Abstract
SUMMARY: Extramedullary hematopoiesis is a complication of a number of myeloproliferative disorders. MR imaging of the orbits was performed in a patient with bilateral orbital swelling with known myeloproliferative disorder and myelofibrosis. The study revealed symmetric, bilateral enhancing masses in the lacrimal fossae extending into the nasolacrimal ducts. Biopsy demonstrated sclerotic extramedullary hematopoietic tumor.
Myeloproliferative disorder with myelofibrosis is a hematologic condition characterized by marrow fibrosis that suppresses bone marrow hematopoiesis and displaces hematopoietic elements. It is often accompanied by extramedullary hematopoiesis that can occur in various locations within the body and is characterized by soft tissue masses seen at imaging.1
Case Report
A 60-year-old man with known myeloproliferative disorder with myelofibrosis presented with an 18-month history of progressive orbital swelling with excessive tearing bilaterally. On physical examination, swelling in the bilateral medial orbital regions was noted without erythema. Corresponding nontender fluctuant masses were noted on physical examination. Laboratory results were remarkable for an elevated neutrophil count of 21,000. The patient had undergone prior imaging related to his disorder, which included CT of chest, abdomen, and pelvis (not shown) and sonography of the scrotum (not shown). These studies documented sites of pleural, mediastinal, retroperitoneal, and testicular extramedullary hematopoiesis. Related to this, the patient had also undergone prior orchiectomy.
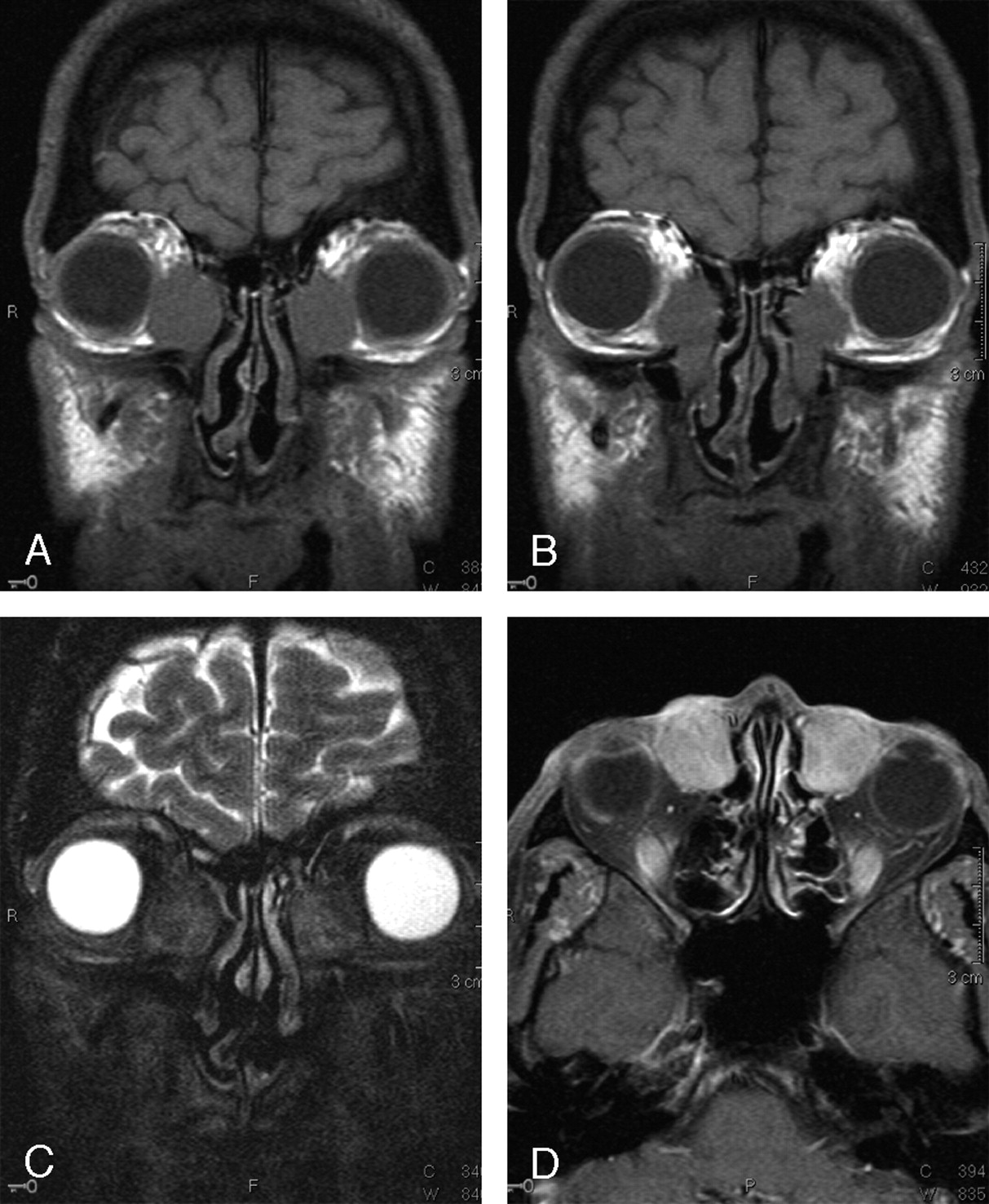
An MR examination of the orbits was obtained that demonstrated symmetric bilateral soft tissue masses centered in the lacrimal fossae, extending into the nasolacrimal ducts. These well-defined lesions were homogeneously hypointense on T1-weighted imaging, heterogeneously hypointense on T2-weighted imaging, and enhanced throughout (Fig 1). Also seen was generalized soft tissue thickening of the eyelids and scalp (not shown). Calvarial and skull base hypointense T1 marrow signal intensity was also noted (not shown).

