Abstract
SUMMARY: We present a case of carotidynia that was imaged with 3 techniques: sonography, CT angiography, and gadolinium-enhanced MR imaging. We describe a previously unreported finding, the resolution of an intimal plaque noted on imaging at the time of initial presentation, presumably due to changes induced by the healing phase of the carotid inflammatory process.
Carotidynia is an unusual cause of vascular neck pain. Findings on sonography, CT, and MR imaging may support this diagnosis in the appropriate clinical context. We present a unique case of carotidynia with resolution of an existing intimal plaque that was imaged with 3 techniques: sonography, CT angiography (CTA), and gadolinium-enhanced MR imaging.
Case Report
A 46-year-old man presented with a 1-week history of right-neck pain. This was preceded by a flulike illness with low-grade fever, chills, fatigue, and myalgia. The pain was aching in character, 3/10 in severity, and aggravated by movement. He had no headache and his vision was normal. Medical history included gastroesophageal reflux disease and occasional migraines.
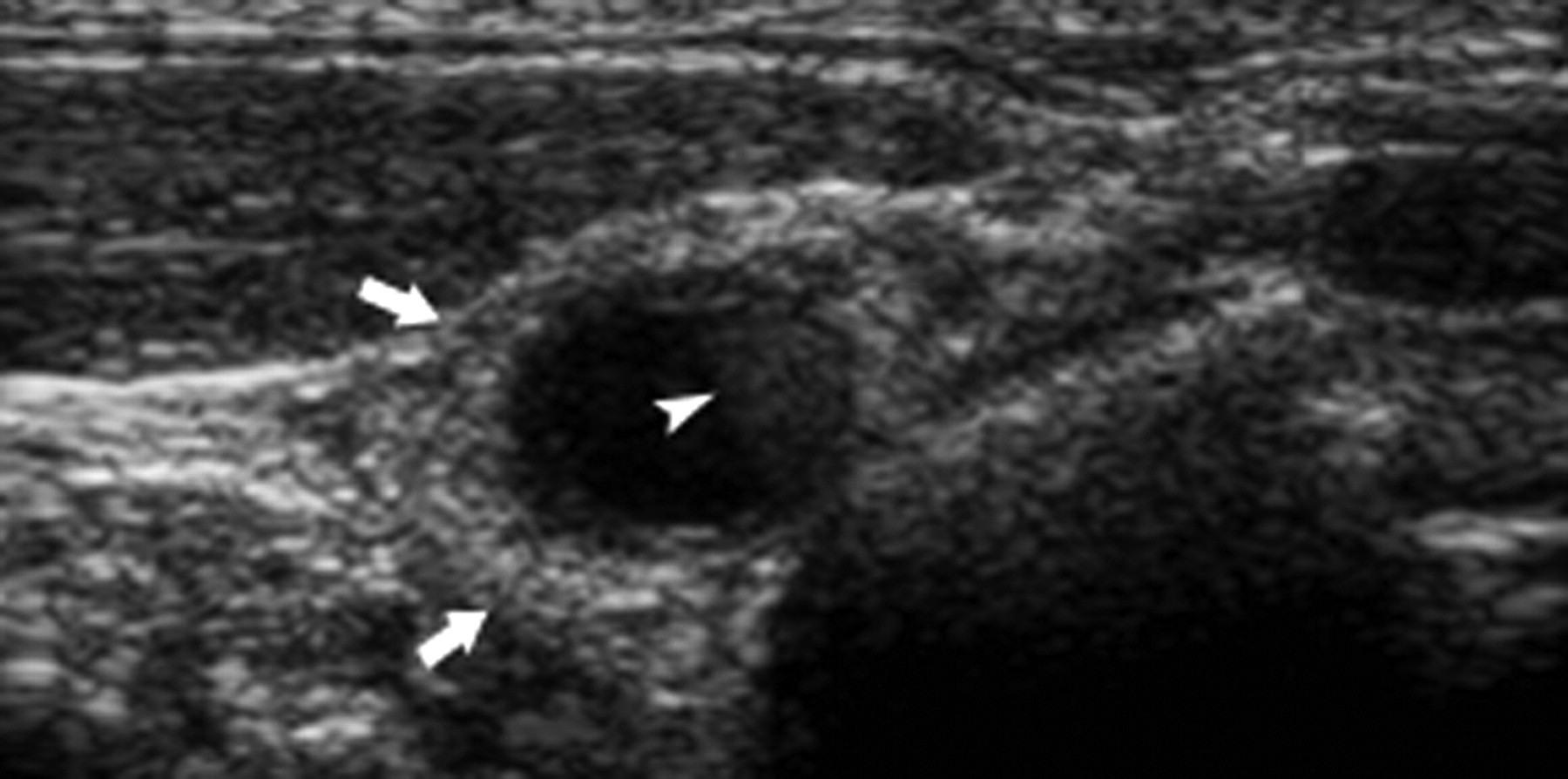
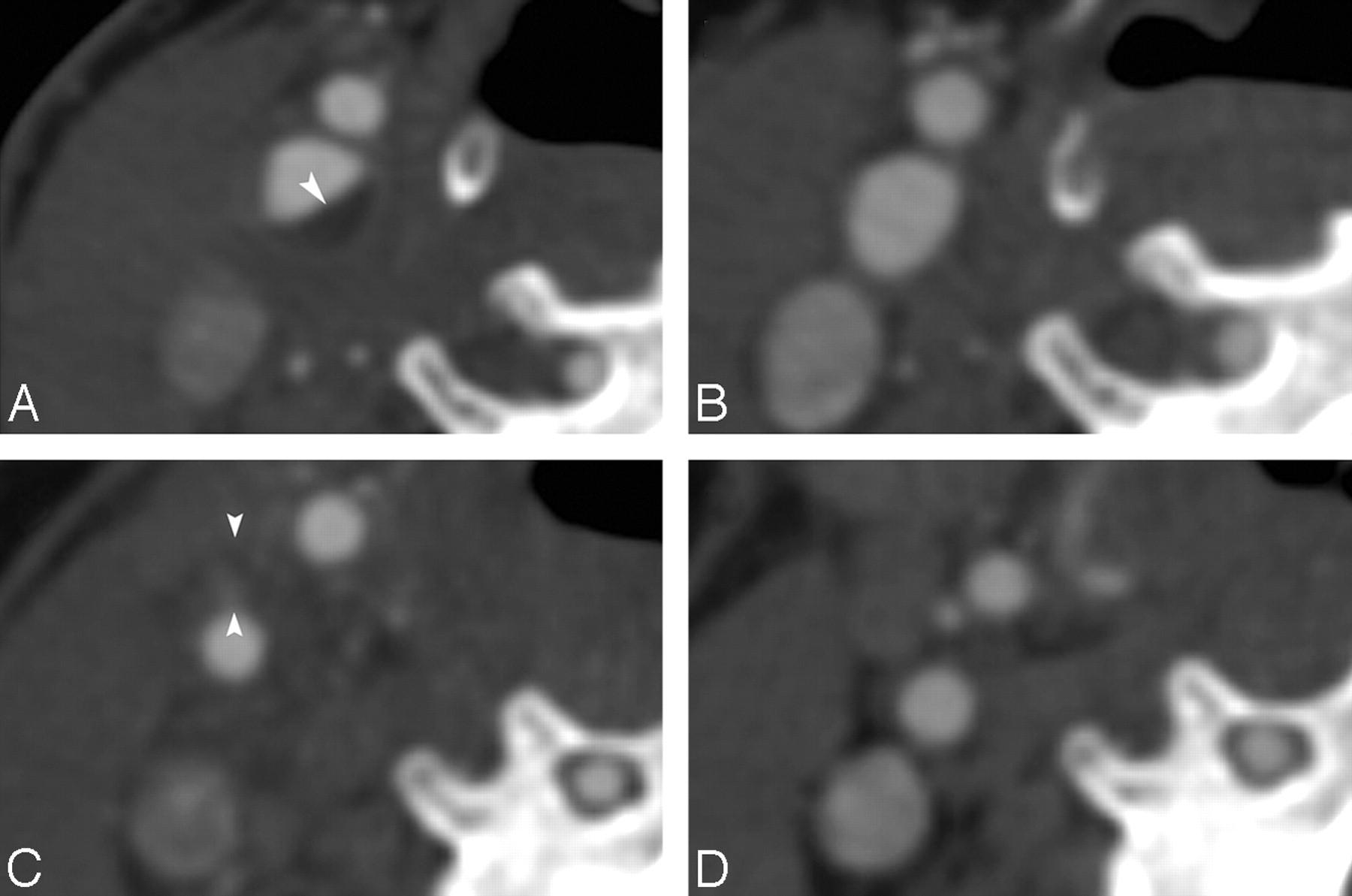
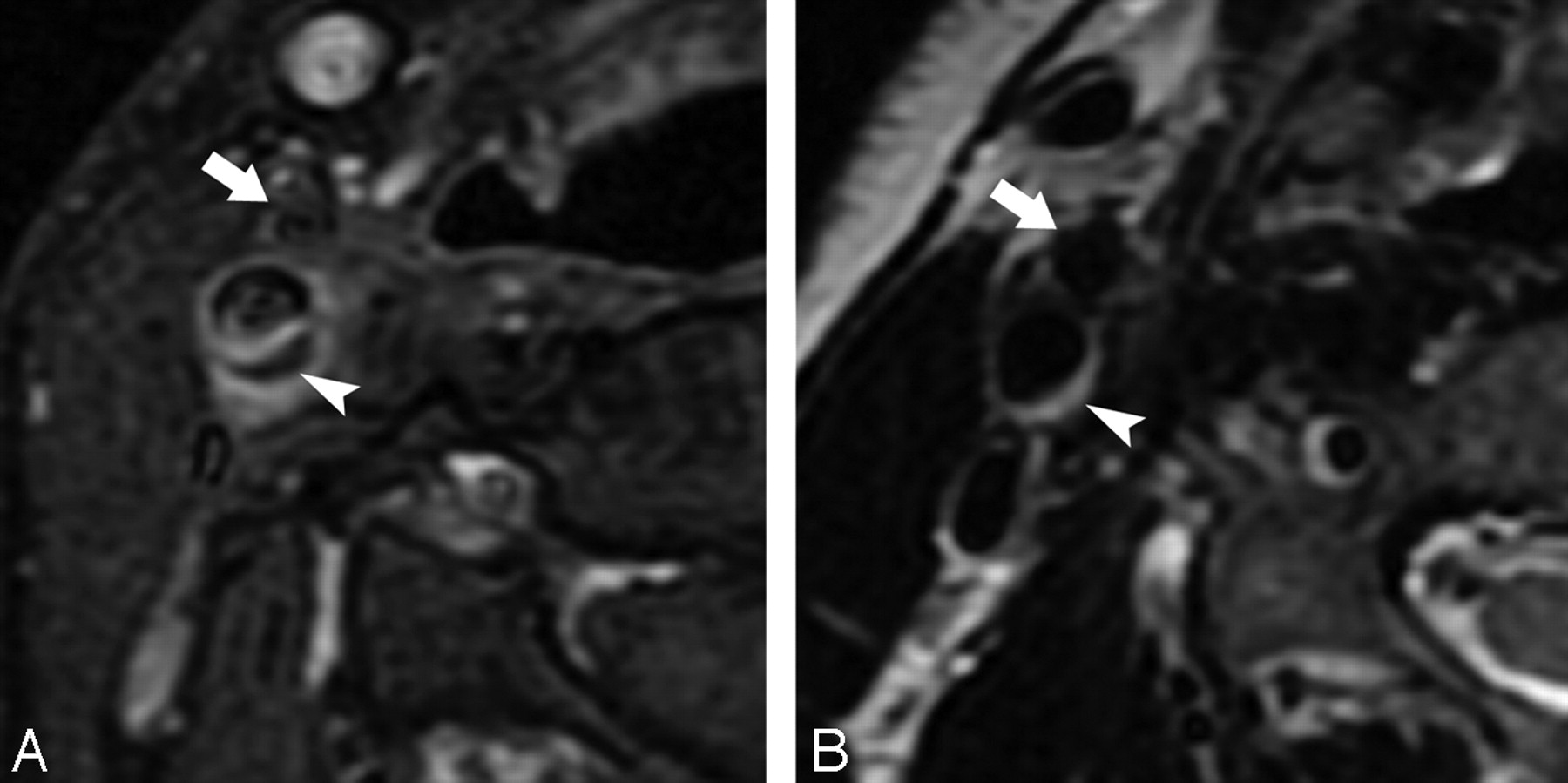
On examination, the patient was afebrile and normotensive. There was localized swelling and tenderness overlying the right carotid bifurcation. There was no associated lymphadenopathy, and no carotid bruits were audible. White blood cell count, erythrocyte sedimentation rate, C-reactive protein, and autoimmune markers (antinuclear antibodies, antineutrophil cytoplasmic antibody, rheumatoid factor) were all normal. Initial imaging was performed approximately 1 week after symptom onset. Sonography demonstrated a thickened vessel wall and an eccentric soft plaque in the distal right common carotid artery (CCA) extending into the proximal internal carotid artery (ICA) (Fig 1). Further evaluation with CTA showed a crescentic fatty plaque, mildly narrowed lumen, concentrically thickened arterial wall, and fat stranding in the carotid space (Fig 2A, -C). Gadolinium-enhanced MR imaging confirmed enhancement of the arterial wall and the presence of a fatty plaque (Fig 3). Sixty milligrams of prednisone per day was initiated and tapered during 8 months to 10 mg per day for ongoing minimal discomfort. All changes resolved at follow-up imaging 5 months after presentation, including the eccentric fatty plaque, which resolved at follow-up with residual irregular inflammatory tissue or scarring (Fig 2B, -D).

