Abstract
SUMMARY: Our aim was to compare the detectability of aneurysmal wall enhancement in unruptured intracranial aneurysms between conventional and motion-sensitized driven equilibrium–prepared postcontrast 3D T1-weighted TSE sequences (sampling perfection with applicationoptimized contrasts by using different flip angle evolution, SPACE). Twenty-two patients with 30 unruptured intracranial aneurysms were scanned at 3T. Aneurysmal wall enhancement was more significantly detected using conventional compared with motion-sensitized driven equilibrium–prepared SPACE sequences (10/30 versus 2/30, P < .0001). Contrast-to-noise ratio measurements did not differ between conventional and motion-sensitized driven equilibrium–prepared sequences (P = .51). Flowing blood can mimic aneurysmal wall enhancement using conventional SPACE sequences with potential implications for patient care.
ABBREVIATIONS:
- AWE
- aneurysmal wall enhancement
- CNR
- contrast-to-noise ratio
- MSDE
- motion-sensitized driven equilibrium
- SPACE
- sampling perfection with application-optimized contrasts by using different flip angle evolution
- UIA
- unruptured intracranial aneurysm
Vessel wall MR imaging is being increasingly used in patients with intracranial aneurysms,1 with aneurysmal wall enhancement (AWE) considered suggestive of instability/rupture.2⇓⇓⇓⇓⇓–8 The most commonly used sequence for vessel wall MR imaging is 3D TSE, including a black-blood effect9; however flowing blood can still lead to lumen enhancement.1,8
Motion-sensitized driven equilibrium (MSDE) uses flow-sensitive dephasing gradients to suppress residual blood flow.10 For the evaluation of AWE, only 1 recent study used MSDE,6 while all the other studies2⇓–4,7,11⇓⇓–14 used a postcontrast sequence without any additional blood-suppression technique (conventional sequence).
The influence of blood-suppression techniques on the detectability of AWE has not yet been evaluated, to our knowledge. We aimed to compare the detectability of AWE in consecutive patients with unruptured intracranial aneurysms (UIAs) using conventional and an MSDE-prepared postcontrast 3D TSE sequence (sampling perfection with application-optimized contrasts by using different flip angle evolution, SPACE).
Materials and Methods
Patients and Brain Imaging
This study was approved by the institutional review board of the Rothschild Foundation Hospital, Paris, France. From September 2016 to February 2017, twenty-two consecutive patients (17 women; 58.1 years of age; range, 25–85 years) with 30 asymptomatic UIAs were included. All patients underwent both DSA and 3T MR imaging within 1 week. Aneurysms were considered nonruptured on the basis of clinical (absence of recent or past acute headaches, no history of subarachnoid hemorrhage) and imaging (absence of recent or past SAH on FLAIR and SWI) data.
MR imaging was performed at 3T (Magnetom Skyra; Siemens, Erlangen, Germany) including DWI, FLAIR, SWI, TOF-MRA, contrast-enhanced MRA, and pre- and postcontrast 3D T1-weighted SPACE acquired with and without MSDE (4 acquisitions per patient). The order of the postcontrast SPACE sequence was randomized. SPACE parameters were similar to those in previous studies2,4,11,12: sagittal plane: TR/TE, 700/11 ms; slice thickness, 0.9 mm; FOV, 230 × 230 mm; matrix, 256 × 256 (interpolated to 512 × 512); voxel size, 0.45 mm; acquisition time, 4 minutes 33 seconds. MSDE preparation consisted of a first-order gradient moment of 500 mT × ms2/m and a b-value of 1.75 s/mm2, according to a previous study.10
Image Analysis
UIAs were defined in consensus using DSA images by 2 neuroradiologists (R.B. and E.K.). SPACE images were blindly and independently assessed in multiplanar mode (with image analysis in arbitrary planes) by 3 neuroradiologists: J.H., T.T., and A.C. Readers were blinded to clinical data and other sequences (except TOF-MRA) but were aware of patient aneurysm location.
Two independent blinded-reading sessions took place 2 weeks apart to avoid recall bias. Each UIA was analyzed only once per session, with pre- and postcontrast either conventional or MSDE-prepared SPACE sequences. For each of the 2 sets of SPACE acquisitions, the readers evaluated each UIA for AWE defined as a thick (>2 mm) area of aneurysmal wall with increased signal intensity between pre- and postcontrast images. Discrepancies were resolved by consensus.
