Abstract
SUMMARY: Photon-counting CT is an increasingly used technology with numerous advantages over conventional energy-integrating detector CT. These include superior spatial resolution, high temporal resolution, and inherent spectral imaging capabilities. Recently, photon-counting CT myelography was described as an effective technique for the detection of CSF-venous fistulas, a common cause of spontaneous intracranial hypotension. It is likely that photon-counting CT myelography will also have advantages for the localization of dural tears, a separate type of spontaneous spinal CSF leak that requires different myelographic techniques for accurate localization. To our knowledge, prior studies on photon-counting CT myelography have been limited to techniques for detecting CSF-venous fistulas. In this technical report, we describe our technique and early experience with photon-counting CT myelography for the localization of dural tears.
ABBREVIATIONS:
- CTM
- CT myelography
- DSM
- digital subtraction myelography
- EID
- energy-integrating detector
- PCCT
- photon-counting CT
- PC-CTM
- photon-counting CT myelography
- SIH
- spontaneous intracranial hypotension
- SR
- standard resolution
- UHR
- ultra-high-resolution
- VMI
- virtual monoenergetic image
Spontaneous intracranial hypotension (SIH) is caused by a spinal CSF leak, which, in turn, may be secondary to a dural tear (type 1), a leaking meningeal diverticulum (type 2), or a CSF-venous fistula (type 3).1 Clinical manifestations of SIH are frequently debilitating and occasionally life-threatening. SIH is often reversible when treated, but this procedure requires identification of the site and type of CSF leak present. Brain MR imaging is an effective means of corroborating a diagnosis of SIH but findings can be normal in a subset of patients.2 Spine MR imaging and/or conventional CT myelography is helpful to determine the type of CSF leak present; those with dural tears almost universally have extradural CSF, while those with leaking diverticula or CSF-venous fistulas are typically negative for extradural CSF collections.3 After these initial tests, advanced myelography is almost always needed to precisely localize a spinal CSF leak.
Recently, decubitus myelography using photon-counting CT (PCCT) was described as an effective technique for the detection of CSF-venous fistulas.4 PCCT uses a different type of x-ray detector than traditional energy-integrating detector (EID) CT. The detector used in PCCT permits direct conversion of x-rays into an electrical pulse with energy proportional to the incident photon. In contrast, EID CT detectors require a 2-step conversion process that results in summation of photon energies and loss of individual photon energy information. Furthermore, PCCT detectors do not require septa between detector elements, reducing limitations on spatial resolution.4 PCCT myelography (PC-CTM) was shown to identify CSF-venous fistulas that were missed on decubitus digital subtraction myelography (DSM) and decubitus EID CT myelography (EID CTM). This finding was largely related to several technologic advantages conferred by PCCT, including improved spatial resolution, higher temporal resolution, and inherent spectral sensitivity, all of which can be useful to detect subtle CSF leaks.5 PCCT has also been shown to confer dose reduction compared with EID CT in spine imaging, with 1 study showing a >50% dose reduction in CT of the lumbar spine.6
To our knowledge, PC-CTM has not been previously used for the localization of dural tears. Although dural tears are not typically as elusive on imaging as CSF-venous fistulas, they can, nonetheless, be challenging to precisely localize. PC-CTM likely provides advantages compared with typical techniques currently used such as DSM and dynamic EID CTM. Here, we describe a technique for dynamic PC-CTM used to localize dural tears in patients with SIH with spine MR imaging demonstrating extradural CSF collections.
TECHNICAL REPORT
Previous Myelographic Techniques
In recent years, the 2 main techniques used for localization of dural tears have included DSM and dynamic EID CTM.7 These procedures are performed with the patient positioned prone when a ventral dural tear is suspected and decubitus when a lateral dural tear is anticipated.8 DSM provides higher spatial and temporal resolution and typically has a lower radiation dose compared with dynamic CTM on EID scanners.9 By contrast, the main advantage of dynamic EID CTM is that it provides cross-sectional detail, which often allows one to determine not only the level but also the precise laterality of a dural tear (for example, left/right ventrolateral versus midline ventral). Furthermore, dynamic CTM can reveal osseous spicules or osteophytes that frequently cause ventral dural leaks, while such lesions are usually occult on DSM.10 Dynamic CTM was initially described in 2003 by Luetmer and Mokri.11 Since that time, the technique has been improved with newer-generation CT technology.12⇓-14 To date, all described techniques for dynamic CTM have used EID CT scanners, most recently including modern dual-energy CT scanners with fast scan speeds.12,13 PCCT represents a fundamental shift in CT technology, using a novel detector mechanism that permits a wide variety of the aforementioned improvements.