Coronal T1 (A and B), coronal T2 fat-saturated (C), and axial T1 fat-saturated postgadolinium (D) images of the orbits. Homogeneous, well-defined T1-hypointense masses are seen in the lacrimal fossae bilaterally (A), extending inferiorly into the nasolacrimal ducts (B). These masses are largely hypointense on T2-weighted imaging with heterogeneous areas of hyperintensity (C). Diffuse enhancement is seen after gadolinium administration (D).
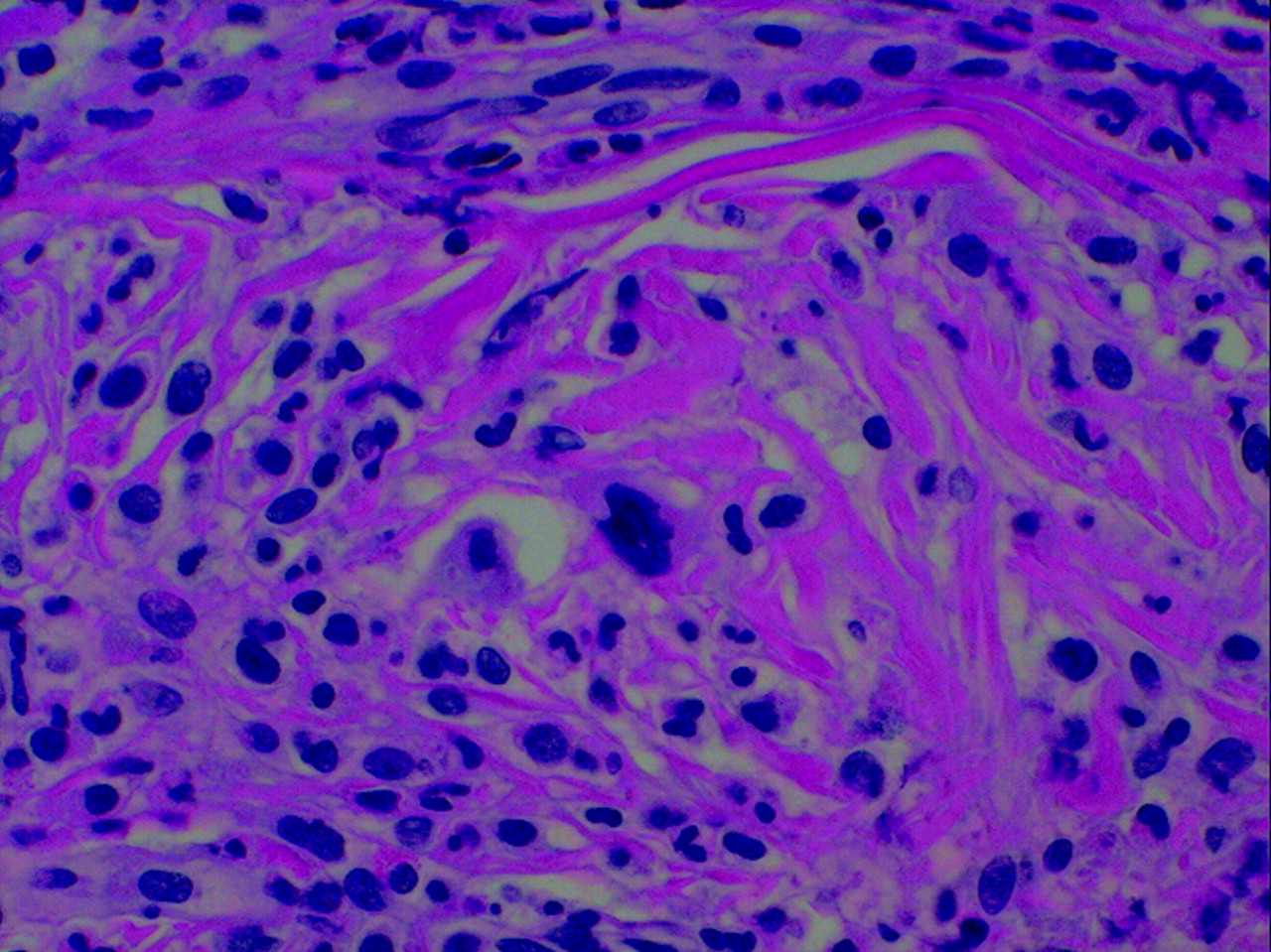
The patient underwent biopsy of both lesions. Histologic examination revealed these masses to be characterized by a proliferation of pleomorphic, large cells and fibrosis that infiltrated, surrounded, and replaced the normal tissue. Every specimen consisted of attenuated, sclerotic connective tissue within which large, atypical cells (megakaryocytic-like) with lobulated nuclei were found as well as scattered lymphocytes and granulocytes (Fig 2).

