Abstract
BACKGROUND AND PURPOSE: An “unwound” or “offset” cochlea has been described as a characteristic imaging feature in patients with branchio-oto-renal syndrome, and recently recognized to be associated in particular to those with EYA1 gene mutations. Determination of this feature has traditionally relied on subjective visual assessment. Our aim was to establish an objective assessment method for cochlear offset (the cochlear turn alignment ratio) and determine an optimal cutoff turn alignment ratio value that separates individuals with EYA1-branchio-oto-renal syndrome from those with SIX1-branchio-oto-renal syndrome and healthy controls.
MATERIALS AND METHODS: Temporal bone CT or MR imaging from 40 individuals with branchio-oto-renal syndrome and 40 controls was retrospectively reviewed. Cochlear offset was determined visually by 2 independent blinded readers and then quantitatively via a standardized technique yielding the cochlear turn alignment ratio. The turn alignment ratio values were compared between cochleae qualitatively assessed as “not offset” and “offset.” Receiver operating characteristic analysis was used to determine the ability of the turn alignment ratio to differentiate between these populations and an optimal cutoff turn alignment ratio value. Cochlear offset and turn alignment ratio values were analyzed for each branchio-oto-renal syndrome genotype subpopulation and for controls.
RESULTS: The turn alignment ratio can accurately differentiate between cochleae with and without an offset (P < .001). The optimal cutoff value separating these populations was 0.476 (sensitivity = 1, specificity = 0.986, J = 0.986). All except 1 cochlea among the EYA1-branchio-oto-renal syndrome subset and all with unknown genotype branchio-oto-renal syndrome had a cochlear offset and a turn alignment ratio of <0.476. All except 1 cochlea among the SIX1-branchio-oto-renal syndrome subset and all controls had no offset and a turn alignment ratio of >0.476.
CONCLUSIONS: There is a statistically significant difference in turn alignment ratios between offset and nonoffset cochleae, with an optimal cutoff of 0.476. This cutoff value allows excellent separation of EYA1-branchio-oto-renal syndrome from SIX1-branchio-oto-renal syndrome and from individuals without branchio-oto-renal syndrome or sensorineural hearing loss. The turn alignment ratio is a reliable and objective metric that can aid in the imaging evaluation of branchio-oto-renal syndrome.
ABBREVIATIONS:
- BOR
- branchio-oto-renal syndrome
- ROC
- receiver operating characteristic
- TAR
- turn alignment ratio
Branchio-oto-renal syndrome (BOR) is a cause of hearing loss with autosomal dominant inheritance, first described in 1975 in a family with hearing loss, cup-shaped anteverted pinnae, preauricular pits, branchial fistulas, and renal dysplasia.1 Cochlear hypoplasia was later noted on tomography.2 Since then, with the advent of CT and MR imaging, much more has been described in the literature of characteristic features of the temporal bone among patients with BOR, most notably an “unwound” or “offset” appearance of the cochleae,3,4 in which small middle and apical turns are anteriorly offset and appear separated from the basal turn. Most recently, it was shown that the offset appearance of cochlear middle and apical turns is indeed a distinctive finding among patients with BOR, but only among those with EYA1 gene mutations having the EYA1 genotype-phenotype; patients with SIX1 mutations have different phenotypes without cochlear offset, but the apical turns have a protuberant “thorny” appearance.5 The differing genotype-phenotype correlation could be related to different functions of the SIX1 and EYA1 genes, and the different sites of expression and roles of the resultant proteins in the cochlea during the embryologic development of the inner ear. Recognition of these distinct phenotypes on imaging and knowledge of the respective genotype-phenotype correlation offers a powerful tool to radiologists, who can then suggest a genetic diagnosis in the context of a potential syndromic presentation compatible with BOR.5
With regard to the offset cochleae seen among patients with EYA1-BOR, prior description and determination of this feature in the literature has been based on visual assessment.3,4,6 This presumes familiarity with normal cochlear morphology, in order to recognize when the middle and upper turns of the cochleae are anteromedially displaced by a degree that is more than expected for the typical normal cochlea. However, this recognition may be challenging for radiologists who do not regularly interpret temporal bone imaging, and there may be other conditions in which the cochlear turns are not aligned normally or where the turns may not be sufficiently offset to raise the suspicion for EYA1-BOR syndrome or another anomaly.
The aim of this study was to define and quantify the cochlear turn alignment ratio (TAR), to analyze the TAR among both cochleae with offset and cochleae without offset as visually assessed by expert head and neck radiologists (the traditional/usual method of assessment), and to determine whether there is a distinct TAR cutoff value that distinguishes the 2 groups. We then examined the cochleae of patients with EYA1-BOR, those with SIX1-BOR, patients with BOR of unknown genetic association, and controls without evidence of sensorineural hearing loss to determine whether there are quantitative TAR cutoff values that can distinguish patients with BOR from healthy controls and patients with EYA1-BOR from those with SIX1-BOR. The goal was to establish objective metrics that can separate these populations from each other. The resultant TAR measurement method and criteria can aid any radiologist in the determination of “how offset is too offset” with objectivity and establish normative TAR values for the normal cochlea.
