Abstract
BACKGROUND AND PURPOSE: The outcome of treatment for unruptured intracranial aneurysm by surgery or endovascular therapy appeared to be related to the volume of patients treated by the hospital. We performed an analysis in the ATENA series to determine whether the outcome of endovascular treatment was different in hospitals with low and high volumes of cases.
MATERIALS AND METHODS: The ATENA series included 649 patients with 739 unruptured intracranial aneurysms. Patients were classified into 2 groups. Group A had 171 patients with 197 aneurysms in 13 centers that treated ≤20 patients; group B, 478 patients with 542 aneurysms in 14 centers that treated ≥21 patients.
RESULTS: Groups A and B had similar patient populations and aneurysm characteristics. Stent placement was used in group B more frequently than in group A (9.6% versus 2.5%, P = .0016). The global rate of adverse events was not significantly different in groups A and B (16.0% and 14.4%, respectively). Thromboemobolic events and intraoperative rupture were not significantly more frequent in group A than in group B. One-month mortality and morbidity rates were not significantly different in groups A (2.3% and 1.8%, respectively) and B (1.0% and 1.7%, respectively). Anatomic outcomes for groups A and B were not significantly different.
CONCLUSIONS: Clinical and anatomic outcomes of endovascular treatments for unruptured intracranial aneurysms were similar in hospitals with low and high volumes of cases.
Abbreviations
- ACA
- anterior cerebral artery
- AcomA
- anterior communicating artery
- ATENA
- Analysis of Treatment by Endovascular Approach of Nonruptured Aneurysms
- CH
- centre hospitalier
- CHU
- Centre Hospitalier Universitaire
- CI
- confidence interval
- GP
- group
- HTA
- hypertension artérielle
- ICA
- internal carotid artery
- MCA
- middle cerebral artery
- mRS
- modified Rankin Scale
- NA
- not applicable
- TE
- thromboembolic complications
- UIA
- unruptured intracranial aneurysm
- VB
- vertebrobasilar system
The prospective multicenter ATENA series was conducted in France to evaluate the outcome of endovascular treatment for UIAs.1 That analysis showed that endovascular treatment of unruptured intracranial aneurysms was feasible in a high percentage of cases (95.7%), with low morbidity and mortality rates (1.7% and 1.4%, respectively).
However, some controversy arose regarding the relationship between clinical outcome and the volume of specific surgical procedures or medical conditions treated in a given hospital (cases/hospital volume).2 Few investigations have addressed this point for the treatment of intracranial aneurysms.3–9 To clarify the relationship between outcome and cases/hospital volume for endovascular treatment of unruptured intracranial aneurysms, we conducted a subgroup analysis on the ATENA population. The subgroups were formed on the basis of the number of patients treated in a single center.
Materials and Methods
Protocol
The ATENA protocol has been previously presented.1 Briefly, ATENA was conducted by the French Society of Neuroradiology to evaluate the results of endovascular treatment for patients with UIAs. From June 2005 to October 2006, 649 patients were prospectively and consecutively enrolled from 27 Canadian and French neurointerventional centers to be treated with an endovascular approach. The inclusion criteria were the presence of ≥1 unruptured previously untreated intracranial aneurysm of <15 mm. Patients with fusiform and dissecting aneurysms and aneurysms associated with brain arteriovenous malformations were excluded.
The protocol was approved by the Ethics Committee of Reims, and informed consent was obtained from all patients.
Clinical status was defined with the mRS. Clinical and procedural data were collected, encoded for anonymity, and entered via an electronic Web site; the blinded data were subsequently reviewed by the principal investigators (L.P. and L.S.). All adverse events that occurred in patients with or without clinical modifications were reported.
Permanent morbidity and mortality rates of treated patients were evaluated at 1 month. Morbidity was defined as an mRS score from 2 to 5. When a preoperative mRS was >1, morbidity was defined as any increase in the mRS score.
The neuroradiologist who performed the treatment evaluated the degree of aneurysmal occlusion on the basis of the modified 3-point classification scale of Raymond et al10: complete occlusion, neck remnant, and aneurysm remnant.
Group Definitions
The ATENA study centers were classified according to the number of patients treated during the study period. To divide the centers into approximately equal groups, we used an arbitrary limit of 20 patients treated during the period of inclusion.
Group A included 13 centers that treated ≤20 patients: In 1 center, <5 patients were treated; in 2 centers, 6–10 patients were treated; in 5 centers, 11–15 patients were treated; and in 5 centers, 16–20 patients were treated.