Dynamic PC-CTM Technique
In our practice, all patients with suspected SIH undergo noncontrast MR imaging of the entire spine. If this demonstrates extradural CSF, a dural tear is assumed to be present.15 If the extradural CSF collection is largely ventral, a ventral dural tear is suspected. If the extradural collection is predominantly dorsolateral or if there is a large or irregular meningeal diverticulum, greater consideration is given to the possibility of a lateral leak site. On the basis of these factors, prone-versus-decubitus positioning for subsequent myelography is chosen. The decision among DSM, dynamic EID CTM, and dynamic PC-CTM is currently based on the radiologist’s preference and/or equipment availability.
For dynamic PC-CTM, patients are placed prone or decubitus on the PCCT scanner table (NAEOTOM Alpha; Siemens), using a custom cushion to elevate the pelvis. Lumbar puncture is performed under CT guidance at L2–L3 or below using a 22-ga Quincke spinal needle. Intrathecal needle positioning is confirmed with a tiny (∼0.2 mL) injection of Omnipaque 300 (GE Healthcare). A low-dose monitoring scan is set up approximately 2 spinal levels below the lowest level at which extradural CSF is present. Next, 2 mL of contrast is injected while the monitoring scan is continuously repeated every 5 seconds. As soon as intrathecal contrast is visible on the monitoring scan, 2–4 scans of the spine are initiated, with the exact number of scans depending on patient-specific factors (for example, more scans may be obtained if the patient has undergone previously unrevealing myelograms). The scan range may be limited to the spinal levels at which extradural CSF is present or may include the entire spine, largely depending on proceduralist’s preference. An additional 1–2 mL of contrast is injected immediately before every scan. The scans are obtained as quickly as allowed by the scanner, with usually only 2–3 seconds of delay between scans.
Each scan is obtained in standard resolution mode (SR, 144 × 0.4 mm detector collimation), except for the final scan, which is obtained in the ultra-high-resolution mode (UHR, 120 × 0.2 mm detector collimation). The SR mode provides greater temporal resolution due to a shorter scan time, though the resulting section thickness is limited to 0.4 mm. The UHR mode usually has approximately double the scan time but can provide a section thickness as low as 0.2 mm. The rationale for performing a UHR scan at only the final acquisition is to provide at least 1 high-resolution scan without impairing the temporal resolution during the most time-sensitive portion of the examination. Both scan modes confer spectral sensitivity even when a single x-ray source is used, meaning that images can be reconstructed at any desired virtual monoenergetic level. All scans use a rotation time of 0.5 seconds and a CARE keV IQ level of 200. The pitch is 1.2 (SR) or 1.0 (UHR). Automatic exposure control is used, with a manual tube potential of 140 kV.