MATERIALS AND METHODS
Participants
This was a multicenter retrospective review of temporal bone imaging studies among individuals with clinically diagnosed BOR (from the same database we previously used for qualitative comparison of BOR cochlear phenotypes) and controls without BOR or sensorineural hearing loss. For the BOR group, 40 individuals from 4 participating institutions were included; inclusion criteria were a clinical diagnosis of BOR syndrome7 and diagnostic temporal bone CT and/or MR imaging available for review. Among these 40 patients, 16 had known underlying causative EYA1 genetic mutations, 4 had known SIX1 genetic mutations, and 20 had not undergone genetic testing. For the control group, consecutive multidetector row CT scans of 40 patients without clinical or audiometric evidence of sensorineural hearing loss who underwent temporal bone CT for symptoms unrelated to hearing loss (eg, otalgia, otitis media, dizziness, facial palsy) were included. Imaging among the BOR group occurred between April 2001 and April 2021. Imaging among the control group occurred between January 2019 and December 2020. This study was approved by the institutional review board/ethics committee of each institution.
Image Acquisition
BOR Group.
Of the 40 patients, 33 had undergone CT, 6 had undergone MR imaging, and 1 had undergone both CT and MR imaging. All CT scanners across the participating institutions were helical multidetector row scanners (Discovery 750 HD, LightSpeed Pro 16 SYS, HiSpeed CT/i SYS, or HiSpeed RP SYS; GE Healthcare; SOMATOM Sensation 40 or SOMATOM Force SYS; Siemens) with parameters ranging as follows: 120 kV (peak), 100–200 mA, section thickness = 0.6–0.625 mm, some with an overlap of 0.2 mm. All MR imaging scanners across the participating institutions were 3T units, with assessment conducted on the heavily T2-weighted sequence such as 3D driven equilibrium radiofrequency reset pulse (DRIVE; Philips Healthcare), constructive interference in steady state (CISS; Siemens), and T2 sampling perfection with application-optimized contrasts by using different flip angle evolution (T2 SPACE; Siemens). All temporal bone images were uploaded onto the PACS, with axial reformats created in a plane parallel to the plane of the lateral semicircular canal (or estimated to be so in cases when the lateral semicircular canal was anomalous), and coronals perpendicular to these reformatted axials, before image analyses.
Control Group.
Multidetector row CT scanning (Discovery 750 HD) of the temporal bone was performed with 120 kV(p), 240 mA, 0.6-mm section thickness, and 0.2-mm overlap. Axial reformats of the temporal bones were created in a plane parallel to the lateral semicircular canal, and coronals perpendicular to these reformatted axials before image analyses.
Image Review
Two neuroradiologists with 5 (J.P.) and 15 (A.F.J.) years of experience with subspecialty head and neck expertise reviewed all cases and controls. The reviewers were blinded to the original reports, patient demographics, clinical diagnoses including whether there was BOR syndrome, underlying genetic abnormality, and the other reviewer’s findings.
Qualitative Assessment.
The cochleae of all enrolled individuals (patients with BOR and controls) were assessed qualitatively on standardized reformatted axial images in the plane of the lateral semicircular canal. Each cochlea was designated as “with offset” or “without offset” by consensus. Any thorny appearance of the apical turn of the cochlea was also noted as present or absent.5
Quantitative Assessment.
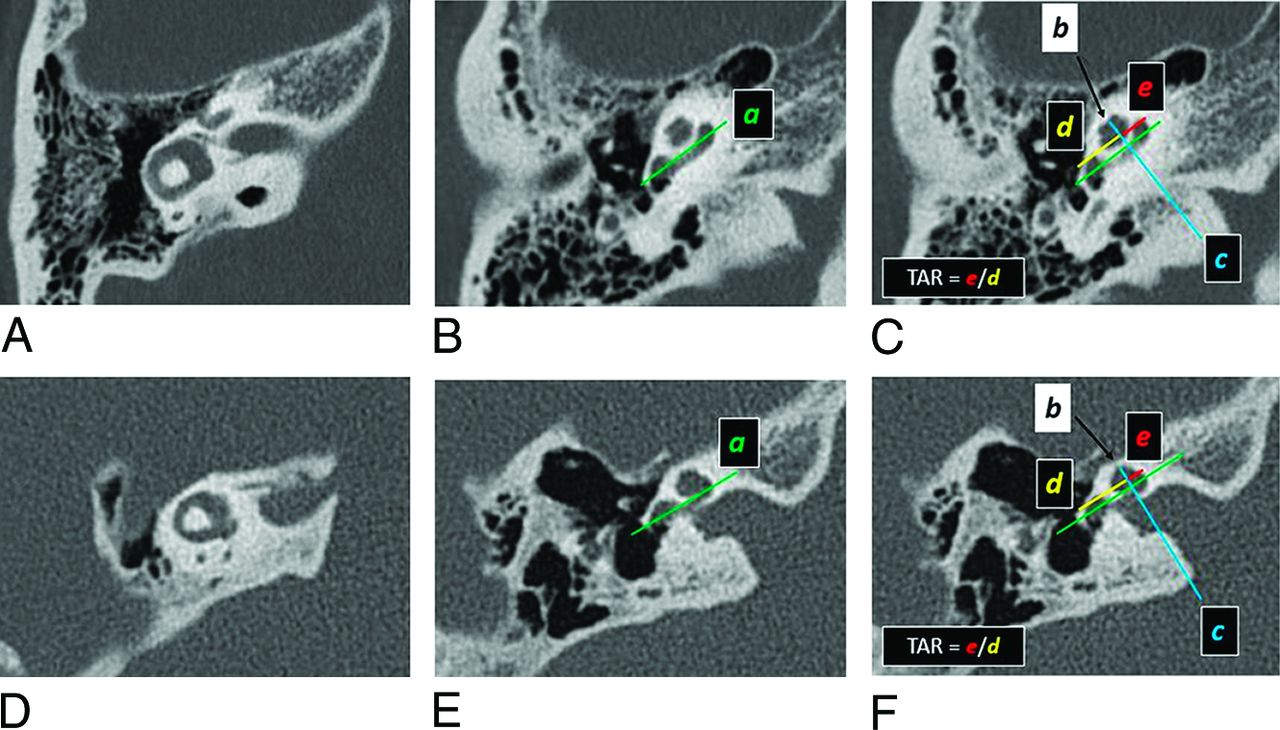
For each ear, the TAR of the cochlea was assessed quantitatively on standardized reformatted axial images in the plane of the lateral semicircular canal, with the following methodology (Fig 1):
A line was drawn parallel to the long axis of the basal turn, extending from the round window to the medial bend (line a).
