performed in all mutation carriers. All MR imaging examinations were performed on a 1.5T MR system (Philips Medical Systems, Best, the Netherlands). T1-weighted spin-echo images (section thickness, 6 mm, with a 0.6-mm intersection gap [6/0.6 mm]; repetition time [TR]/echo time [TE], 600/20 milliseconds; matrix, 256 × 205; and a field of view [FOV], 220 × 165 mm), dual T2-weighted fast spin-echo (FSE) images (3.0/0.0 mm; TR/TE, 3000/27/120 milliseconds; matrix, 256 × 205; FOV, 220 × 220 mm), T2*-weighted gradient echo-planar (EPI) sequence (6/0.6 mm; TR/TE, 2598/48 milliseconds; matrix, 256 × 192; FOV, 220 × 198 mm; EPI factor, 25), and fast fluid-attenuated inversion recovery (FLAIR) images (3.0/0.0 mm; TR/TE, 8000/100 milliseconds; inversion time, 2000 milliseconds; matrix, 256 × 192; FOV, 220 × 176 mm) were obtained in the axial plane parallel to the inferior border of the genu and splenium of the corpus callosum.
White matter hyperintensities were defined as white matter areas with increased signal intensity as compared with the surrounding white matter on T2, proton attenuation–weighted, and FLAIR images (Fig 1). The amount of white matter hyperintensities was assessed by using semiautomated segmentation software (Department of Radiology, Division of Image Processing, Leiden University Medical Center, Leiden, the Netherlands). Volume of white matter hyperintensities was corrected for total brain volume by dividing the individual volume of white matter hyperintensities by intracranial volume and expressed in percent.

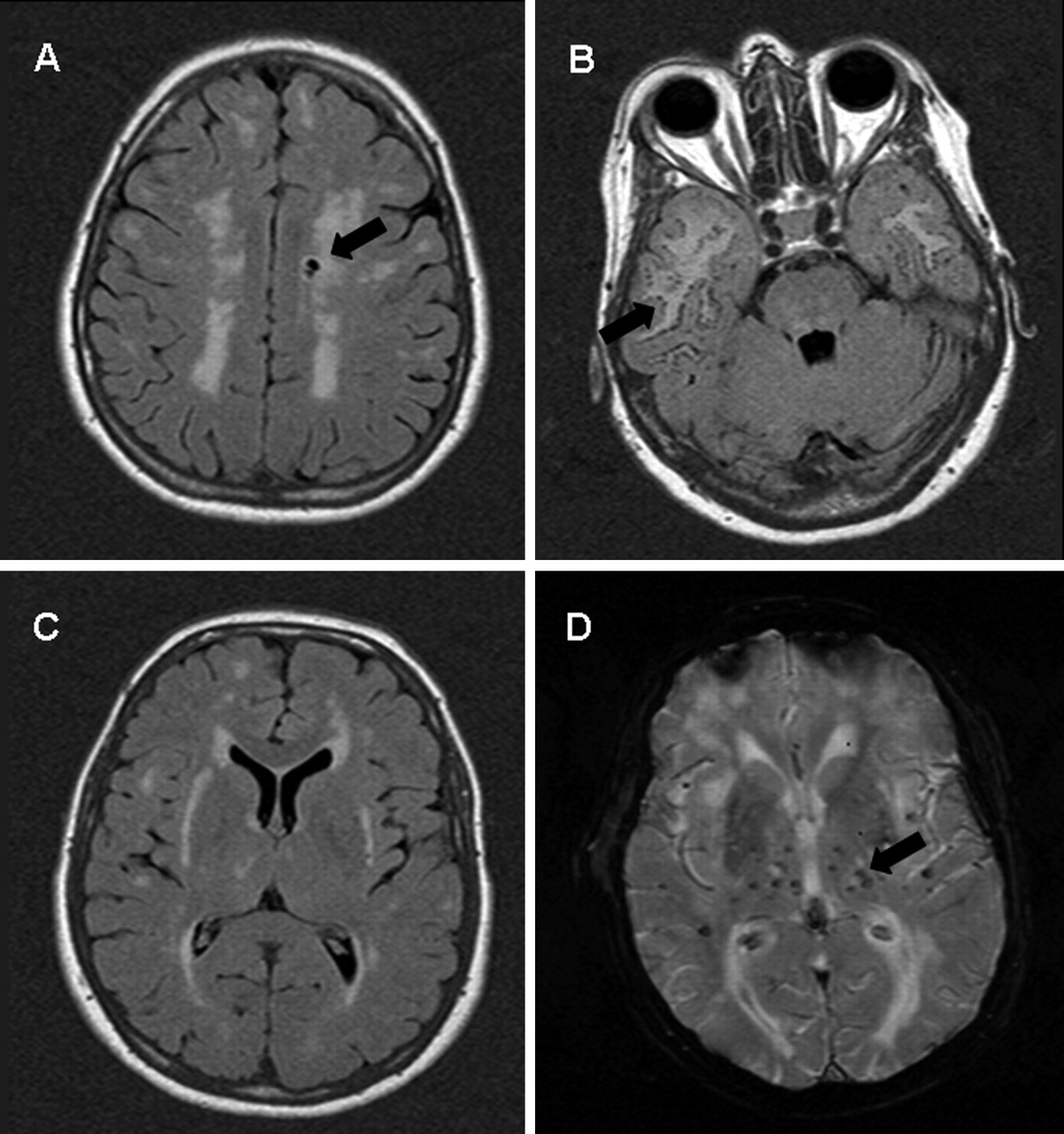{kind=link}
Axial FLAIR (A–C) and T2*-weighted gradient (D) MR images of CADASIL patients. Complete MR imaging spectrum of CADASIL: confluent hyperintensities (A–C), lacunar infarcts (A, arrow), subcortical lacunar lesions (B, arrow), and microbleeds (D, arrow).
