Abstract
BACKGROUND AND PURPOSE: Air cells are often seen within the frontal intersinus septum. These cells have traditionally been thought to arise from displaced ethmoid cells from the frontal recess. This study explores the possibility that such cells may actually be diverticula from the frontal sinuses themselves and not of a direct ethmoid origin.
MATERIALS AND METHODS: A prospective study of 200 consecutive CT scans in the coronal and axial planes was performed on patients without a history of recent trauma. The images were interpreted independently by a radiologist and an otolaryngologist. The CT studies were evaluated for the presence of a central intersinus septal air cell. If such a cell was identified, it was further classified as either being completely isolated from both frontal sinuses by a bony rim or as a communicating diverticulum from one of the frontal sinuses. If a central cell was present, it was also assessed for how much of the height of the intersinus septum it involved (lower one-half or full height).
RESULTS: There was a complete concordance of the results between the 2 observers. An intersinus septal air cell was seen in 61 (30.5%) of the 200 cases, and 85.3% of these cells were clearly seen to communicate anteromedially with either one of the frontal sinuses or both frontal sinuses (3 cases). In 9 (4.5%) of the 200 cases, the central cell had no demonstrable connection to either frontal sinus. Of the 61 cases with a central cell, 55 (90.16%) of the cells occupied the full height of the septum, and 6 (9.84%) only involved the lower half of the septum.
CONCLUSION: Contrary to the present convention that frontal intersinus septal cells originate as displaced ethmoid cells from the frontal recess, we found that most such cells are actually diverticula from the frontal sinuses themselves.
The development of the frontal sinus from the anterior ethmoid labyrinth allows for the presence of extramural ethmoid cells both around and within the frontal sinus proper. These cells, which communicate with the frontal recess, include supraorbital, infrafrontal, and intersinus septal cells. Such cells were identified by anatomic dissection studies in the first part of the 20th century and were subsequently detailed by radiographic imaging in living patients.1–3
The belief that there was a common embryogenesis of the frontal sinus and associated cells by evagination and pneumatization from the frontal recess have resulted in a generally accepted unifying hypothesis of their formation. However, our study challenges the concept that the intersinus septal cell is uniformly of an ethmoid derivation. Rather, we suggest that such a cell may most often represent a diverticulum from the frontal sinus itself.
Materials and Methods
From our outpatient population, we prospectively performed 200 consecutive CT studies of the paranasal sinus in both the axial and coronal planes on patients without a history of recent trauma (Figs 1–⇓⇓4). We performed the study with approval of the internal review board (#06-0254). The images were reviewed by a dedicated head and neck radiologist and an otolaryngologist. The images were specifically analyzed for the presence of intersinus septal cells and the location of the cell within the septum (lower half or the entire septum). If an intersinus cell was identified, it was further assessed as either being completely isolated from the frontal sinuses by a bony wall or as being a diverticulum from a frontal sinus.

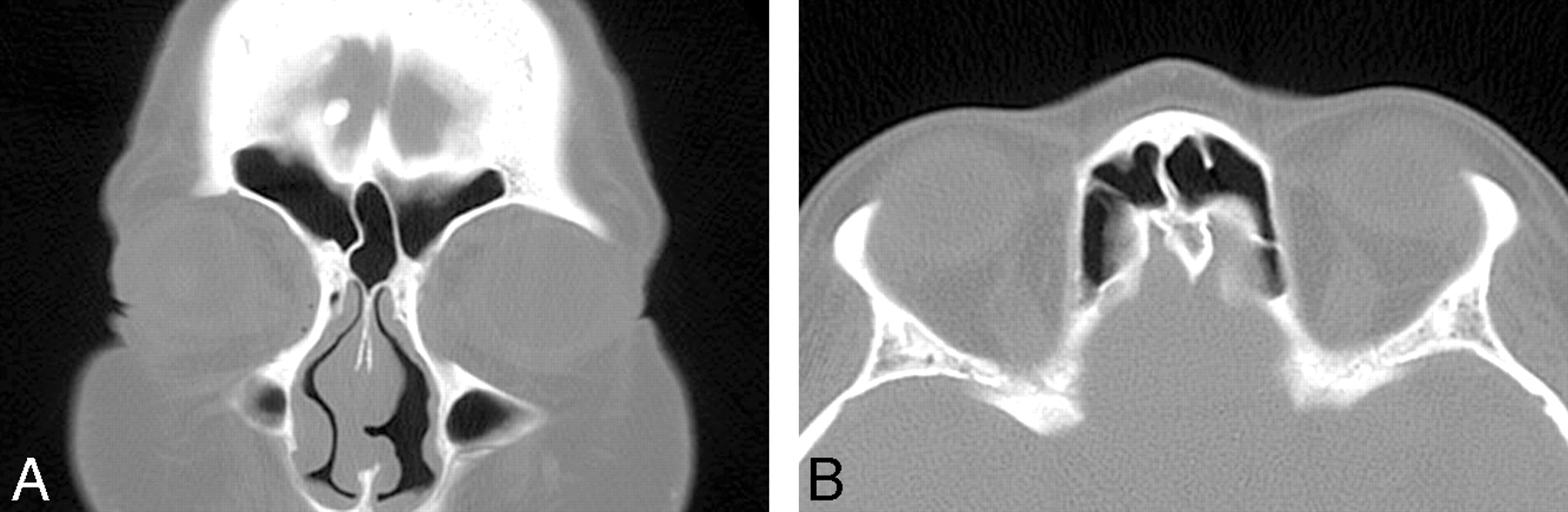
Coronal (A) and axial (B) noncontrast CT scans of the paranasal sinuses show an air cell within the intersinus septum. On the coronal image, the cell seems to arise within the septum. However, on the axial image the cell is seen to be a diverticulum from the left frontal sinus.