The midpoint of the last complete uppermost turn/apex was identified (point b).
A perpendicular line was drawn from point b to intersect line a at a right angle (line c), using the “angle” function on PACS to ensure that the angle of intersection measured 90°.
The distance from the anterior border of the round window to the point of intersection was recorded (distance d).
The distance from the point of intersection to the medial bend of the basal turn was recorded (distance e).
TAR is defined was e/d.

Assessment of TAR of the cochlea on a patient without BOR (A–C) and a patient with EYA1-BOR (D–F). Standardized reformatted axial images are utilized, in which the planes are parallel to the plane of the lateral semicircular canal (A and D). Line a (green) is drawn parallel to the long axis of the basal turn (B and E), which is propagated across all axial images, including those where the apical or uppermost developed turn is visible (C and F). The midpoint of the uppermost turn is identified on the image that best displays it (black arrows in C and F); this point (point b) can also be propagated across all axial images. Line c (blue) is then drawn through point b (black arrow), perpendicular to line a (green). Distance d (between the anterior round window and the point of intersection, in yellow) and distance e (between medial bend of basal turn and the point of intersection, in red) are measured. TAR is e/d. As can be seen on these images, TAR in the patient with EYA1-BOR (F) is smaller than in the patient without BOR (C).
These lines and points were usually not all appreciated on 1 single axial plane; thus, care was taken to scroll through consecutive images while keeping the electronic caliper fixed at 1 point from the initial index image before reaching the end point on another image, or lines were propagated across images with identical orientation. When there was need for confirmation, minimum-intensity projections were made to view structures in a stack.
To accurately and reproducibly quantify the cochlear offset, we carefully determined cochlear turns by considering the cochlea in fifths as mentioned by Fitch et al8 and Chen et al.9 The basal turn constitutes the first and second fifths (from the round window to the medial bend, then the medial bend back to the lateral edge), the middle turn constitutes the third and fourth fifths (from the lateral edge to the medial bend, then the medial bend back to the lateral edge), and the apical turn is the last fifth (from the lateral edge at the end of the middle turn going medially toward the end of the tip) (Fig 2). The very short segment of the cochlea that is relatively linear, extending from the round window to the point when the cochlea begins to coil, has been referred to as the “hook region” of the cochlea.10,11 For this study, we followed the methodology of a previously published article,5 in which the hook region of the cochlea is grouped with the spiraling main portion of the basal turn to be collectively considered as the first fifth, ensuring a standardized lateral boundary of the basal turn at the round window membrane and thus ensuring measurement consistency.

A, Fifths of a cochlea, as demonstrated on a 3D reconstruction of the inner ear from a heavily T2-weighted sequence (3D DRIVE). The first fifth is in red (including the hook region), the second fifth in orange, the third fifth in blue, the fourth fifth in green, and the fifth fifth in black. (B, C, and D). CT of the temporal bone in a bone algorithm in the Stenvers view (B) and axial (C and D) planes shows the fifths of the cochlea in the same color scheme as depicted on the 3D model in A.
Statistical Analysis
On the basis of qualitative assessment, the cochleae of all enrolled individuals were divided into 2 groups: with offset and without offset. The number of individuals with EYA1-BOR, SIX1-BOR and unknown-mutation BOR and healthy controls (non-BOR and without hearing loss) in each group was noted.