Contrast-to-noise ratio (CNR) measurements were performed to ensure that the differences observed between SPACE sequences were not artifactual. Standardized ROIs (same size and location) were drawn within the following: 1) aneurysm lumen, 2) brain parenchyma, 3) anterior pituitary gland (ie, T1-enhancing tissue), and 4) background noise. CNR was measured in comparison with the parenchyma [CNR = (SI1 − SI2)/SDnoise] for aneurysm lumen and pituitary gland, with SI indicating signal intensity.
Statistical Analysis
Interobserver agreement was evaluated (Fleiss κ). Occurrence of AWE in the whole cohort and CNR values were compared between conventional and MSDE-prepared SPACE images (Fisher exact and paired t test, respectively).
Results
Thirty UIAs (mean long axis, 6.5 mm; range, 2.5–16 mm; mean short axis, 4.6 mm; range, 2–13 mm) were visible in the 22 patients (1.4 per patient; maximum, 4), affecting the basilar (n = 1), anterior cerebral (n = 1), middle cerebral (n = 10), anterior communicating (n = 8), or internal carotid artery (n = 10), including ophthalmic (n = 4) and intracavernous (n = 2) carotid segments.
Interrater agreement was almost perfect (κ = 0.87; 95% CI, 0.72–1.00; and κ = 0.81; 95% CI, 0.63–0.98) with conventional and MSDE-prepared SPACE images, respectively.
AWE was more frequently detected using a conventional (10/30 UIAs, 33.3%) than the MSDE-prepared (2/30, 6.7%) SPACE sequence (P < .0001). AWE was found using both sequences in 2 UIAs (Fig 1) and only with conventional SPACE in 8 with a circumferential appearance (Fig 2).

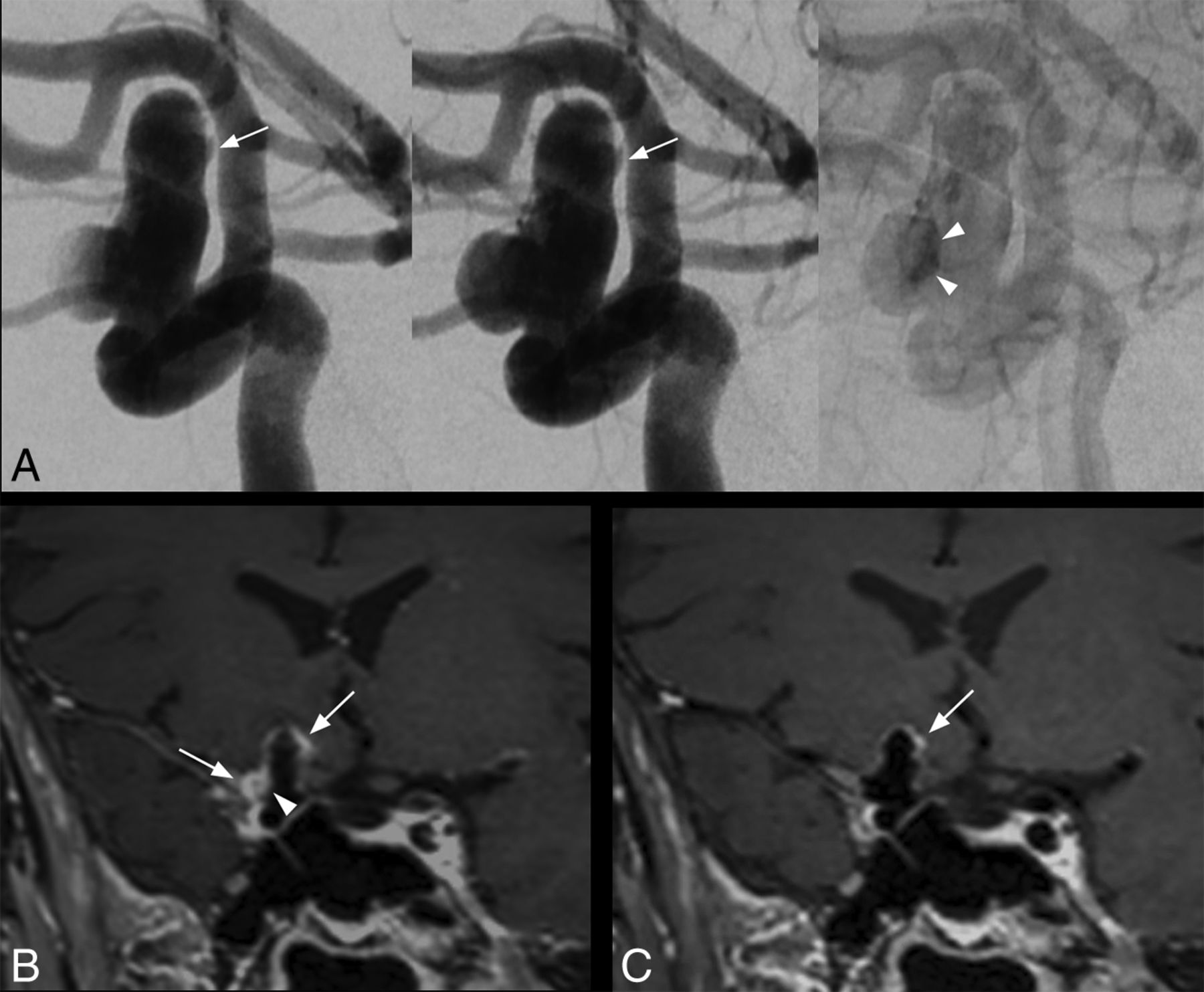
