Time is on my side, yes it is…
Norman Meade and The Rolling Stones
Recent studies have attempted to capture the frequency and clinical significance of recurrences after endovascular treatment of aneurysms. For the group of patients with satisfactory occlusions at 6 months, the rate of recurrent subarachnoid hemorrhage (SAH) is very low and the yield of further imaging has been shown to be minimal. Study methodology remains weak, but the burden of the proof has shifted to those who propose new devices or more follow-ups (and presumably more retreatments).1
Long before the introduction of controllable coils, angiographic recurrences were the Achilles' heel of selective endovascular treatments of aneurysms. I became obsessed with the problem in 1992 when, happy to abandon the dreaded detachable balloons, I used coils for the first time. To my dismay, my patient came running back with a major recurrence a few months later. Despite this drawback, detachable coils were a breakthrough in providing a safer treatment of aneurysms, and engrossed by its new success, the neurointerventional community took time to acknowledge that there was a problem. Still, every single article reporting promising results ended with the conclusion that a longer follow-up would be necessary. The technique had to elbow its place into the market, and competition with surgical clipping played no small role in the debate regarding the magnitude and significance of recurrences. The coil industry, initially appalled by the alleged incidence of recurrences, came to appreciate a new friend. There is no crisis; only new opportunities. An ever larger number of initial-experience publications with second-generation coils and stents were destined to awkwardly conclude that a longer follow-up would be necessary.
How to deal with the issue of time in clinical research is a difficult matter. I remember my first written argument with an unhappy reviewer of a neurosurgical journal. He replied that time will tell. Today, I know that if our bones claim that we are getting old, time is quite mute on any particular subject. Good methodology and hard work may provide some answers to our questions, but contrary to what the Rolling Stones' song says, time is a false friend in most research enterprises, particularly if it is retrospective (often badly planned and conducted in our young field) or when expediency is favored over accuracy, as exemplified by an expanding literature on computer simulations projecting speculations over the lifetime of individuals, to the detriment of prudent assembling of clinical evidence.
Almost 20 years after the invention of detachable coils,2 we are still debating over the “real” magnitude of the problem: Whether late rebleeding risks from recurrences could eventually overcome the superiority of coiling over clipping in young patients3,4 and the efficacy of coiling in the prevention of hemorrhage in patients with unruptured aneurysms remain a mystery.5 Nonetheless, coiling has grown in popularity in all but the most conservative centers. In the absence of reliable evidence, we were inclined to lean on a priori prudential maxims to decide what a responsible physician should do, and a common answer to the problem was to follow individual patients closely for potential recurrences. The trouble is that by doing so we may be causing more harm than good. At least this is the message I understand from van Rooij and Sluzewski,1 who question, in this issue of the American Journal of Neuroradiology, the common advice to follow patients closely for years after coiling. They suggest that imaging follow-up is necessary in only in a special group of patients, because in most patients (80%) with adequately occluded aneurysms at 6 months, the risk of SAH from recurrences and de novo or additional aneurysms is extremely low. We will examine here whether the argument is compelling and if the claim is supported by evidence.
When Do Coiled Aneurysms Recur?
van Rooij and Sluzewski,1 first distinguish between imaging performed to verify that coiled aneurysms remain occluded and imaging to detect the growth of additional or de novo aneurysms. Let us examine the first question they raise regarding the fate of coiled aneurysms: “Can an aneurysm that is adequately occluded at 6 months still reopen at a later point in time and, if yes, at what point in time?” The authors rightly point out that in most studies, the time interval between coiling and the first follow-up study is variable and not predetermined. They suppose that recurrences beyond 6 months could have been detected earlier had an angiogram been obtained. In support of their claim is a series of 126 patients with ruptured aneurysms, 90 with a fixed follow-up at 6 and 18 months, in which none had shown a significant change between the 2 angiograms.6
I for one was not convinced by that series for 3 main reasons: The first one is methodologic. This was a small retrospective study; only 90 patients of the initial 160 had a second follow-up angiogram and it was impossible to be sure that knowledge of the subsequent evolution of the patient had not modified the initial or follow-up angiographic verdict. It is one thing to detect retrospectively that this recurrence was actually heralded by a small but perceptible change at 6 months, compared with the near-occlusion obtained at the time of treatment; it is quite another to make the same claim prospectively. The second reason has to do with time. How can we be reassured that the absence of a perceptible change between the 2 angiograms is a signature of stability? Simply by showing that none of the 90 stable patients had a recurrence after 18 months. However, only 13 and 4 patients had a third and fourth angiogram at 3 and 4 years, respectively. Hence, the claim of stability beyond 18 months is based on 17 patients only. It is, of course, impossible to diagnose late recurrences if we do not look for them.