On the basis of quantitative assessment that yielded TAR numeric values, interrater reliability was evaluated by the intraclass correlation coefficient. Due to excellent agreement, the average of the 2 readers was used for further analysis.12,13
Continuous parametric variables are presented as mean (SD), whereas categoric data are presented as number and percentage. Normal distribution was determined using the Shapiro-Wilk test (P > .05) and histogram plots. A Student t test was performed to explore whether the offset ratio was different between cochleae qualitatively deemed to be with and without offset. Receiver operating characteristic (ROC) curve analysis was used to determine the diagnostic accuracy of the offset ratio. The optimal cutoff point was determined by the Youden index J. P values < .05 were considered statistically significant.
SPSS Statistics 22 software (IBM) was used to perform the analyses. GraphPad Prism 7 (GraphPad Software) was used for graphing.
RESULTS
Eighty participants with a total of 160 cochleae were included in this study: 16 participants (32 cochleae) with EYA1 mutations, 4 (8 cochleae) with SIX1 mutations, 20 (40 cochleae) with BOR of unknown genotype, and 40 (80 cochleae) controls (Table 1).
Qualitative (columns 3 and 4) and quantitative assessment (TAR, column 5) of cochlear offset
There was excellent interrater reliability in the TAR measurements obtained by the 2 independent reviewers, with an intraclass correlation coefficient of 0.976. The values within each of the 2 groups (offset and not offset) followed normal distributions.
The cochleae deemed “not offset” by visual assessment had TAR values ranging from 0.492 to 0.741; the cochleae deemed “offset” by visual assessment had TAR values ranging from 0.189 to 0.460 with 1 outlier at 0.556 (Fig 3). The mean TAR value was significantly lower in cochleae with offset (0.338 [SD, 0.063]) compared with those without offset (0.599 [SD, 0.050]) (P < .001).