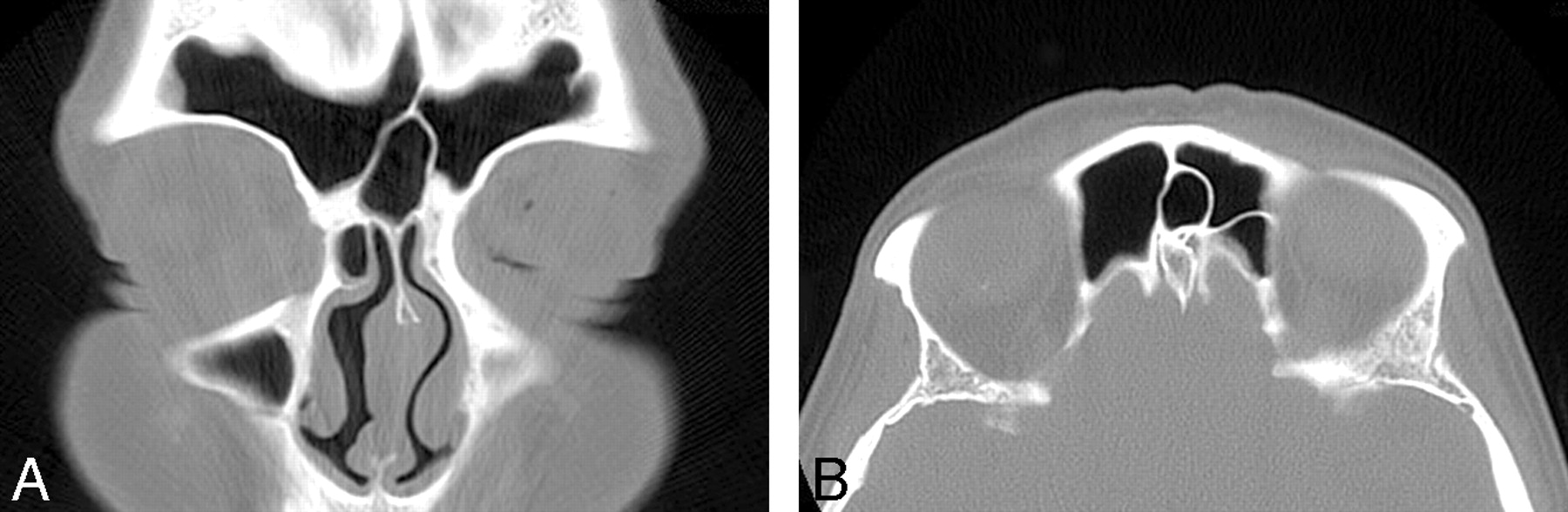
Coronal (A) and axial (B) noncontrast CT scans of the paranasal sinuses show an air cell within the intersinus septum. On the coronal image, the cell seems to arise within the septum. However, on the axial image the cell is seen to be a diverticulum from the right frontal sinus.

Coronal (A) and serial axial (B,C) noncontrast CT scans of the paranasal sinuses show 2 air cells within the intersinus septum. On the coronal image, the cells seem to arise within the septum. However, on the axial images, 1 cell is a diverticulum from the left frontal sinus (B), and the other cell is a diverticulum from the right frontal sinus (C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coronal (A) and axial (B) noncontrast CT scans of the paranasal sinuses show an air cell within the intersinus septum. On both the coronal and axial images, no communication with either frontal sinus was seen. This is a true septal cell.