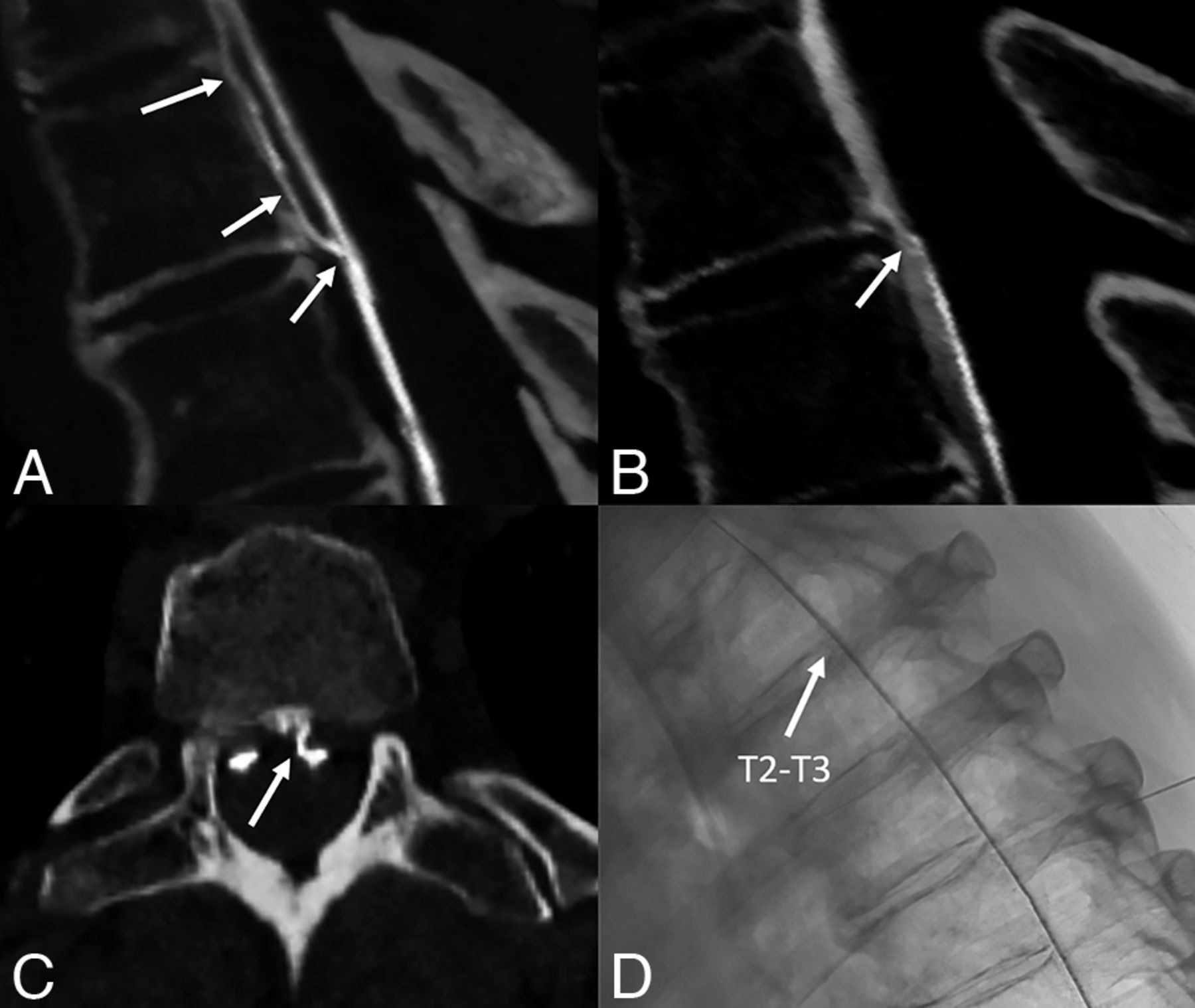
In our protocol, all scans are reconstructed with the lowest section thickness allowed by the scan mode (0.4 mm for SR and 0.2 mm for UHR). A low-energy threshold (referred to as T3D by the manufacturer and including all photon energies from 25 to 140 keV) is applied to all series. Separately, we reconstruct 40-keV virtual monoenergetic images (VMIs) to maximize iodine conspicuity (thus, 2 series are created for each scan performed). We use a Br48 kernel (quantum iterative reconstruction setting of 3) for the 40-keV VMIs and a Br56 kernel (quantum iterative reconstruction setting of 4) for T3D reconstructions. These are both relatively sharp kernels that provide high spatial resolution while maintaining an acceptable noise level. As with previously described techniques, the site of the dural tear is determined by direct visualization of a contrast column leaking into the epidural space (Fig 1). The approximate leak site can also be inferred by the lowest spinal level at which epidural contrast is seen, though this is a less definitive finding, and direct visualization of the exact level is strongly preferred.