Group B included 14 centers that treated >20 patients: In 8 centers, 21–30 patients were treated; in 4 centers, 31–40 patients were treated; and in 2 centers, >40 patients were treated.
Separate analyses were also conducted by using different cut-points, including 1 patient treated per month (≤17 patients or >17 patients during the study period) and 20 patients treated per year (≤28 patients or >28 patients during the study period).
Statistical Analysis
Data management and statistical analyses were independently conducted by the Clinical Research Unit of Reims University Hospital (F.V.) to calculate patient demographics, aneurysm characteristics, treatment, adverse events, and outcome. Mean and frequency comparisons were performed with the Student t test and χ2 test or the Fisher exact test, respectively. Differences were considered significant at P = .05. Statistical analysis was performed with SAS Version 8.0 software (SAS Institute, Cary, North Carolina).
Results
Analysis was performed by using different cut-points: 17, 20, and 28 patients during the study period (see “Materials and Methods”). Results were similar regardless of the cut-point used, and only results obtained with the cut-point of 20 patients are presented in this section.
Patient Population
The distributions of sex, age, and risk factors (smoking and hypertension) of groups A and B were not significantly different (Table 1).
Patient characteristics in centers with low (group A) and high (group B) numbers of cases/hospital
Aneurysm Characteristics
The aneurysm characteristics (location, aneurysm size, dome-to-neck ratio) of the groups were not significantly different (Table 2).
Aneurysm characteristics in centers with low (group A) and high (group B) numbers of cases/hospital
Modalities of Endovascular Treatment of UIAs
The numbers of nonselective and selective treatments were not significantly different between groups A and B (Table 3). However, the selective treatments were performed significantly differently in group A compared with group B: The standard coiling technique was more frequently used in group A versus group B (62.4% and 50.4%, respectively; P = .001). Conversely, stent placement was more frequently used in group B versus group A (9.6% and 2.5%, respectively; P = .0016). The remodeling technique was used with a higher frequency in group B (38.6% compared with 31.5% in group A), but it was not significant (P = 0.07).
Modalities of treatment in centers with low (group A) and high (group B) numbers of cases/hospital
Adverse Events Related to Endovascular Treatment of UIAs
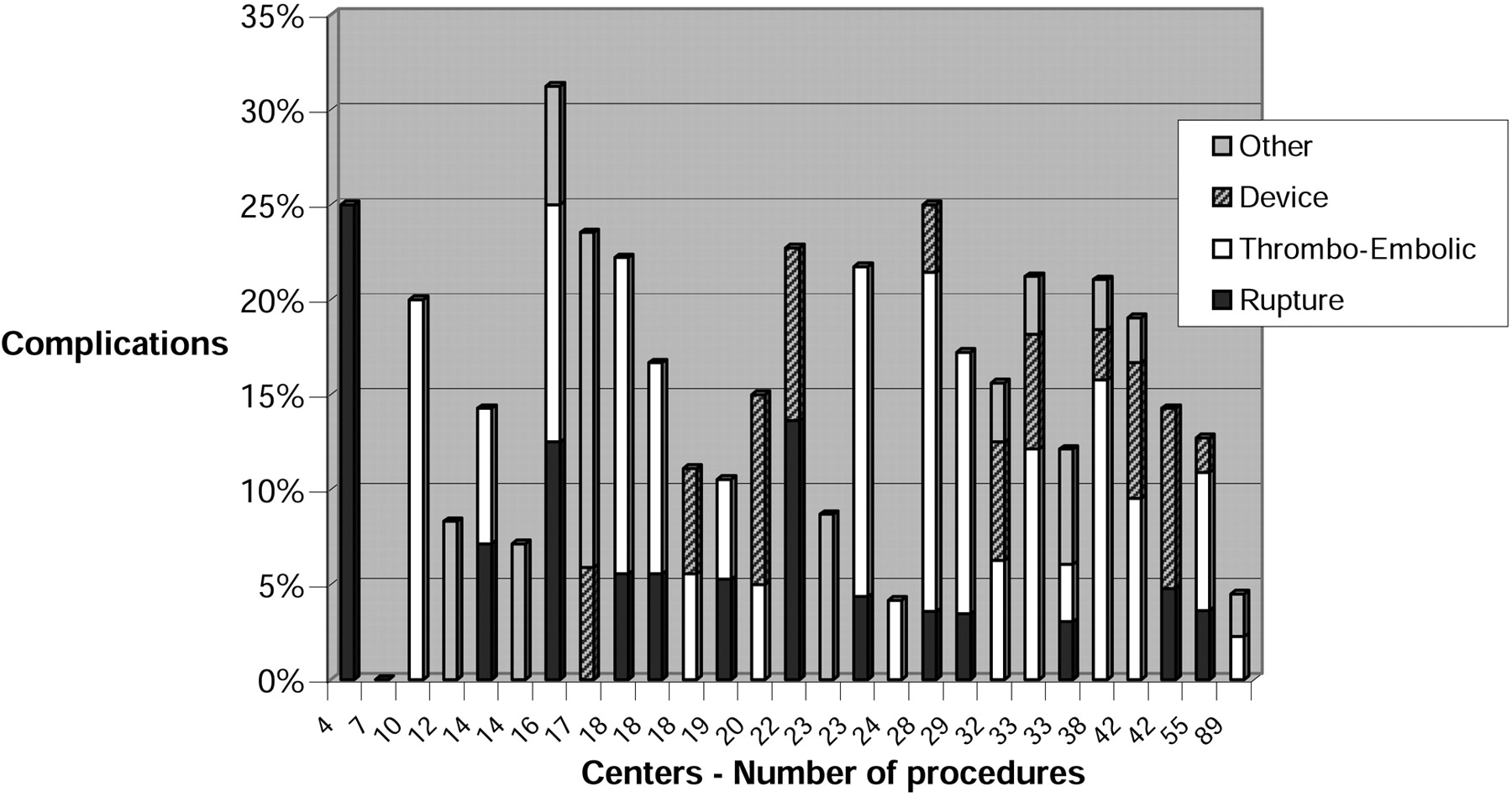
The global rate of adverse events was not significantly different in groups A and B (16.0% and 14.4%, respectively) (Fig 1 and Table 4). Similarly, the rate of specific adverse events (thromboembolism and intraoperative rupture and device-related complication) was not significantly different in groups A and B (12.8% and 12.5%, respectively). Thromboembolic events and intraoperative rupture were not significantly different in group A than in group B (Table 4).

{kind=link}
Adverse events rate in relation to the number of procedures in each center.
Adverse events (per procedure) in centers with low (group A) and high (group B) numbers of cases/hospital
One-Month Clinical Results
One-month mortality and morbidity rates were not significantly different in groups A and B (Table 5).
Morbidity and mortality in centers with low (group A) and high (group B) numbers of cases/hospital
Duration of the Hospital Stay