Cochlear TAR among cochleae-deemed offset and not offset on visual assessment. EYA1-BOR: black round dots; SIX1-BOR: black square dots; unknown genotype: gray rhomboid dots; controls: gray triangle dots. The dashed line indicates the TAR cutoff (0.476) as determined by ROC curve analysis.
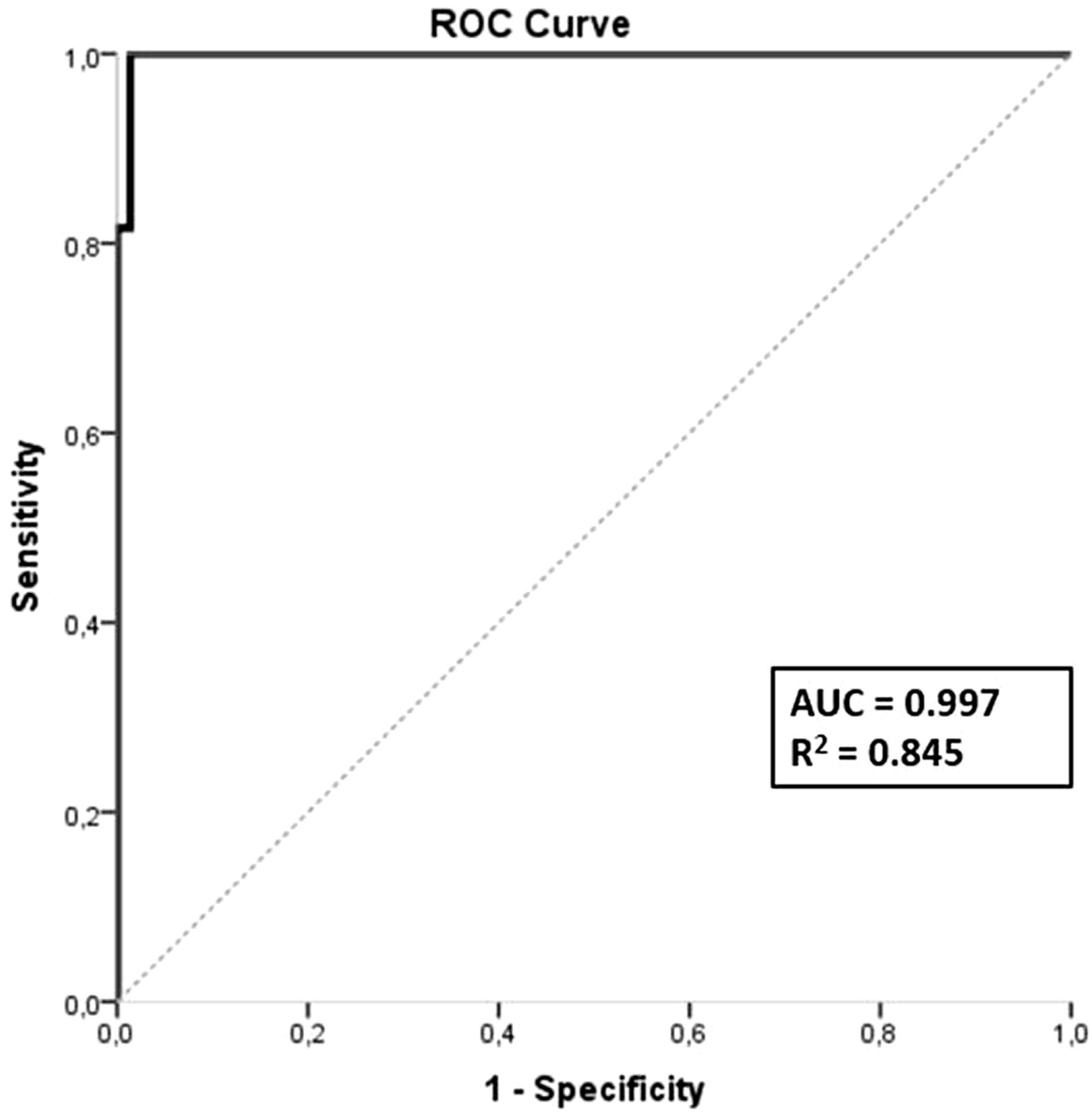
ROC curve analysis showed that TAR can accurately distinguish between cochleae with anterior offset and those without, with an area under the curve (AUC) value of 0.997 (95% CI, 0.992–1) (P < .001) (Fig 4). Based on Youden index J, the optimal cutoff value was 0.476 (sensitivity = 1, specificity = 0.986, J = 0.986). TAR values above the cutoff were predictive of a lack of cochlear offset, whereas values below 0.476 were associated with cochlear offset.

ROC curve.
Seventy-three cochleae showed anterior offset. Of these, 32 were among patients with EYA1-BOR, 1 was among patients with SIX1-BOR, and 40 were among patients with BOR of unknown genotype. Eighty-seven cochleae showed no offset. Of these, 7 were among patients with SIX1-BOR, and the remaining 80 were controls. Of note, all 80 controls showed no offset.
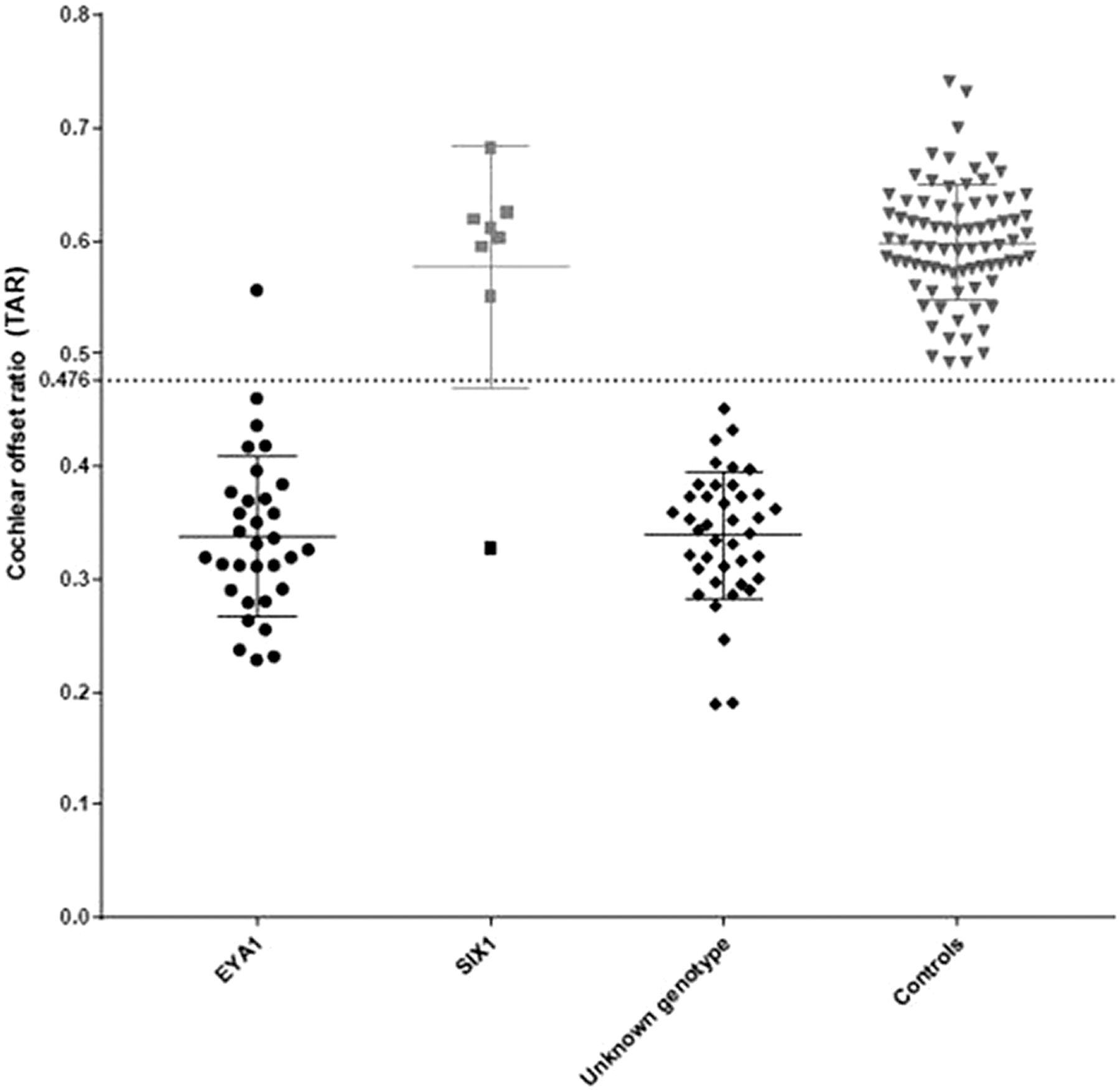
The mean TAR among patients with SIX1-BOR (0.577 [SD, 0.107]) was similar to that among controls (0.598 [SD, 0.051]), with none <0.476. The mean TAR among patients with EYA1-BOR (0.338 [SD, 0.071]) was much lower. The mean TAR among patients with BOR of unknown genotype (0.339 [SD, 0.057]) was similar to that among patients with EYA1-BOR, and all were <0.476. These are listed in Table 1 and depicted in Fig 5.