{kind=link}
{kind=link}
Histologic features. These masses were characterized by a proliferation of pleomorphic, large cells, and fibrosis that infiltrated, surrounded, and replaced the normal tissue. Every specimen consisted of attenuated, sclerotic connective tissue within which large, atypical cells (megakaryocyte-like) with lobulated nuclei were found as well as scattered lymphocytes and granulocytes.
A diagnosis of sclerotic extramedullary hematopoietic tumor was made.
Discussion
Extramedullary hematopoiesis (EMH) is a known complication of myeloproliferative disorders, which include chronic myelogenous leukemia, polycythemia vera, essential thrombocytosis, and myelofibrosis with myeloid metaplasia.1 Among these, it is most commonly associated with myelofibrosis with myeloid metaplasia. EMH is also not uncommonly encountered in chronic anemic states, including sickle cell disease2 and β-thalassemia.3
EMH most commonly involves the reticuloendothelial system (liver and spleen) where it is radiographically manifested as hepatosplenomegaly.1 Nonhepatosplenic EMH is a less common complication of these disease states and has been reported in numerous locations within the body, including lymph nodes, mediastinum, lungs, gastrointestinal and genitourinary systems, and skin.4 Numerous sites of central nervous system (CNS) and head and neck involvement have also been reported, including the middle ear,2 the spine,3, 5 and the suprasellar region.6 It has also been reported in association with an intracranial hemangioblastoma7 and meningioma.8
To the best of our knowledge, this is the first reported case of lacrimal fossa involvement.
In a large series of nonhepatosplenic EMH reviewed by Koch et al,4 paraspinal involvement of the thoracic spine was found to be the most common followed by cervical and para-aortic lymph nodes, the retroperitoneal organs, and the lungs and pleura.
EMH hematopoiesis is usually asymptomatic1 but can present with fatigue or weakness or with symptoms related to its location within the body,4 as it did in this case.
Diagnosis is with cross-sectional imaging with or without biopsy.4 Reticuloendothelial system imaging with technetium Ic99m-sulfur colloid and bone marrow imaging with indium In111-Cl3 have also been used in making this diagnosis.1
MR imaging characteristics of EMH have been described in 2 reports of epidural EMH of the thoracic spine.3, 5 In the former report, T1 isointensity and slight T2 hypointensity compared with bone marrow was demonstrated in a lobulated dorsal epidural mass. No contrast enhancement was reported.3 In the latter report, T1 isointensity to the spinal cord was reported along with marked T2 hypointensity, which was attributed to iron deposition within these lesions. Diffuse contrast enhancement was noted.5
In our case, homogeneous isointensity to slight hyperintensity relative to bone marrow was noted within both lesions. Heterogeneous areas of T2 hypointensity were also noted bilaterally, although this was most likely caused by the presence of densely sclerotic connective tissue noted histologically rather than to iron deposition. These lesions also enhanced.
What is the pathogenesis of these lesions? At least 3 mechanisms have been proposed.3–5 The first is that these masses arise after the deposition of hematopoietic stem cells from the circulation into the involved tissues.4 The second is that these masses arise from fetal rests of hematopoietic stem cells. Finally, direct extension from the adjacent bone marrow is proposed.3, 5 In our case, we feel that the first explanation is possible; in light of the dramatic symmetry of these lesions, however, it is not the most likely. The final explanation is thought unlikely, because there is lack of imaging evidence of direct extension. Consequently, we feel that the second mechanism is most likely.
At the time of interpretation, lymphoma was also a diagnostic consideration; however, prior thoracic and abdominal imaging was available, which showed pleural, mediastinal, and large bilateral perinephric masses with diffuse osseous sclerosis (not shown). Marked hepatosplenomegaly was also noted (not shown). These facts, combined with the history of prior orchiectomy and pathologically confirmed EMH, assured the diagnosis of these lesions even without the more recent biopsy results.
EMH is sensitive to low-dose radiation therapy. Hydroxyurea and thalidomide have also been described in the treatment of EMH.1, 5 Median survival of those with nonhepatosplenic EMH has been reported at 16.5 months.4
References
- Received May 3, 2005.
- Accepted after revision June 10, 2005.
- Copyright © American Society of Neuroradiology