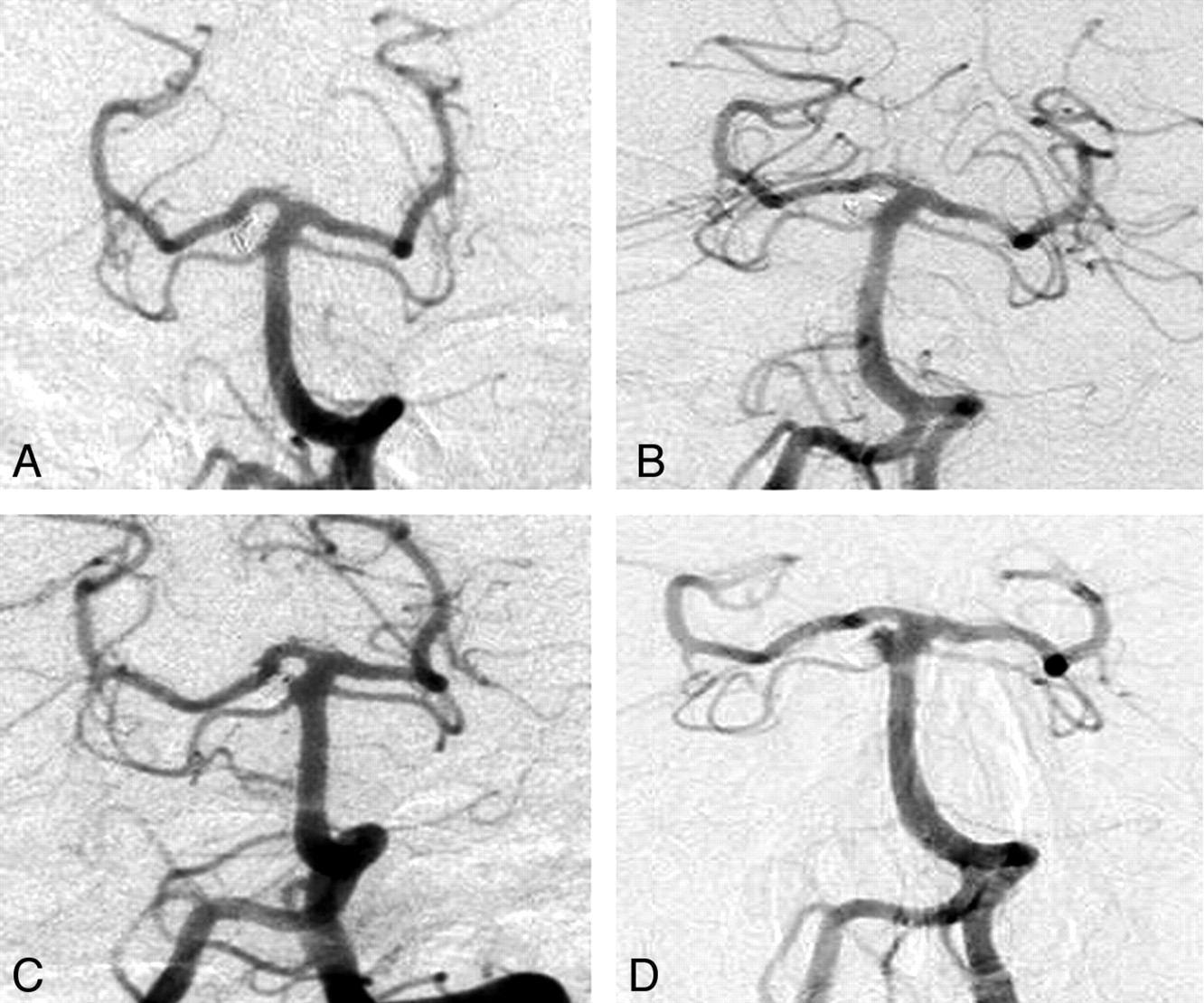
The last reason is factual: I have repeatedly witnessed patients with “stable” complete or near-complete occlusions for many follow-up examinations, only to have them show up years later with recurrences (Fig 1).7 It is true that, grosso modo, 2 types of recurrences can perhaps be distinguished: 1) a more problematic, more frequent, premature type, detectable at 6 months; and 2) a delayed type became more than anecdotal only when follow-up studies were performed 3 years or more after satisfactory occlusions.7 I am aware that some teams, evoking a different mechanism, prefer to call these late recurrences “new aneurysms at the same site,” but surely the problem cannot be evaded by giving it a different name.

