Abstract
SUMMARY: A PTMC is defined as a thyroid papillary cancer that measures ≤10 mm in the greatest diameter. The detection rate for a PTMC has increased because of the worldwide use of high-resolution sonography and US-FNAB. We report a case of a 1-mm-diameter PTMC confirmed at thyroidectomy for which the cytologic diagnosis had an important role in deciding the extent of surgery (ie, either a total thyroidectomy or a hemithyroidectomy).
Abbreviations
- ATA
- American Thyroid Association
- HE
- hematoxylin-eosin
- PTC
- papillary thyroid carcinoma
- PTMC
- papillary thyroid microcarcinoma
- US-FNAB
- sonography-guided fine-needle aspiration biopsy
AUS-FNAB is a widely used procedure for the cytological evaluation of thyroid nodules. However, US-FNAB of a thyroid nodule <10 mm in maximal diameter seems to be limited because of a poor clinical significance and social-medical-cost problem. We report a case of 1 mm diameter PTMC that was diagnosed on US-FNAB and this cytological diagnosis influenced the decision of thyroid surgery type.
Case Report
A 43-year-old woman who had recently complained of fatigue and neck discomfort was referred to the radiology department from the department of general surgery for sonographic evaluation of the thyroid. The patient showed normal values on a thyroid function test (T3, 1.3 nmol/L; free T4, 11.6 pmol/L; thyroid-stimulating hormone, 1.03 mU/L), and no specific abnormalities were detected on a physical examination of the neck. The patient had neither previously undergone a fine-needle biopsy for a thyroid lesion nor had a history of neck irradiation or surgery or a family history of a thyroid malignancy.
A thyroid nodule that showed marked hypoechogenicity, an ill-defined margin, and a taller-than-wide shape was identified in the left lobe on thyroid sonography. The nodule measured 5.5 mm in the maximal diameter and was considered to be highly suspicious for a malignancy (Fig 1 A). A hypoechoic thyroid nodule that measured 1.0 mm in maximal diameter was detected in the medial aspect of the opposite right midlobe on a simultaneous diagnostic sonography examination, and this nodule was considered as an “indeterminate” nodule for a malignancy (Fig 1B). In addition, several thyroid nodules that showed benign sonographic features were observed in both lobes.

{kind=link}
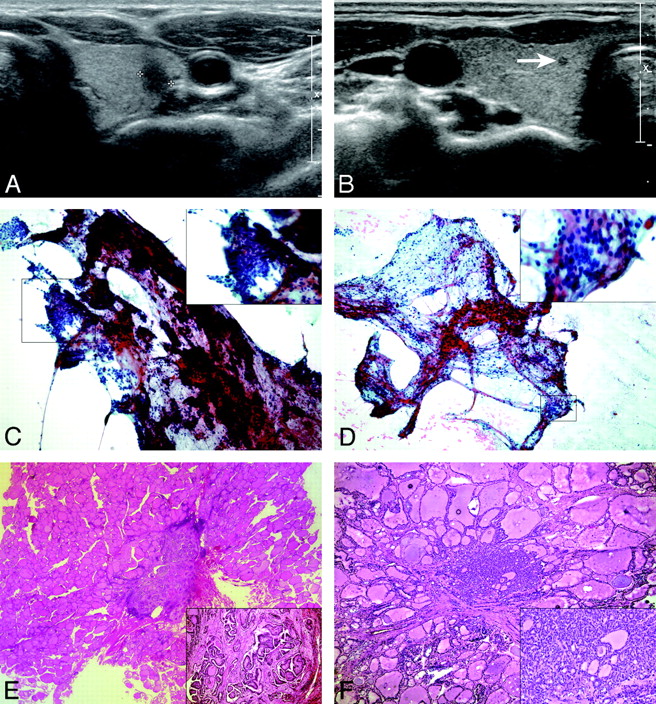
A, A transverse sonogram shows a 5.5-mm-diameter solid thyroid nodule (calipers) with marked hypoechogenicity, an irregular margin, and a taller-than-wide shape located in the left thyroid lobe. B, A transverse sonogram shows a 1.0-mm-diameter solid thyroid nodule with hypoechogenicity in the right thyroid lobe (arrow). C, On aspiration cytology of left thyroid nodule, many 3D papillary or caplike structured clusters are noted. The characteristic nuclear features of papillary carcinoma, including fine and powdery chromatin and irregular nuclear membranes with nuclear grooves, are noted in most nuclei (Papanicolaou, original magnification ×100 [inset, ×400]). D, Aspiration cytology of the right thyroid nodule reveals a few small aggregates of follicular cells within some lymphocytes. The follicular cells reveal nuclear clearing and grooves suspicious for papillary carcinoma (Papanicolaou, original magnification ×100 [inset, ×400]). E, On higher magnification of left thyroid nodule, the papillary arrangement is well recognized and is considered a classic type of PTMC (HE, original magnification ×40 [inset, ×100]). F, Right thyroid nodule reveals a follicular variant of PTMC, which is composed of follicles having nuclear features of papillary carcinoma on a frozen-section slide (HE, original magnification ×10 [inset, ×100]).
