Abstract
SUMMARY: Hypoxic-ischemic injury is the most common cause of neonatal encephalopathy. T1-weighted punctate white matter lesions have been described in hypoxic-ischemic injury. We have reviewed a healthy volunteer neonatal population to assess the prevalence of punctate white matter lesions in neonates with no clinical signs of hypoxic-ischemic injury. Fifty-two subjects were scanned on a neonatal-specific 3T MR imaging scanner. Twelve patients were excluded due to the lack of T1-weighted imaging, leaving a total of 40 patients (35 term, 5 preterm) assessed in the study. One had a solitary T1-punctate white matter lesion. We concluded that solitary punctate white matter lesions have a low prevalence in healthy neonates.
ABBREVIATIONS:
- HII
- hypoxic-ischemic injury
- PWML
- punctate white matter lesion
- SDH
- subdural hematoma
Neonatal hypoxic-ischemic injury (HII) is the most common cause of neonatal encephalopathy, ahead of infection, metabolic disorder, and trauma.1,2 HII can occur in preterm or term infants.1 On MR imaging, HII with brain injury can manifest as signal abnormality within the posterior putamen, ventral-posterolateral thalamic injury, central sulcus cortical injury (acute profound asphyxia), or watershed injury (chronic partial asphyxia).3 Punctate white matter lesions (PWMLs) are hyperintense on T1-weighted and iso- to hypointense on T2-weighted imaging. PWMLs have been described in association with hypoxic-ischemic injury.4 PWMLs can be multifactorial, with a combination of gliotic scarring, hemorrhage, and mineralization contributing to their MR imaging appearance; however, it is often not possible to ascertain which of these is the causative factor in each case. A histologic study has, however, found that approximately 25% of PWMLs are secondary to hemorrhage.5
SWI may help differentiate hemorrhagic PWMLs from nonhemorrhagic PWMLs, with the latter attributed to early scarring or mineralization.6 Hemorrhagic PWMLs are also associated with greater proportions of infantile intraventricular hemorrhage, with nonhemorrhagic PWMLs being associated more with ischemia-related injury.7 In either etiology, the general consensus is that PWMLs are derived from pathologic processes occurring via hemorrhagic or ischemic pathways. Thus, these lesions, one would assume, should not be present in a healthy neonate who has not been subjected to any known pathologic insult.
In our study, we reviewed MR images of a healthy volunteer neonate population obtained on a specific neonatal MR imaging scanner to assess the prevalence of PWMLs in neonates without clinical signs of HII.
MATERIALS AND METHODS
A 3T neonatal MR imaging scanner (GE Healthcare) was installed in the neonatal unit of the local obstetric department.
Ethics approval was governed by the Medicines and Healthcare products Regulatory Agency of the UK. Conditions of use granted under the Medicines and Healthcare products Regulatory Agency were that the scanner was not to be used for primary diagnostic purpose and the manufacturer sponsored the study. Enrollment for up to 60 neonatal subjects was granted. Two groups were scanned. Group 1 consisted of healthy term neonates (≥37 weeks’ gestational age) whose parents agreed to MR imaging before discharge. Group 2 involved premature neonates about to be discharged at term-corrected age, with no other clinical complications.
All subjects had 2 scheduled sonography examinations throughout pregnancy as per local guidelines, at approximately 12 and 19 weeks for the first and second scans, respectively. No subjects were found to have screening anomalies on fetal sonography.
All parents provided informed, written consent and completed an MR imaging safety form for the neonate and themselves because 1 parent could accompany their child during scanning.
Healthy volunteer subjects were imaged as part of the Firefly 3T MR imaging project evaluation.8 The scans were performed within 1 hour of feeding. The 3T magnet strength was deemed safe for neonatal scanning.9 Subjects’ vital observations encompassing body temperature, heart rate, and oxygen saturation were monitored throughout scanning. Scanning time was limited to 1 hour inclusive of the time for room acclimatization, monitoring, and subject positioning.
Initially, T2-weighted images were acquired in a trial format and optimized for contrast, resolution, and scan time before using them for both ultrafast single-shot FSE and T2-FSE imaging. The optimized T2-sequence parameters were subsequently used for all cases with long-TE single-voxel proton spectroscopy, T1-volume/spin-echo, DWI, and MR arteriography added as tolerated.