The median of duration of a hospital stay was the same in each group:
Anatomic Results
The postoperative aneurysmal occlusion was not significantly different in groups A and B (Table 6).
Anatomic results (per aneurysm) in centers with low (group A) and high (group B) numbers of cases/hospital
Discussion
The ATENA study was conducted in 27 neurointerventional centers in France and Canada from June 2005 to October 2006. It showed that the endovascular treatment of unruptured intracranial aneurysms was feasible in a high percentage of cases with low morbidity and mortality rates. However, an important unanswered question was whether the results were similar among centers that treated high and low volumes of patients—that is, it was unknown whether the treatment in a center with a high volume of cases was associated with a better outcome.
Previously, patients with ruptured or unruptured aneurysms with surgery or endovascular treatments have been studied to evaluate the relationships between physician experience, volumes of patients treated, and clinical and anatomic outcomes.3–9 Most series were based on a retrospective analysis of a data base of hospital discharges and were fraught with the limitations of this type of evaluation.
Previous analyses were conducted in the patient population that had been treated surgically. Solomon et al3 reviewed all discharges in the state of New York from 1987 to 1993 that had been recorded in the Statewide Planning and Research Cooperative System of the New York Department of Health. They analyzed the outcomes of all patients who underwent craniotomy for cerebral aneurysms (n = 4034). They found that hospitals that performed >30 craniotomies per year had a 43% lower mortality rate than hospitals that performed fewer craniotomies (8.8% versus 15.5% mortality rates, respectively). They found similar results for patients who underwent craniotomy for unruptured cerebral aneurysms. Hospitals that performed >30 craniotomies per year had a 43% lower mortality rate than hospitals that performed fewer craniotomies (4.6% versus 8.1% mortality rates, respectively). Similar results were reported for older patients with ruptured aneurysms treated by the surgical approach.4 The 30-day mortality rates for patients with subarachnoid hemorrhage who were treated surgically were 20.5%, 18.4%, and 14.3% in hospitals averaging <1, between 1 and 5, and ≥5 interventions per year, respectively. Similar results were observed in a more recent series that studied mortality and morbidity after surgical treatment of unruptured intracranial aneurysms in the United States (1996–2000). The hospitals that treated ≥20 patients/year had fewer adverse outcomes (15.6%) and lower mortality rates (1.6%) compared with hospitals with <4 cases/year (23.8% adverse outcomes and a 2.2% mortality rate).8
One study analyzed the effects of endovascular services and volume of cases/hospital on cerebral aneurysm treatment outcomes. They showed that patients were less likely to die in the hospital when treated at institutions that more frequently used coil embolization and angioplasty for vasospasm.5 However, the volume of cases/hospital was not independently associated with in-hospital deaths. Johnston et al6 analyzed the data base from the Office of Statewide Health Planning and Development of California for the period of 1990–1998. They showed that compared with surgery, endovascular therapy of unruptured aneurysms was associated with a lower risk of adverse outcomes and in-hospital deaths. The volume of cases/hospital was also associated with outcome.