Lacunar infarcts were defined as parenchymal defects not extending to the cortical gray matter with a signal intensity following that of CSF on all pulse sequences, irrespective of size (Fig 1). In an effort to differentiate lacunar infarcts from dilated perivascular spaces, areas that were isointense to CSF on all pulse sequence and located in the lower third of the corpus striatum, were excluded.9, 10 Subinsular perivascular spaces were differentiated from lacunar infarcts based on Song et al’s description: enlarged perivascular spaces have a feather-like configuration and are isointense to CSF on T2- and T1-weighted images but do not have high signal intensity on FLAIR images.11 In an effort to differentiate perivascular spaces along the perforating arteries from lacunar infarcts, a modification of the descriptive criteria for perivascular spaces as used by Bokura et al was applied: all lesions with a transverse diameter ≤2 mm or with a tubular appearance following the course of perforating arteries were most likely to represent perivascular spaces and were excluded as well.12
Microbleeds were defined as focal areas of signal intensity loss on T2-weighted FSE images that increased in size on the T2*-weighted gradient echo pulse sequence (“blooming effect”).13 In this way, microbleeds were differentiated from areas of signal intensity loss based on vascular flow voids. Areas of symmetric hypointensity of the globus pallidus likely to represent calcification or nonhemorrhagic iron deposits were excluded (Fig 1).3
Subcortical lacunar lesions were defined as linearly arranged groups of rounded, circumscribed lesions just below the cortex, at the gray-white matter junction with a signal intensity that was identical to that of CSF on all pulse sequences (Fig 1).14 One experienced neuroradiologist (M.A.v.B.) assessed the number of lacunar infarcts and microbleeds and the presence of subcortical lacunar lesions. He was blinded to the apoE status.
Only cognitively capable subjects were included into this study to ensure acquisition of informed consent. Informed consent was obtained from all subjects. The medical ethics committee of our institution approved the study protocol.