Ventral dural tear localized on PC-CTM after negative prone DSM and negative prone dynamic EID CTM. Sagittal low-energy threshold (T3D) reconstructions from the first scan during dynamic PC-CTM demonstrate a ventral leak at T2–T3 (A, arrow). The leak remained visible on the second scan obtained 4 seconds later (not shown) but was barely visible on the third scan obtained after another 4 seconds (B, arrow), largely because of dense contrast that had already leaked into the epidural space. An axial 0.4-mm image from the first scan (C) clearly shows the precise site of the dural tear, which is slightly to the left of midline (C, arrow). This leak was occult on prone DSM (unsubtracted image D, arrow), as well as on prone dynamic EID CTM (not shown), both of which were performed before the PC-CTM.
DISCUSSION
We have described a technique for dynamic PC-CTM that can be used for the precise localization of dural tears. Fundamentally, this technique is similar to those previously described for EID CT. However, there are several nuances unique to PCCT, and radiologists considering PC-CTM for this purpose should become familiar with the different scan modes, reconstructions, and benefits of PCCT.
Our early experience has demonstrated several advantages of dynamic PC-CTM specific to the localization of dural leaks. First, the high temporal resolution conferred by the SR scan mode allows rapid imaging of the spine as the intrathecal contrast bolus ascends. This is crucial because dural tears usually result in fast CSF leaks, and high temporal resolution maximizes the chance of observing the precise location where contrast leaks into the epidural space (Fig 1). The difference in temporal resolution between dynamic PC-CTM and dynamic EID CTM varies depending on the specific EID scanner used. We have observed that both the time between scans and the time per scan are approximately 50% longer on dynamic EID CT performed on our dual-energy scanner (Definition Flash; Siemens) compared with PCCT. Second, PC-CTM offers very high spatial resolution. This has a variety of benefits for localization of dural tears, including more precise anatomic discrimination of the leak site, greater confidence in localization of subtle leaks, and exquisite characterization of tiny osseous spicules that often cause these leaks (Figs 1–2).10 Third, PC-CTM has inherent spectral sensitivity, meaning that VMIs can be reconstructed without the need for dual-energy or dual-source techniques. We have found that 40-keV VMIs are useful to increase the conspicuity of subtle CSF leaks (Online Supplemental Data). Although dual-energy CT can provide VMIs as well, they come at the cost of slower scan speeds. Finally, PC-CTM has a lower radiation dose compared with EID CT.6 A reduced-dose EID CT–based technique was recently described by Mamlouk et al,14 and dynamic PC-CTM has the potential to even further reduce the radiation dose to these patients.