Axial gray-scale sonogram of the right CCA demonstrates concentric wall thickening (arrows) and a soft crescentic plaque (arrowhead).

Axial CTA images of the right ICA at presentation (A and C) and at 5 months (B and D). A, An eccentric fatty plaque (arrowhead) is seen in the ICA (−5 HU). B, Resolution of the fatty plaque is noted. C, Concentric wall thickening (arrowheads), narrowing of the lumen, and effacement and stranding of the fat in the carotid space are seen at a level superior to A. D, Resolution of the mural thickening and increased caliber of the ICA, with return of some fatty attenuation in the carotid space, are noted.

{kind=link}
{kind=link}
{kind=link}
Right ICA at presentation (A) and at 5 months (B). A, Axial fat-suppressed postcontrast T1-weighted image demonstrates enhancement of the ICA wall and a fatty plaque (arrowhead) deep to the intima. Arrow indicates right external carotid artery (ECA). B, Axial fat-suppressed T1-weighted image demonstrates resolution of mural thickening and high signal intensity; disappearance of the fatty plaque with irregular mural thickening is now seen (arrowhead), consistent with scarring or residual inflammatory tissue. Arrow indicates right ECA.
Discussion
The causes of vascular neck pain are extensive and include entities such as dissection, giant cell arteritis, thrombosis, fibromuscular dysplasia, aneurysm, Takayasu arteritis, and nonvascular etiologies such as lymphadenitis and submandibular gland disease. After the exclusion of these diseases, carotidynia needs to be considered.
Carotidynia is an idiopathic unilateral neck pain syndrome characterized by tenderness over the carotid bifurcation.1 Neck pain is usually self-limited or resolves with nonsteroidal anti-inflammatory drugs or steroids in <2 weeks. In 2004, the International Headache Society2 published modified criteria for carotidynia, classifying it as a syndrome rather than a distinct pathologic entity (Table). In particular, the criteria specify that patients with carotidynia should not have a structural abnormality of the carotid artery (criterion C).
International Headache Society modified criteria of carotidynia (revised 2004)*
In patients with history, physical, and laboratory results suggestive of carotidynia, imaging with sonography,3 CT,4 and MR5 has revealed fairly consistent findings suggestive of carotid inflammation. Our case and multiple others3–5 have demonstrated 1 or more of the following imaging findings: involvement of a contiguous segment of the distal CCA, bulb, or proximal ICA; mild luminal narrowing; concentric thickening or outward extension of the wall; and enhancing wall and fat stranding in the adjacent carotid space. One report confirmed histologic findings of nonspecific inflammation of the carotid adventitia.6 The etiology of this inflammation is not clear. These imaging findings suggest that a structural abnormality of the carotid artery is present in carotidynia and that criterion C should be revised.
Unique to our case is the appearance of a fatty plaque that resolved at follow-up imaging with minimal residual irregular inflammatory tissue or scarring.
In summary, in the appropriate clinical context, a diagnosis of carotidynia as a cause for vascular neck pain may be supported by characteristic radiologic findings. This case report supports the imaging features of carotidynia previously described in the literature. In addition, our case had a finding not previously described, the resolution of a fatty plaque noted on imaging at the time of initial presentation, presumably due to changes induced by the healing phase of the carotid inflammatory process.
References
- Received September 6, 2007.
- Accepted after revision November 12, 2007.
- Copyright © American Society of Neuroradiology