Inclusion criteria were patients with T2-weighted imaging and either or both standard T1-weighted spin-echo and T1-volumetric sequences. Excluded cases were those without T1-weighted imaging because they were unable to be adequately assessed for PWML.
Acquired images were reviewed by 2 consultant pediatric neuroradiologists. Further reviews were conducted by 2 post-board examination Royal College of Radiologists (FRCR, UK) neuroradiology fellows.
RESULTS
Fifty-two subjects were recruited into the study in total; however, 12 had no T1-weighted imaging; therefore, 40 cases were evaluated for evidence of PWML (35 in group 1, five in group 2).
One subject had a pre-existing bradycardia, and while having a normal sinus rhythm before scanning, the subject developed bradycardia during scanning. This was, however, not deemed to be attributed to MR imaging, and the neonate did not require further follow-up on discharge. No other subject demonstrated abnormal vital signs before, during, or immediately after MR imaging.
One hundred percent of imaging studies (40/40) were deemed evaluable, either completely or partially. Twenty-five percent (10/40) of studies were deemed partially evaluable, predominantly secondary to motion artifacts. The partially evaluable studies were, however, still thought to be accurate enough to identify notable abnormal findings on T1-weighted imaging.
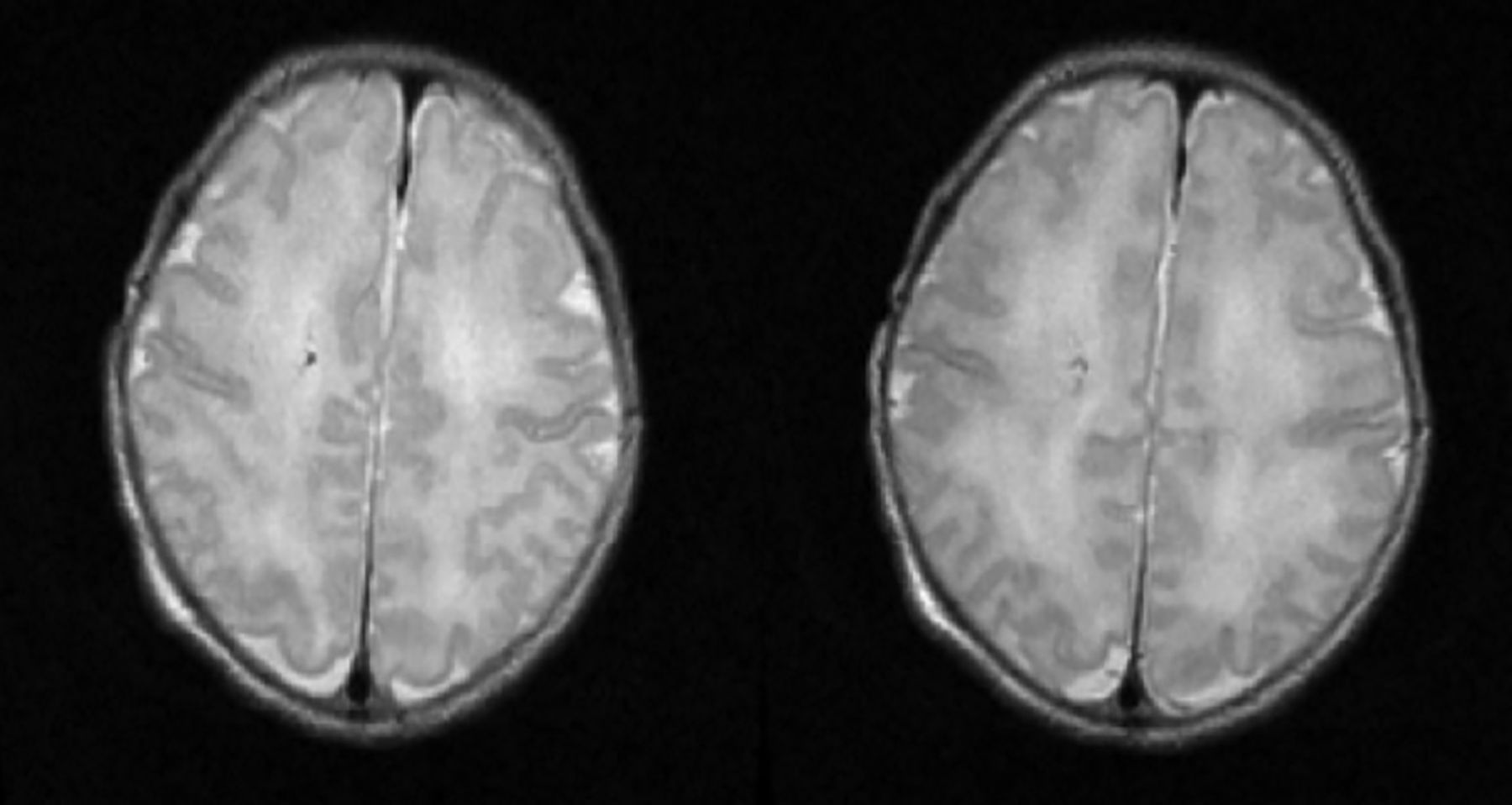
Of the 40 subjects, 1 subject in group 1 (2.5%) had evidence of a 2-mm solitary PWML, which was hyperintense on T1-weighted imaging (Fig 1). It was not possible to further distinguish this PWML as hemorrhagic or nonhemorrhagic (scarring/mineralization) due to absence of SWI. In this case, no pre- or perinatal injury was known to have occurred, nor was there any evidence of neonatal encephalopathy. The finding was, therefore, of unknown etiology but highly unlikely to be from perinatal asphyxia. The long-term follow-up of this PWML is not known.