{kind=link}
{kind=link}
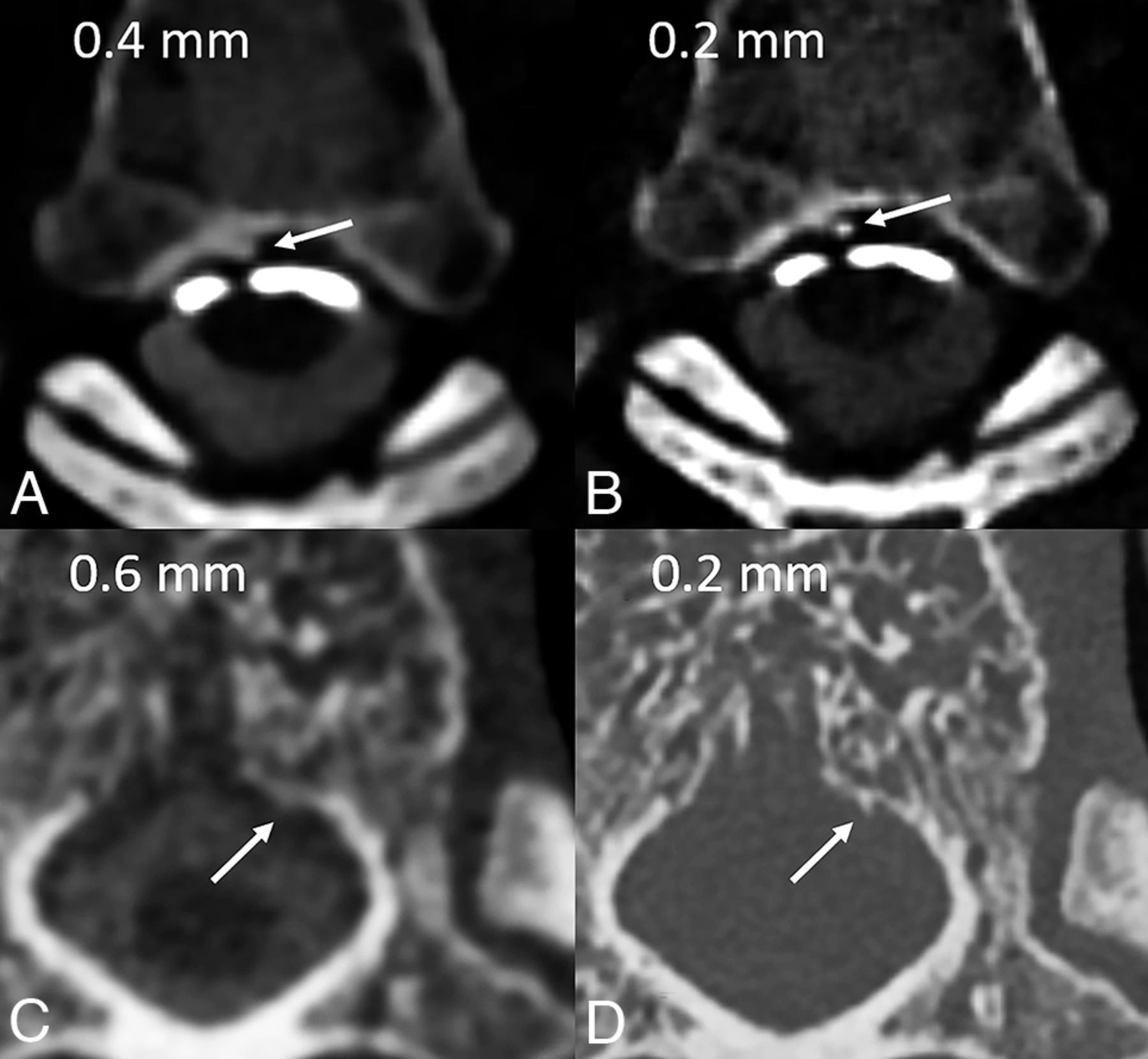
Benefits of high spatial resolution in 2 patients with ventral dural tears. In the first patient (A and B), axial low-energy threshold (T3D) images from a prone dynamic PC-CTM demonstrate a thin column of epidural contrast that had leaked ventrally at T5–T6 (A and B, arrows). The contrast column is more exquisitely delineated from the vertebral body cortex when the same image is reconstructed at 0.2 mm compared with 0.4 mm. In the second patient, a ventral leak at T11 was diagnosed on prone DSM. A postmyelographic EID CT image at 0.6 mm (C) shows a questionable osseous excrescence at the level of the leak (C, arrow) without a definite spicule. Subsequent PCCT image at 0.2 mm (D) shows that this lesion is, in fact, a sharp osseous spicule arising from the vertebral cortex (D, arrow), confirming the presumed cause of the leak, which was later identified and repaired at surgery.
Our technical report has limitations, the most important of which is the small number of patients on which this examination has been performed (n = 6). The site of the dural tear was precisely localized in all 6 of these patients, including 5 ventral leaks and 1 lateral leak. Three patients had previously unrevealing findings on myelograms. Specifically, 1 underwent an initially negative prone DSM, 1 underwent an initially negative dynamic EID CTM, and 1 underwent both an initially negative DSM and negative dynamic EID CTM (Fig 1). For the 2 patients who underwent both a dynamic EID CTM and dynamic PC-CTM, we observed a dose reduction per scan of 20% and 25%, respectively (measured in dose-length product). Future studies on larger patient populations will be needed to determine how frequently PC-CTM adds true diagnostic value and how much dose reduction is typically achieved, but our preliminary experience with this application of PC-CTM has been promising. It will be particularly important to compare DSM, dynamic EID CTM, and dynamic PC-CTM in a randomized fashion, because varying results between modalities could theoretically be due to uncontrolled factors such as spontaneous opening or closure of leaks. Another limitation of this study is that PCCT is not available at all institutions. However, it is likely that this technology will become more prevalent in the near future, underpinning the need for continued investigation of its role in patients with SIH.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- Received December 3, 2023.
- Accepted after revision January 8, 2024.
- © 2024 by American Journal of Neuroradiology