Cochlear TAR among individuals with EYA1-BOR, SIX1-BOR, BOR of unknown genotype, and controls without BOR or sensorineural hearing loss. The TAR cutoff of 0.476 was determined by ROC curve analysis. All except one of the EYA1-BOR cochleae have TAR below the cutoff value. All except one of the SIX1-BOR cochleae have TAR above the cutoff value. All individuals with BOR of unknown genotype have TAR below the cutoff value. None of the controls have TAR below the cutoff value.
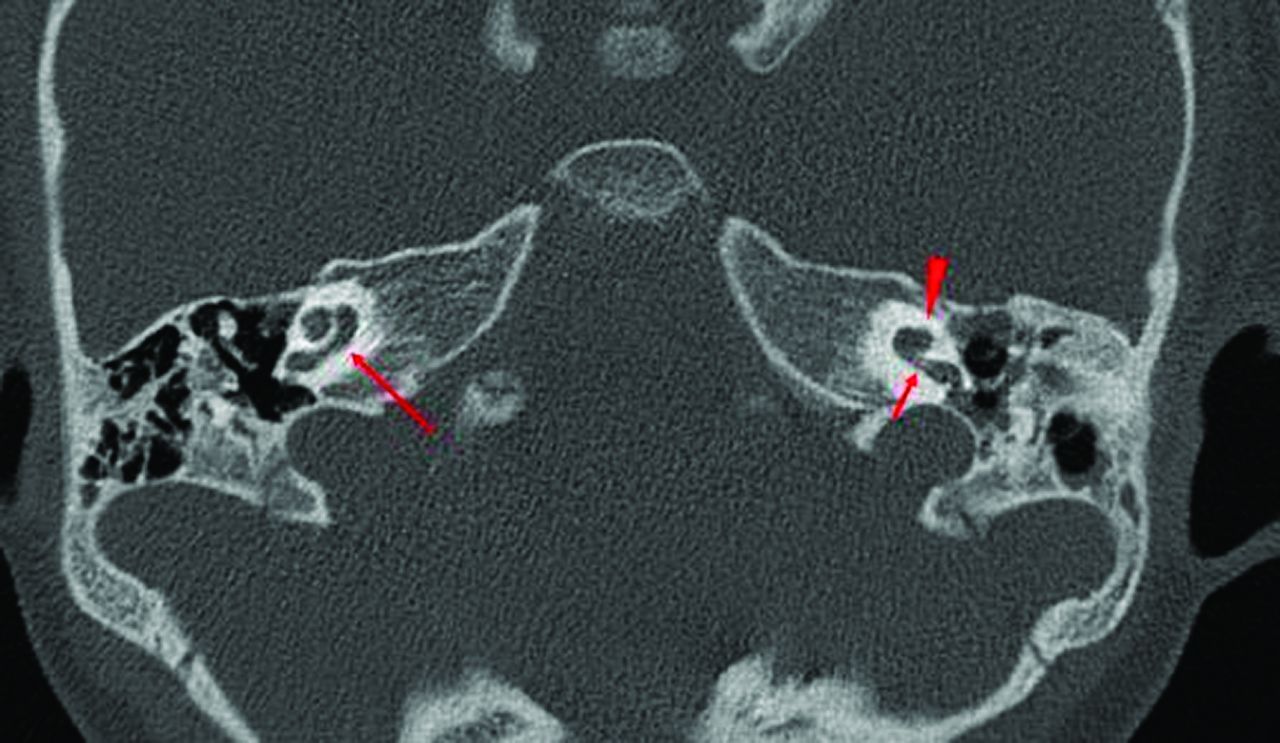
On qualitative assessment, all individuals with EYA1-BOR (32 cochleae of a total of 32) and BOR of unknown genotype (40 cochleae of a total of 40) had bilateral offset cochleae (Fig 6). None had a thorny apical turn (Table 2). On the contrary, cochlear offset was not seen in individuals with SIX1-BOR except in 1 cochlea; that cochlea appeared different from the typical unwound, offset cochlea but instead fit the description of cochlear hypoplasia type 4 (Fig 7)14,15 and lacked a thorny apical turn. The remainder of the SIX1-BOR cochleae had thorny tips (7 cochleae of 8). None of the controls had cochlear offset or a thorny apical turn.