A subsequent analysis of patients treated for ruptured or unruptured aneurysms was conducted in New York State. Again, that study showed that the volume of cases/hospital and the propensity of a hospital to use endovascular therapy were both independently associated with better outcomes.7 In cases that involved clipping of either ruptured and unruptured aneurysms, a higher volume of cases/hospital was associated with a better outcome. In cases that involved embolization, the volume of cases/hospital was either not significantly associated with outcome or demonstrated a statistically weaker association than clipping. In addition, Hoh et al9 conducted a retrospective cohort study with the Nationwide Inpatient Sample of 1996–2000. They demonstrated that hospitals with >23 admissions per year had fewer adverse outcomes (5.2%) than hospitals with <4 admissions per year (17.6%). The mortality rate was lower at hospitals with high volumes of cases (1.0% versus 3.7%), but the difference was insignificant. Finally, the length of stay was shorter at hospitals with high volumes of cases.
We used a completely different approach in our analysis of the relationship between the volume of cases/hospital and the outcome of endovascular treatment for UIA. We did not use a discharge data base but the results from a prospective consecutive multicenter controlled study. This methodology can avoid much of the bias that might be encountered in a retrospective analysis of a discharge data base, but it is also associated with some limitations (see below). The population of the ATENA study was divided into 2 groups according to the volume of cases/hospital. The groups were defined to ensure approximately the same number of centers in each group. Group A included 13 centers that treated ≤20 patients, and group B included 14 centers that treated >20 patients during the inclusion period. With other cut-points (see “Materials and Methods”), similar results were obtained (not shown). Although the patient and aneurysm characteristics were similar in both groups, the endovascular treatment was performed differently in groups A and B. The standard coiling technique was more frequently used in group A (62.4% versus 50.4% in group B, P = .001), and stent placement was more frequently used in group B (9.6% versus 2.5% in group A, P = .0016). These results suggested that centers with high volumes of cases may facilitate the use of complex techniques like stent placement.
The most important factor in evaluating any treatment is certainly clinical outcome, as assessed by morbidity and mortality. Morbidity was not significantly different in groups A and B (1.8% and 1.7%, respectively). The mortality rate was higher in group A (2.3% versus 1%), but the difference was not significant. Hoh et al9 reported somewhat different outcomes. They found that discharge to a facility other than home occurred at a rate of 5.2% from hospitals with high volumes of cases compared with 17.6% from hospitals with low volumes of cases. However, with findings similar to ours, they reported a lower mortality rate at hospitals with high volumes of cases (1.0% versus 3.7%), but the difference was not significant.
Several factors may explain the discrepancies between studies. Our series was conducted more recently (2005–2006) and during a shorter period than the analysis of Hoh et al (1996–2000).9 Endovascular treatment started in France in 1993–1994; thus, most teams participating in the ATENA study had long experience with the endovascular treatment of unruptured aneurysms. This was probably not the case in the series of Hoh et al. Moreover, the development of more appropriate devices (coils, microcatheters, microguidewires, etc) has facilitated the performance of endovascular treatments. Also, the series of Hoh et al included a very large (81) number of centers compared with the number included in our series (27); thus, the levels of clinical experience were presumably more heterogeneous in the series of Hoh et al. Finally, we defined high- and low-volume hospitals differently than Hoh et al did. They defined high-volume hospitals as those with >23 admissions per year and low-volume hospitals as those with <4 admissions per year; in contrast, we defined high- and low-volume hospitals as those with greater or less than 20 admissions during 17 months, respectively.