Results
There was a complete concordance of the results between the 2 observers. An intersinus septal air cell was seen in 61 (30.5%) of the 200 cases, and 85.3% of these cells were clearly seen to communicate anteromedially with either of the frontal sinuses or both frontal sinuses (3 cases). In 9 (4.5%) of the 200 cases, the central cell had no demonstrable connection to either frontal sinus. Of the 61 cases with a central cell, 55 (90.16%) of the cells occupied the full height of the septum, and 6 (9.84%) only involved the lower half of the septum.
With respect to all of the 200 patients, 31 (15.5%) had right-sided diverticula, 18 (9%) had left-sided diverticula, 2 (1%) had bilateral diverticula, 1 (0.5%) had a central cell and a diverticulum from the fright frontal sinus, and 9 (4.5%) had central cells without demonstrable connection to either frontal sinus. In 6 (3.0%) cases, the central cell was in the lower third of the septum, and the central cell occupied the entire septum in 55 (27.5%) cases.
Discussion
The presence of extramural frontal sinus cells, initially interpreted as duplications of the frontal sinus, has been known since the early 1900s when anatomic studies of the frontal sinus described the presence of multiple air cells within the frontal bone.4,5 However, to understand the true derivation of these frontal sinus cells, it is necessary to review the present knowledge of how the frontal sinuses develop. The frontal sinus first begins in the third to fourth fetal month with the appearance of the frontal recess in the lateral nasal cavity wall.1,6 A series of pits1–4 or furrows develop in the frontal recess, which represent rudimentary anterior ethmoid cells. Each pit has the potential to form the frontal sinus; hence the variability in the outflow tract of the frontal sinus. Occasionally, the frontal sinus may develop from an ethmoid cell migrating from the ethmoid infundibulum rather than from the frontal recess, and combined patterns of development may result in multiple sinuses on each side.7,8
In addition to establishing the origin of the frontal sinus from the frontal recess, Schaeffer1 also attributed the derivation of what he termed frontal cells to be from the anterior ethmoid labyrinth. These findings were further quantified by Van Alyea,2 who found 100 specimens containing ethmoid cells extending into the frontal sinus on dissection of 242 skulls. He grouped these broadly into frontal recess cells and invading cells. The invading cells consisted of supraorbital ethmoid, intersinus septum, and infrafrontal air cells. In 28 specimens, an intersinus cell was detected, of which 14 drained into the frontal recess, 11 drained above the infundibulum, and 3 drained into the infundibular groove.
The major development of the frontal sinus occurs in the postnatal period, where the sinus slowly enlarges until completion of growth at approximately the end of the second decade of life.2 In a study of 160 skulls, ranging in age from birth to 16 years, Davis5 detected the earliest presence of a cell in the frontal bone at 2 years of age. The frontal bone cell extended to 3.8 mm above the nasion at 3 years of age and increased at a rate of 1.5 mm/year until 15 years of age. Each frontal sinus develops by pneumatizing the medullary cavity of the frontal bone. The remaining medullary bone between the 2 frontal sinuses is the intersinus septum. Because the initial frontal sinus growth is fairly symmetric, the intersinus septum is almost always in the midline at its most caudal extent. However, as there is usually differential growth of the 2 frontal sinuses, the intersinus septum usually then deviates away from the side of the larger frontal sinus, often terminating far off of the midline.
In a study by Merrit et al,3 on the basis of coronal CT scans of 100 cadavers and 200 patients with chronic sinusitis, an intersinus septal cell was identified in 34% of the studies. These cells were subdivided into cells limited to the nasofrontal region at the base of the septum, those cells extending the entire length of the septum, and those cells that were intermediate in their septal pneumatization. These authors suggested that these cells originated from ethmoid extensions.
Our study used CT scans on 200 patients studied in both the axial and coronal planes. We found a septal cell in 30.5% of the cases. Of these cases, 85.3% were seen to communicate anteromedially with either one of the frontal sinuses or both frontal sinuses (3 cases). In these cases, the interseptal cells were considered to arise from a frontal sinus and not directly as a result of migration from the frontal recess. In 9 (4.5%) of the 200 patients, the central cell had no demonstrable connection to either frontal sinus, and these cells were considered to be displaced cells of ethmoid origin. Of the 61 cases with a central cell, 55 (90.16%) of the cells occupied the full height of the septum, and 6 (9.84%) only involved the lower half of the septum. These findings suggest that the genesis of intersinus septal air cells may primarily be from the frontal sinuses themselves rather than from migration of an anterior ethmoid cell into the intersinus septum.
Conclusion
There is a widely held concept that, in a similar manner to the development of supraorbital and intrafrontal sinus cells, intersinus septal cells originate from the frontal recess. However, our study, based on axial and coronal CT studies of 200 patients, suggests that most intersinus septal cells are diverticula from the frontal sinuses and not ectopic frontal recess cells.
References
- Received June 14, 2007.
- Accepted after revision January 27, 2008.
- Copyright © American Society of Neuroradiology