Axial CT images of 3 different patients with EYA1-BOR showing the anteriorly offset unwound cochlea, an imaging feature characteristic of EYA1-BOR. Notice that the middle and apical turns are anteriorly located relative to the basal turn (red arrows) and slightly tilted away and separated from the basal turn (yellow arrowheads).
The presence/absence of thorny tips among the 3 BOR populations and in controls

CT image of the patient with SIX1-BOR in whom the right cochlea does not demonstrate any offset (long arrow), while the left cochlea has an offset but with an appearance akin to cochlear hypoplasia type 4 rather than the typical unwound and offset cochlea of EYA1-BOR. Notice the normal size and morphology of the basal turn first half (short arrow), while the distal basal, middle, and apical turns are hypoplastic (arrowhead).
DISCUSSION
The presence of a cochlear offset associated with EYA1-BOR has traditionally been determined qualitatively, whereby the radiologist visually estimates whether the alignment of the cochlear turns appears to be anomalous, with the upper turns anteriorly displaced and slightly tipped away relative to the basilar turn, outside the range of normal. However, this estimation may be challenging for radiologists who do not routinely interpret temporal bone imaging studies. In this study, we explored an objective method to evaluate and quantify the presence of an anteriorly offset or unwound cochlea in patients with EYA1-BOR, to provide a reproducible and reliable diagnostic tool for all radiologists.
All of our patients with a clinical diagnosis of BOR and confirmed EYA1 mutations (16 patients, 32 cochleae) had anteriorly offset cochleae on subjective visual analysis. We found that there was a statistically significant difference in TAR between individuals with EYA1-BOR and controls without a diagnosis of BOR or sensorineural hearing loss. The optimal cutoff value for the upper limit of TAR that produced the greatest sensitivity and specificity for the detection of cochlear offset suggestive of EYA1-BOR was 0.476. This implies that this TAR measurement method and cutoff value can be used to suggest EYA1 mutations in patients with a clinical diagnosis of BOR.
Furthermore, except for 1 outlier, all cochleae among the patients with SIX1-BOR in our cohort did not have anterior offset, with a TAR of >0.476. In the 1 outlier that did demonstrate misaligned cochlear turns, it appeared to be due to an underlying cochlear hypoplasia (type 4) (Figs 7), distinct in morphology from the typical EYA1-BOR offset cochlea (Fig 1E, -F). Thus, there is a good degree of quantitative difference in cochlear turn alignment between individuals with EYA1-BOR and those with SIX1-BOR. This is in addition to morphologic differences in the apical turn of the cochlea previously demonstrated, whereby the EYA1-BOR cochlea appears unwound with an anterior offset, while the SIX1-BOR cochlea has a thorny apical turn without the characteristic anterior offset (Fig 8).5

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
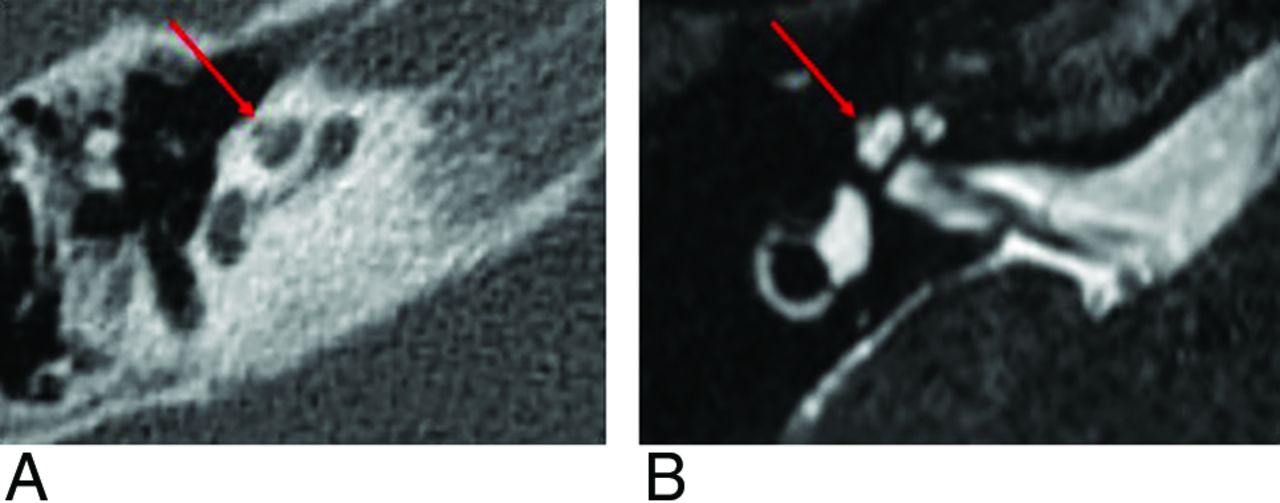
A thorny apical turn in a patient with SIX1-BOR. The apical turn of the cochlea appears as a short, protuberant, thorny tip, as seen on CT (A) and MR imaging (B).