{kind=link}
Angiograms show satisfactory occlusion postcoiling (A) and stability at 2 years (B), only to have the aneurysms recur (minimally) 4 (C) and (significantly) 6 years later (D).
Even if occluded aneurysms (at 6 months) could recur on longer follow-up examinations, the question van Rooij and Sluzewski1 ask remains pertinent: Are these recurrences sufficiently frequent to justify follow-up studies? Now to capture this frequency accurately, we need large numbers, long-term prospective follow-up studies, a strong methodology to provide power, and decreased bias and sampling error.
What Is the Evidence?
Unfortunately, the 2 studies van Rooij and Sluzewski1 used to support their claim are quite weak: Both are retrospective and observational. We review here the most pertinent weaknesses. One study retrospectively recalled 104 (17%) surviving patients with satisfactory occlusion at 6 months from a cohort of 612 patients with ruptured and unruptured aneurysms, to perform 3T MR imaging 6 years after coiling: 181 patients were excluded for recurrent or incompletely occluded aneurysms (was this determined prospectively, before 6 months?), 73 were untraceable (did they bleed?), 84 were excluded for various reasons, and 36 declined.8 MR angiography (MRA) findings were “if necessary, compared with results of angiographic follow-up at 6 months,” raising the concern of post hoc selection. Recurrences were found in 4 of 104 patients (95% confidence interval, 1%–9%), necessitating retreatment in 1 (0%–5%).8 To show that retrospectively recalling selected patients for follow-up studies has a low yield is not showing that the careful prospective follow-up of patients is useless. Moreover, how can we project with confidence the results obtained in 17% of patients onto 80% of patients (the claimed proportion of patients with satisfactory occlusions at 6 months)?