Saccular intracranial aneurysm in a 63-year-old patient. DSA angiogram (A, from left to right: early arterial phase, arterial phase, and venous phase) shows a 14-mm right internal carotid artery aneurysm with intrasaccular slow flowing/stagnant blood (arrowheads) and irregular shape (arrow). With conventional SPACE imaging (B), extensive AWE is visible, more prominent at the apex and at the lateral portion of the aneurysm (B, arrows). Note the enhancement within the aneurysm lumen visible only using conventional SPACE imaging (B, arrowhead), matching the stagnant blood on DSA (A, arrowheads). With MSDE SPACE imaging, AWE is only visible at the apex (C, arrow).

{kind=link}
{kind=link}
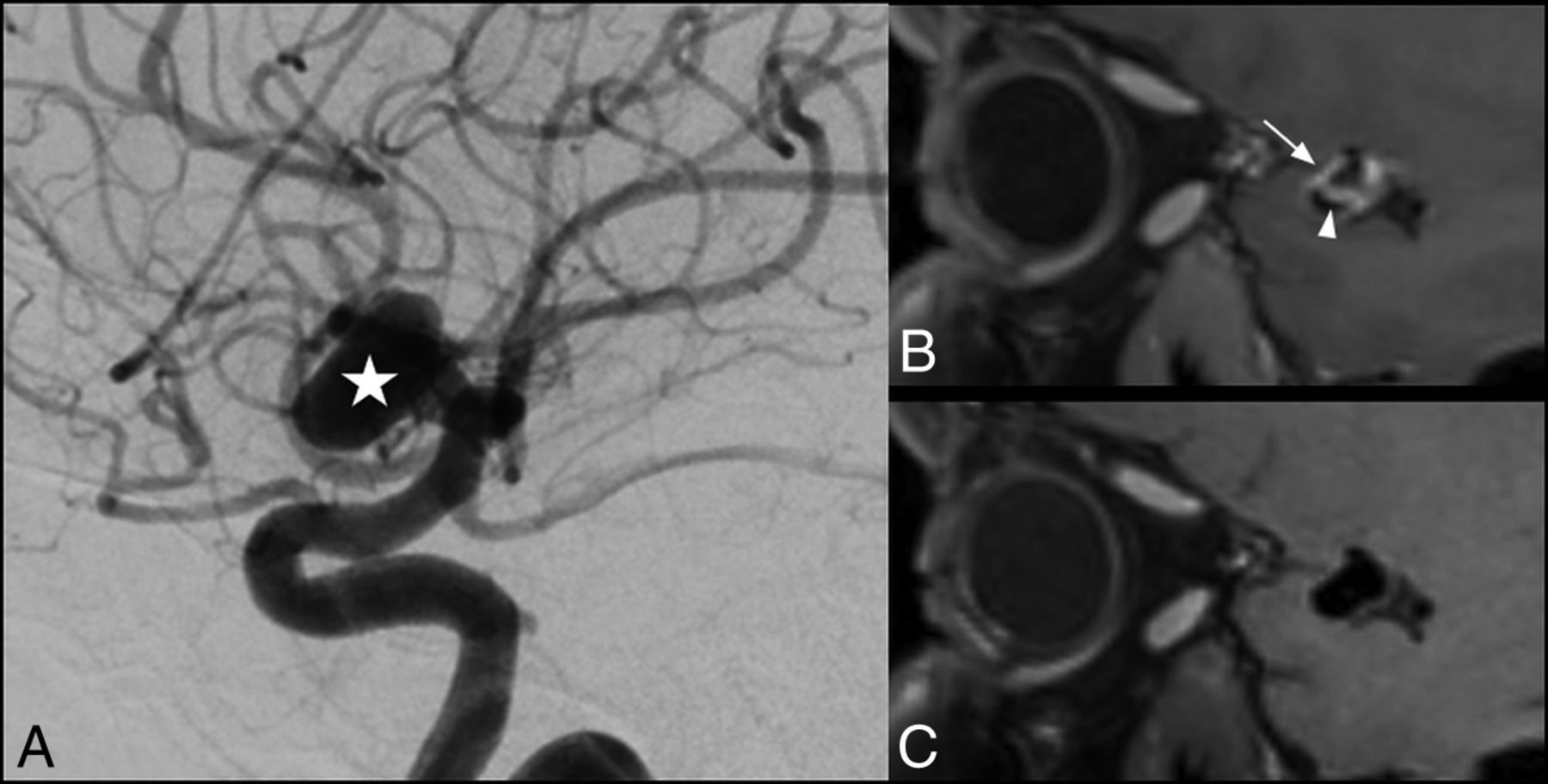
Saccular intracranial aneurysm in a 42-year-old patient. DSA angiogram shows an 11-mm aneurysm (A, star) arising from the M1 segment of the right middle cerebral artery. AWE is visible on the conventional SPACE image (B, arrow), while there is no enhancement visible on the corresponding MSDE SPACE image (C). Enhancement within the aneurysm lumen was also visible using a conventional SPACE image (B, arrowhead).
CNR did not differ between the 2 SPACE sequences for the pituitary gland (ie, T1-enhancing tissue) (321.9 ± 103.7 versus 304.8 ± 60.4 for conventional and MSDE-SPACE, respectively, P = .51) and was higher for the aneurysm lumen with MSDE-prepared SPACE sequences (102.4 ± 83.1 versus 180.2 ± 36.4, P = .008).
Discussion
MSDE preparation reduced the occurrence of AWE, suggesting flowing blood mimicking AWE on conventional images. Such pitfalls may have biased previous studies evaluating AWE and could also have implications for patient care.
Double inversion recovery, MSDE,10 or delay alternating with nutation for tailored excitation (DANTE) can be used for vessel wall MR imaging. We performed MSDE, considering its excellent blood suppression and adaptability to 3D imaging readout (while double inversion recovery is time-consuming and not easily adaptable for large-FOV 3D imaging). Low first-order gradient moment/b-values and composite pulses were used to avoid signal loss and eddy current effects, respectively.