Notably, in our cohort, all the individuals with BOR of an unknown underlying causative genotype had offset cochleae, with a TAR of <0.476. In addition, they did not have thorny apical turns. On the basis of the strong phenotype-genotype correlation in patients with BOR and our current results, we speculate that all the patients with BOR in our cohort of an unknown genetic diagnosis may have EYA1 mutations, given their anteriorly offset cochleae and lack of a thorny apical turn. This finding would be in keeping with the estimated substantially higher prevalence of EYA1 compared with SIX1 mutations among patients with BOR reported in the literature.16-19
Interestingly, all our patients with EYA1-BOR (TAR < 0.476) had moderate-to-severe conductive hearing loss and mild-to-moderate sensorineural hearing loss. All our patients with SIX1-BOR without obvious cochlear dysmorphology (TAR > 0.476) had mild conductive hearing loss (35–40 dB) and mild sensorineural hearing loss (25–35 dB). The 1 patient with SIX1-BOR with a hypoplastic cochlea had severe conductive hearing loss and profound sensorineural hearing loss. All except one of the patients with BOR of unknown genotype had moderate-to-severe conductive hearing loss and mild-to-moderate sensorineural hearing loss, showing that most of them had hearing ability similar to that of those with the EYA1 mutation rather than the SIX1 mutation; this finding would be in keeping with the known estimated prevalence of these 2 genotypes among the overall BOR population.
The interactions between SIX1 and EYA1 protein expression during cochlear development are complex; however, we know from murine models that while SIX1 expression is dependent on EYA1, EYA1 expression is not impacted by SIX1. Moreover, SIX1 is mainly expressed in the apical part of the cochlea.20 This location may explain the milder alteration in cochlear phenotype associated with SIX1 mutations compared with EYA1 mutations. It is unclear why one of our patients with a SIX1 mutation had the characteristic thorny cochlea on only 1 side and an anterior offset and hypoplastic cochlea on the other; it is possible that this feature is due to the particular locus of the mutated base pairs in the gene leading to different resultant disturbances in the complex SIX1/EYA1 interactions.21 Furthermore, the SIX1 variant in this case (Cys16Tyr) is located closer toward the N-terminal (SD domain) within an α-helix critical for EYA interaction. More studies with larger cohorts of patients with SIX1-mutated BOR would be helpful to clarify whether specific mutations within the same gene can create varying and potentially characteristic phenotypes.
As expected, none of the control patients had anteriorly offset cochleae, corroborating the high sensitivity of this radiologic sign. However, there are other genetic causes of malformed cochleae with hypoplastic middle and apical turns reported in literature, such as Walker-Warburg syndrome, where the “hook” of the basal turn is the only well-preserved portion of the cochlea and the upper parts are anteriorly placed and markedly hypoplastic, resembling an extreme anteriorly offset cochlea.22 This appearance may relate to an arrest in embryonic development before the end of the seventh week of gestation, when only the first half of the basal turn is formed and the second half of the basal turn and the middle/upper turns have yet to develop and fold on themselves to create the final cochlear structure. To the best of our knowledge, at the current time, the anterior offset unwound cochlea fitting the original radiologic description3,5 has been described only in EYA1-BOR and Walker-Warburg syndrome. However, as knowledge in genetics increases with time, it might be discovered that this offset appearance of the cochlea may be a part of the phenotypic constellation in other, rare causes and genotypes related to cochlear dysplasia.23
Some limitations of this study are its retrospective design, different CT and MR imaging protocols among the participating institutions, and its relatively small sample size. In the future, we would benefit by prospective enrollment of patients with BOR to achieve a larger population size, preferably with known underlying genotypes, and to perform qualitative and quantitative TAR assessment in a large BOR population.
CONCLUSIONS
This study shows that there is a statistically significant difference in TAR between offset and nonoffset cochleae, with an optimal cutoff at 0.476. This is also the optimal TAR threshold value that allows excellent separation of the EYA1-BOR population from the SIX1-BOR population, and separation of patients with EYA1-BOR from individuals without sensorineural hearing loss. The proposed TAR measurement method and threshold value can aid any radiologist in the determination of “how offset is too offset”, to decide objectively whether there are anomalous offset cochleae compatible with the EYA1-BOR genotype-phenotype.
Footnotes
A.F. Juliano and F. D’Arco are co-first authors.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- Received May 2, 2022.
- Accepted after revision August 19, 2022.
- © 2022 by American Journal of Neuroradiology