The other study is an invalid comparison between 2 divergent series of post hoc selected coiled-but-not-clipped patients with satisfactory occlusions at 6 months (60% of the entire cohort of 476 patients with coiled ruptured aneurysms) and less selected clipped-but-not-coiled patients (96% of 776 clipped patients with SAH), showing that at most 0.2%–3.1% of coiled patients and 1.3%–3.6% of clipped patients had another SAH in the first 10 years after the initial SAH.9 van Rooij and Sluzewski1 have now changed subject, from recurrences seen on imaging to recurrent SAH. The problem here is that most SAHs observed in the clipping cohort were related to additional or de novo aneurysms (only 4/18 were related to the treated aneurysm), suggesting that some form of bias must be involved (why should coiled aneurysms have a lesser incidence of multiple aneurysms?). Hence, the observation that the risk of recurrent SAH after coiling is 5 times lower than that after clipping is invalid.10,11
In the only randomized trial available (International Subarachnoid Aneurysm Trial [ISAT]), late rebleeds were more frequent (though not significantly so) after coiling (7 versus 3) but late retreatments (9% versus 0.85%) were clearly more frequent.12 ISAT can be criticized, if only because patients with clipped aneurysms were not followed by imaging the way patients with coiled aneurysms were. It may be interesting to note further that in this randomized series of small ruptured aneurysms, complete occlusions were less frequently associated with retreatments, except after 3 years, probably because some recurrences take a long time to be manifest.12 Yet again, this is no strong objection. Is the frequency of recurrent SAHs sufficient to justify follow-up imaging in all these patients? The answer seems to be no. If SAH can be considered a life-long disorder because patients remain at a much higher risk of recurrent SAH than the general population, screening of clipped patients (and by extrapolation of coiled patients) is not cost-effective.9,13–15 It is true that long-term rebleeds in ISAT (and in the Cerebral Aneurysm Rerupture After Treatment trial) were reassuringly uncommon; however, would this still be true had follow-up imaging and retreatments not been performed?12,16
Imaging for Additional and De Novo Aneurysms
The case for follow-up imaging for growth of additional or de novo aneurysms is even weaker. The yield of follow-up MR imaging in a small series of coiled patients was shown to be minimal.17 Follow-up CT angiography in clipped patients was not cost-effective and of questionable merit.15,18 Although SAH may be seen in aneurysms shown to have grown in retrospect,19 no one has proved that aneurysms that have increased in size must be treated. If we still lack proof that treating unruptured aneurysms is beneficial, it is no wonder that follow-up imaging of untreated aneurysms, watching for growth, and detecting new aneurysms can only lead to more treatments that are still unjustified by evidence, even though the follow-up imaging program accompanying therapeutic abstention was designed to replace unjustified interventions in the first place.20
Care of Patients
van Rooij and Sluzewski1 have succeeded in undermining the role of imaging in the detection of the growth of additional or de novo aneurysms, and they have shown, by using imperfect but fair methods, that if we focus on coiled aneurysms that remain occluded or near-occluded at 6 months, recurrences are so infrequent that their clinical relevance must be small. The implications of this conclusion may be far-reaching. Perhaps new devices designed to improve the efficacy of endovascular treatment should be sparingly and selectively used because they may benefit only a small proportion of patients. The methods that the authors have used are prone to error, and I am still worried that their proposition, too eagerly applied, may do some harm. We know how complacent self-evaluation of angiographic results can be.21 This complacency, combined with pressure to use the less invasive MRA for follow-ups, with the attending difficulty in reliably comparing 2 different modalities at 2 different dates (digital subtraction angiography at the end of treatment and MRA at 6 months), could yield a spuriously high proportion of stable near-occlusions that could never be shown to be erroneous if longer follow-ups are not performed.
There is here a tension between individual care and a more global assessment of our performance, as well as between 2 prudent attitudes that may not be equally appropriate, depending on context: 1) more care (read “more follow-ups”) means better care, and 2) do not impose on patients tests (that can lead to treatments) that have not yet been proved beneficial. The latter principle is 1 version of the primo non nocere clause that may now be more appropriate to a more mature field. When endovascular treatment was progressively replacing clipping, it may have been prudent to ensure that the treatment “holds.” Still, in Raymond et al,7 our recommending close and long follow-ups simply because more recurrences could be found that way was fallacious reasoning: The mere presence of an imaging finding is not a mandatory indication for doing something about it.
In general, we must first prove that our actions lead to better outcomes. This proof is currently not available for any type of patient, not even those with troublesome aneurysms that recur within 6 months. We know that the reliable way of showing a clinical benefit from follow-up imaging or from new devices designed to improve efficacy is to resort to the difficult but rigorous methodology of a trial. However, the numbers shown by van Rooij and Sluzewski1 may simply be too small to justify such an effort, at least for patients with satisfactory occlusions at 6 months.
I doubt that the last word has been said on this subject, but we must thank these authors for stimulating a deeper reflection on this matter. By looking for data rather than sticking to a priori opinions, they have opened the way to a more rigorous assessment of the problem. Their work is an important contribution to a field aiming for maturity.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- Copyright © American Society of Neuroradiology