Statistical Analyses
As subdivision by genotype would reduce the group size and thereby decrease the statistical power too much, we obtained descriptive statistics for the mean volume of white matter hyperintensities, number of lacunar infarcts, number of microbleeds, and presence of subcortical lacunar lesions. Differences in age, white matter hyperintensities, lacunar infarcts, and microbleeds between ε4 allele carriers and non-ε4 allele carriers were then investigated with a Student t test for unpaired data. Differences in subcortical lacunar lesions were tested by using the Fisher exact test. A P value < .05 was considered significant. The statistical package SPSS-10 (SPSS, Inc., Chicago, Ill) was used for data analysis.
Results
Of the 36 mutation carriers studied, 29 had neurologic symptoms, ranging from one transient ischemic attack to multiple strokes and cognitive deficits. Eight were ε4 allele carriers, and 28 had no ε4 allele. The complete distribution of apoE genotype was as follows: ε2/ε3 (n = 1 [3%]); ε3/ε3 (n = 26 [72%]); ε3/ε4 (n = 8 [22%]); ε2/ε2 (n = 1 [3%]); and ε4/ε4 (n = 0).
Results of the MR imaging analysis are shown in the Table. No significant difference was found between the ε4 allele carriers and the non-ε4 allele carriers in age (P = .46), volume of white matter hyperintensities (P = .84), number of infarcts (P = .27), number of microbleeds (P = .58), or subcortical lacunar lesions (P = .66).
MR imaging findings in apoE genotype subgroups
Discussion
There are several studies that address the issue of the considerable variability in the rate of progression and survival between individual CADASIL patients. Evidence suggests that male patients have a shorter survival than female patients.2, 15 One study has systematically compared the influence of different notch3 mutations on the disease phenotype and found no obvious effect of single mutations on the volume of lesions seen on brain MR imaging.16 Other studies focused on the influence of vascular comorbidity including hypertension, smoking, diabetes mellitus, and hypercholesterolemia on phenotype and the development of white matter hyperinstensities and microbleeds.13, 17 No strong genotype-phenotype relationships in CADASIL were found.
In sporadic amyloid angiopathy as well as in Alzheimer disease, the apoE genotype is a strong predictor of the clinical expression of disease and the development of cerebral structural (including vascular) lesions. There are indications that in Alzheimer disease concomitant vascular lesions, such as infarcts, white matter hyperintensities, and hemorrhagic infarcts are associated with the ε4 allele.6 In our CADASIL study population, the ε4 allele frequency was almost the same (22%) as in the general Dutch population (30%), offering the possibility to compare ε4 carriers with noncarriers.18 In our study, the apoE genotype was not significantly associated with structural changes seen on MR imaging, which suggests that, in CADASIL, structural lesions caused by vascular changes are independent of apoE ε4 genotype. It is possible that the vascular effect of apoE genotype observed in other diseases is dependent on amyloid angiopathy.
Our results extend those of an earlier study of Singhal et al, that found no correlation of the apoE genotype with white matter hyperintensities on MR imaging.17 In addition, we observed a lack of correlation between apoE genotype and occurrence of the other radiologic hallmarks of CADASIL: lacunar infarcts, microbleeds, and subcortical lacunar infarcts. In contrast to that study, we used a more extensive MR imaging protocol as an objective measure of disease severity. We believe that clinical parameters, contrary to structural MR imaging lesions, are a less valid measure of the burden of the disease because of superimposed external factors. Furthermore, not all brain lesions produce clinical symptoms.
A potential limitation of our study may be that only patients who were able to understand the informed consent were included and therefore the most severely affected patients might have been excluded. At this end stage of the disease, however, neither the phenotypic nor the radiologic expression of CADASIL differs as much as at a younger age, and we therefore believe that our results are not influenced by excluding these patients.
In conclusion, our population included 36 CADASIL mutation carriers. By using a very rigorous objective measure for the disease burden—namely, the MR imaging-endophenotype, we may conclude that the variability of structural MR imaging lesions in CADASIL patients are independent of apoE ε4 genotype and that other processes such as environmental and other genetic factors must underlie the variable natural history of the disease.
References
- Received April 27, 2005.
- Accepted after revision June 21, 2005.
- Copyright © American Society of Neuroradiology