A solitary T1-weighted PWML was demonstrated in the left corona radiata of 1 study patient (white arrow).
One group 2 subject (2.5%) had a finding of a right frontal developmental venous anomaly (Fig 2) with small-volume intraventricular hemorrhage; however, clinical review was unremarkable, and the subject was developing normally on 2-month assessment.

One subject demonstrated a right frontal developmental venous anomaly.
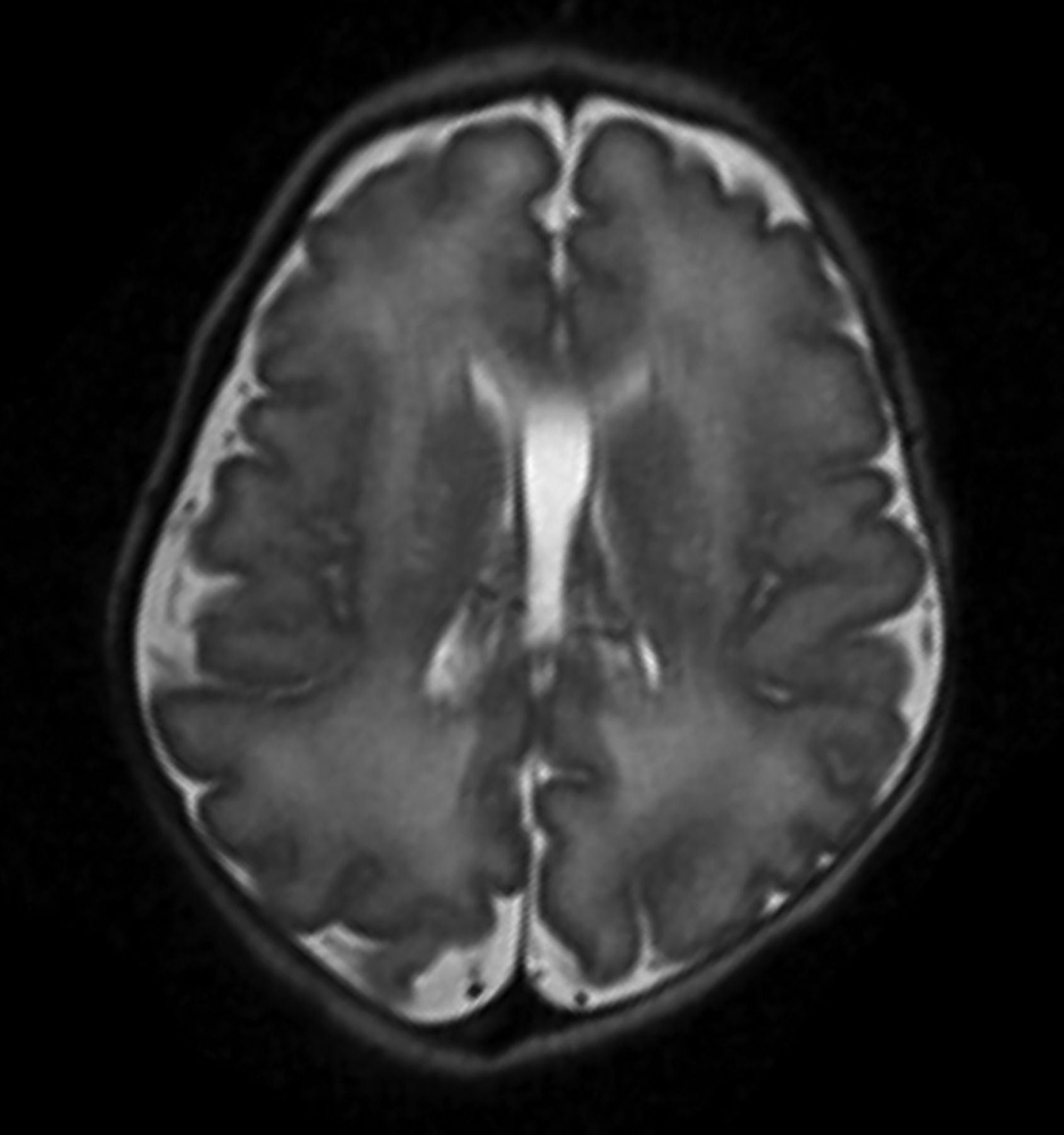
One group 1 subject (2.5%) had a cavum vergae, a normal anatomic variant with no clinical consequences (Fig 3). One group 1 subject (2.5%) also had a maturing left subdural hematoma (SDH) (Fig 4).

An incidental normal variant of a cavum vergae was seen in 1 study subject.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A moderate-sized left-convexity SDH was observed in 1 otherwise clinically well patient on T1-weighted imaging. This can be a common finding postbirth, seen in up to 38% of the population, spontaneously self-resolving in most cases.
DISCUSSION
In our population, there was an overwhelmingly large proportion of subjects presenting with no evidence of PWMLs (97.5%). In the single patient presenting with a tiny, solitary PWML, no discernible signs of physiologic impairment were seen on early medical assessment of the infant. Recent studies performed at approximately 18 months postpartum have demonstrated a similar, albeit slightly higher incidence of incidental PWMLs at approximately 12%; however, this is still consistent with a substantial minority within the population.10 The slightly higher incidence in a delayed-scan cohort could potentially be secondary to a greater number of lesions being visible from gliosis or scarring, which may not necessarily have been immediately visible in our postpartum scan cohort; however, with time, these lesions may become more apparent.
