We read with interest the case report by Mathur et al1 in which they have described an acute ischemic event in the posterior part of the intraorbital optic nerve consequent to rhinocerebral mucormycosis and its early detection by diffusion-weighted MR imaging (DW-MR imaging). In this regard, we would like to report another similar case that we came across in our tertiary care institute and benefited from the above report.
In April 2007, a 40-year-old man with diabetes presented to the emergency department with sudden-onset holocranial headache associated with pain in the left eye and diplopia. There was associated proptosis of the left eye. The patient was referred to us for MR imaging of the brain, which showed a normal brain parenchyma and intracranial venous sinuses (as seen on MR venogram). On MR angiogram (Fig 1A) there was nonvisualization of the left internal carotid artery (ICA) with reformation of the left middle and anterior cerebral arteries via the collateral circulation from the right side. Subtle increase in the caliber of the left cavernous sinus compared with the right was noted; no direct or indirect evidence of cavernous sinus thrombosis was noted. Enhancing soft tissue filling the whole of the left sinonasal area was incidentally seen. However, no direct intracranial extension of a sinonasal pathologic process was noted. Edema was seen involving the left lateral rectus muscle (Fig 1B). DW-MR imaging in the axial and sagittal planes with 3-mm sections was done, which showed restriction in the posterior part of the intraorbital segment of the optic nerve on apparent diffusion coefficient (ADC) maps (0.635 × 10−3 mm−2/s). Increased ADC (1.7 × 10−3 mm−2/s) suggesting a vasogenic edema was noted in the anterior part. The posterior part of the nerve did not show alteration in signal intensity on fat-saturated T2-weighted and gadolinium-enhanced, fat-saturated T1-weighted sequences. Fundus examination was normal. This led to a diagnosis of acute posterior ischemic optic neuropathy (PION). The possibility of developing optic atrophy and risks of thromboembolism were explained, and the patient was managed conservatively. Histopathologic specimens from scrapings from the nasal cavity suggested the possibility of Aspergillus infection. The ophthalmic examination showed positive perception of light and projection of rays. However, adequate perimetry was not possible because of poor patient cooperation. Follow-up screening revealed edema in the whole of the intraorbital optic nerve, even in the fat-saturated T2-weighted sequence. The patient sustained multiple territorial infarcts of varying sizes in the subsequent days of his hospital stay, which suggested an embolic phenomenon. He died of a cardiac arrest on day 11.
In most cases of fungal sinusitis, PION is caused by occlusion of the central retinal artery,2 necrosis of the ophthalmic artery,3 infarction and necrosis of the optic nerve,2,3 or direct infection of the optic nerve by mucormycosis.3 In the absence of direct invasion, a sinonasal infection can cause ipsilateral cavernous sinus phlebitis via the pterygoid plexus of the veins, thrombosis of the internal carotid artery being secondary to involvement of the cavernous sinus. Again, isolated ischemia in the posterior part of the intraorbital optic nerve, without direct involvement by a sinus pathologic process, could result from thrombosis of the vessels supplying the perineural pial plexus that is the principal source of blood supply to this segment.4,5 The perineural plexus supplying the posterior part of the optic nerve is formed by a recurrent branch from the anterior superior hypophyseal artery, branches from the ophthalmic artery, and the intraneural recurrent branch from the central artery of the retina, all originating from the segment of the ICA, which was thrombosed in our patient.4 Anastomosis between the orbital branches of the ICA and the facial branches of the external carotid artery may help feed the anterior two thirds of the optic nerve by retrograde flow in the event of occlusion of the ICA, the posterior third remaining deprived.
No treatment of proved value is available for cases having direct extension of infection, yet a trial of systemic corticosteroids can help improve vision in a minority of patients.6 In cases like ours, where arterial thrombosis was the underlying cause, thrombolysis may be helpful. In both situations, DW-MR imaging guides early institution of appropriate therapy and must be considered part of a routine imaging protocol.