We found that the anatomic outcomes were similar in both groups. Despite the difference in treatment techniques (see above), the relative percentages of complete occlusion, neck remnant, and aneurysm remnants were not different in groups A and B. However, this result was based on the occlusion rates determined by the practitioners that performed the procedures. A core lab analysis of anatomic results is necessary to confirm that the results were similar in both groups.
Our study had several limitations. First, it was not possible to evaluate the results according to the physician volume. Because 1, 2, or more physicians can be involved in the treatment of a single patient, it was not possible to calculate the physician volume by simply dividing the number of patients treated by the number of physicians in each center. Second, it was not possible to evaluate the effect of physician experience because we had no information regarding the years of experience or the number of unruptured aneurysms treated before the study for each physician. It was previously shown that the risk of complications with coil embolization of unruptured aneurysms was dramatically reduced with physician experience.11 Third, we were unable to take into account the global experience within each center for the treatment of intracranial aneurysms, including ruptured aneurysms, and of neurovascular procedures in general. Finally, our definitions of high- and low-volume centers for groups A and B were arbitrary; in fact, there is a continuum from group A to group B, and this may partially explain our results. However, results were similar whatever the cut-point used to define the low and high-volume centers.
Summary
Our analysis demonstrated that at least in France (and Canada), clinical and anatomic outcomes of endovascular treatments for unruptured intracranial aneurysms are similar in centers with low and high volumes of cases/hospital. This is probably related to the fact that most neurointerventional teams participating in ATENA have had long intensive experience with the endovascular treatment of intracranial aneurysms (unruptured and ruptured).
Appendix
Participating Centers and Investigators
CHU Larrey, Angers, France; Anne Pasco
C HU Jean Minjoz, Besançon, France; Jean-François Bonneville
CHU Pellegrin, Bordeaux, France; Xavier Barreau, Jérôme Berge
CHU de la Côte de Nacre, Caen, France; Patrick Courthéoux, Suzana Saleme
CHU Gabriel Montpied, Clermont Ferrand, France; Emmanuel Chabert, Jean Gabrillargues
CH Louis Pasteur, Colmar, France; Alain Tournade
CHU Hôpital General, Dijon, France; Frédéric Ricolfi
CHU Albert Michallon, Grenoble, France; Pierre Bessou
CHU Roger Salengro, Lille, France; Xavier Leclerc, Jean-Pierre Pruvo, Christian Taschner
CHU La Timone, Marseille, France; Olivier Lévrier
CHU Gui de Chauliac, Montpellier, France; Alain Bonafé
CHUM Notre-Dame, Montréal, Canada; Jean Raymond, Daniel Roy, Alain Weill
CHU Hôpital Neurologique, Nancy, France; René Anxionnat, Serge Bracard, Luc Picard
CHU G et R Laënnec, Nantes, France; Hubert Desal, Axel de Kersaint-Gilly
CHU Kremlin-Bicêtre, Kremlin-Bicêtre, France; Hortensia Alvarez, Pierre Lasjaunias, Augustin Ozanne
CH Foch, Suresnes, France; Anne Boulin, Georges Rodesch
CHU La Pitié Salpêtrière, Paris, France; Alessandra Biondi, Fabrice Bonneville, Betty Jean, Nader Sourour
CHU Mondor, Créteil, France; Raphaël Blanc, André Gaston
CH Fondation Rothschild, Paris, France; Guido Lazzarotti, Manoel Maia Filho, Jacques Moret, Charbel Mounayer, Michel Piotin, Christiana Queiroz, Laurent Spelle
CH Sainte-Anne, Paris, France; Sylvie Gordon-Hardy, Jean-François Meder, Denis Trystram
CHU de la Milétrie, Poitiers, France; Jacques Drouineau
CHU Maison Blanche, Reims, France; Sophie Gallas, Laurent Pierot
CHU Bellevue, Saint-Etienne, France; Fabrice-Guy Barral, Luis Manera
CHU Hautepierre, Strasbourg, France; Rémy Beaujeux
CH Sainte-Anne, Toulon, France; Charles Arteaga
CHU Purpan, Toulouse, France; Christophe Cognard, Anne-Christine Januel, Philippe Tal
CHU Bretonneau, Tours, France; Denis Herbreteau
Footnotes
-
Indicates Editor's Choices selection
-

-
This work was supported by the French Society of Neuroradiology.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- Received June 27, 2009.
- Accepted after revision November 20, 2009.
- Copyright © American Society of Neuroradiology