A US-FNAB was performed by 1 investigator (D.W.K.) on the 2 nodules that showed a likelihood of being thyroid malignancies. Only 1 sampling was achieved for each thyroid nodule, without the administration of local anesthetic. A US-FNAB was not performed on several other thyroid nodules suggestive of being benign lesions on thyroid sonography because the selection of a nodule for US-FNAB was based primarily on the sonographic features rather than the nodule size. The patient had no significant pain or other complications following the US-FNAB procedure. On the basis of the cytology results, a nodule highly suspicious for a malignancy in the left lobe was identified as compatible with PTC (Fig 1C), and a 1-mm right-lobe nodule suspicious for a malignancy on thyroid sonography was also identified as suspicious for PTC (Fig 1D).
Although the primary PTC had a maximal diameter of 5.5 mm and an intraglandular location, the surgeon and the patient chose a total thyroidectomy rather than a left hemithyroidectomy on the basis of the cytology findings. On pathology, the tiny malignancy in the right thyroid lobe measured 1.5 mm in maximal diameter at gross and microscopic examinations. On the pathologic findings, PTMCs in left and right thyroid lobes were a classic type and follicular variant, respectively (Fig 1E, -F). These 2 PTMCs showed no capsular or nodal invasion in the perithyroidal areas. In addition, several thyroid nodules that had showed benign features on thyroid sonography in both lobes were determined to be nodular hyperplasia at microscopic findings. After thyroid surgery, the patient has undergone follow-up and has not had any problems related to the thyroid malignancy or the surgery.
Discussion
A PTMC is defined as a PTC <10 mm in the maximal diameter. The detection and incidence rates of PTMCs have increased recently with the worldwide use of thyroid sonography and US-FNABs, and there have been many reports related to the diagnostic efficacy of US-FNAB for PTMCs.1–6 The ATA guidelines and the Society of Radiologists in Sonography Consensus Statement suggest that, in general, only nodules >10 mm in diameter should be evaluated because these nodules have the potential to represent a clinically significant cancer.7,8 However, both the ATA and Society of Radiologists in Sonography Consensus Statement suggest performing US-FNAB on thyroid nodules ≥10 mm in maximal diameter when the nodules exhibit sonographic features associated with thyroid cancer. Recently, Roti et al9 reported that this incidence of bilaterality of a PTMC is 19%. This suggests that incomplete treatment would occur in 19% of patients if only hemithyroidectomy was performed. Therefore, we believe that an accurate evaluation of satellite malignancy in an opposite thyroid lobe through sonographic diagnosis and US-FNAB of the thyroid nodule is necessary.
The sampling technique for US-FNAB of small thyroid nodules <5 mm in maximal diameter is the same as that for thyroid nodules >5 mm in maximal diameter. After the needle tip is placed in the appropriate area of the target nodule, the sampling begins by using the “mixed sampling technique,”6,10 in which the needle is moved up and down for a few seconds only by movement of the operator's wrist and without initial aspiration under sonographic guidance. When the hub of the needle is filled with the proper amount of material, the syringe-needle unit should be rapidly withdrawn. However, if no aspirates are obtained after a few seconds of capillary sampling, negative pressure can gradually be added by use of the first finger of the right hand. This to-and-fro needle movement should be continued during the entire sampling procedure. Only 1 sampling is achieved in most of the US-FNABs for thyroid nodules by using 1 needle puncture and without local anesthesia.
The smear technique is as follows: The operator expels the contents of the needle hub onto 1 or 2 slides for smear preparation after filling the empty syringe with room air. Two-to-4 slides are then obtained by duplicating the smear. Finally, a special technique is used in which the operator flips the plastic hub of the needle onto the slide for effective cell acquisition of the remaining material in the needle hub.10
One of the investigators (D.W.K.) has performed US-FNAB for small thyroid nodules <5 mm in maximal diameter when a nodule has shown the likelihood of a malignancy on diagnostic thyroid sonography.6 In particular, US-FNAB has been performed for small thyroid nodules regardless of the nodule size when it is necessary to determine the type of thyroid surgery (a total thyroidectomy or hemithyroidectomy), if the primary thyroid malignancy is a PTC and is <10 mm in maximal diameter. Our present patient had a small thyroid nodule in the left thyroid lobe that was considered highly suspicious for a malignancy as well as a tiny nodule in the right thyroid lobe that was considered indeterminate for a malignancy on thyroid sonography. The patient underwent a total thyroidectomy based on cytologic findings after a successful US-FNAB for each nodule.
In conclusion, we report a case of a 1-mm-diameter PTMC that was diagnosed by cytology after US-FNAB and confirmed after thyroidectomy. The use of US-FNAB for a 1-mm-diameter thyroid nodule influenced the decision regarding the most appropriate type of thyroid surgery technique.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- Received April 14, 2009.
- Accepted after revision July 25, 2009.
- Copyright © American Society of Neuroradiology