With conventional SPACE sequences, our results (AWE in 33.3% of UIAs) were similar to those previously published.2 The rate of AWE was lower (6.7%) using MSDE, similar to that of Nagahata et al6 also using this technique (4.8% of UIAs). AWE detected using MSDE-prepared SPACE sequences can be related to wall inflammation and/or alternatively to an incomplete suppression of flowing blood not yet degraded by gradients. Such slow inflows may also be associated with degenerative remodeling and thus aneurysm growth.15
There is conflicting evidence on the relationship between AWE and aneurysm size. Some studies found no relationship between wall enhancement and aneurysm size,2,4 with others demonstrating a positive correlation.12 Considering our results, such discrepancy could be due to the relationship between intrasaccular flowing blood and aneurysm size.2,12
Limitations include a small number of patients and lack of histopathologic analysis (reference standard for AWE) because patients did not undergo an operation. However, our purpose was not to assess accuracy for the diagnosis of wall inflammation because we aimed to evaluate the influence of MSDE on AWE detectability. We focused only on UIA; further studies including patients with ruptured aneurysms with histologic analysis available may demonstrate the advantages of MSDE preparation.
ACKNOWLEDGMENTS
We thank Aurélien Monnet and Wadie Ben Hassen from Siemens Healthineers for their support.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- Received January 29, 2018.
- Accepted after revision February 5, 2018.
- © 2018 by American Journal of Neuroradiology