{kind=link}
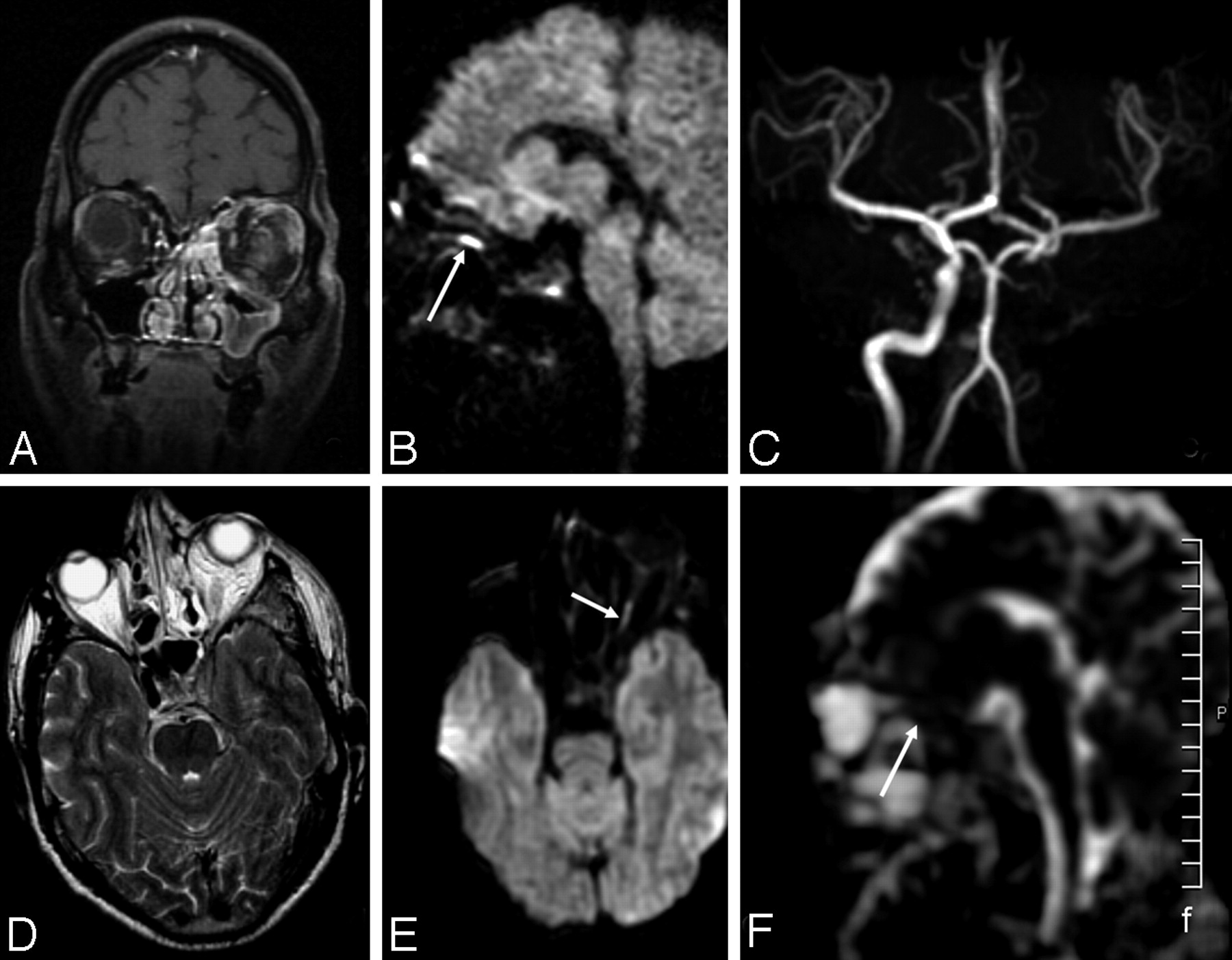
MR imaging shows enhancing mucosal thickening in the left sinonasal complex on coronal postcontrast fat-saturated T1-weighted (A) and axial T2-weighted sequences (B). In addition, the T2-weighted image shows a bulky, enhancing left cavernous sinus with nonvisualization of left ICA flow void (suggesting thrombosis). A 3D time-of-flight MRA (C) shows absence of the left ICA and paucity of the branches of the left distal MCA. Sagittal (D) and axial (E) DW images show restriction in the posterior part of the intraorbital optic nerve (arrow). The ADC map (F) shows reduced ADC in the posterior part (arrow) and increased ADC in the anterior part, respectively.
References
- Copyright © American Society of Neuroradiology