The same proportion of subjects that presented with a PWML also presented with an incidental normal variant (cavum vergae) and a left-sided SDH. SDH is a common finding, seen in up to 38% of births.11
A limitation of our study was that some studies were affected by motion artifacts; therefore, not all studies were of an equivalent reading standard. Nevertheless, all studies were deemed by participating radiologists to be of sufficient quality to provide conclusive PWML identification/exclusion. Furthermore, there was a significant difference in subject numbers within the 2 groups (35 versus 5); and while the overall number of 40 subjects is low, given the limitations of the population, this is the largest cohort of healthy neonates in the literature to be scanned postpartum for PWMLs.
Our findings conclude that PWMLs have very low prevalence in healthy neonates, and the presence of 1 or 2 PWMLs in otherwise healthy patients is not likely to be of clinical relevance. Furthermore, PWMLs in these cases may not necessarily be secondary to hemorrhage or scarring, but from physiologic mineralization. In contrast, when several T1 PWMLs (approximating ≥6) are present, this is more likely related to perinatal asphyxia, and closer follow-up is recommended.3
CONCLUSIONS
We recommend that in the event of neonates demonstrating 1 or 2 PWMLs with no other clinical or radiologic abnormality, no routine follow-up imaging is indicated. Further long-term follow-up studies to investigate the chronic relevance of solitary PWMLs in otherwise healthy neonates are required.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- Received March 17, 2022.
- Accepted after revision May 24, 2022.
- © 2022 by American Journal of Neuroradiology