Abstract
BACKGROUND AND PURPOSE: Concentrations of calcitonin gene-related peptide, a neuropeptide and potent endogenous vasodilator, are reportedly higher in patients with migraine than in healthy subjects, both during and between migraine attacks, reflecting ongoing activation of the trigeminal nervous system. In this prospective study, we measured CBF during the interictal period of patients with migraine after considering insomnia and depression and examined the effects of ongoing activation of the trigeminal nervous system, including during the interictal period, on CBF.
MATERIALS AND METHODS: In a total of 242 patient with migraine (age range, 18–75 years), CBF was measured by MR imaging arterial spin-labeling during the interictal period and was compared with results from 26 healthy volunteers younger than 45 years of age as control subjects (age range, 22–45 years). Cortical hyperperfusion was defined as identification of ≥2 cerebral cortical regions with regional CBF values at least 2 SDs above the mean regional CBF in control subjects.
RESULTS: The overall frequency of cortical hyperperfusion was significantly higher in patients with migraine (115 of 242, 48%) than in control subjects (1 of 26, 4%). Multivariable analysis revealed the 18- to 40-year age group and patients with migraine without insomnia as significant positive clinical factors associated with cortical hyperperfusion. Among patients with migraine without insomnia, the frequency of cortical hyperperfusion was >92% (89 of 97). One-way ANOVA showed that in all ROIs of the cortex, regional CBF was significantly higher in patients with migraine without insomnia than in patients with migraine with insomnia or control subjects. In patients with migraine without insomnia, cortical hyperperfusion findings showed a sensitivity of 0.918 and a specificity of 0.962 for migraine in the interictal period, representing excellent accuracy. In contrast, among patients with migraine with insomnia, sensitivity was only 0.179 but specificity was 0.962.
CONCLUSIONS: Patients with migraine without insomnia may have cortical hyperperfusion during the interictal period; however, the findings of the present study need to be prospectively validated on a larger scale before clinical applicability can be considered.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- AIS
- Athens Insomnia Scale
- AI
- asymmetry index
- ASL
- arterial spin-labeling
- BDI-II
- Beck Depression Inventory, second edition
- CGRP
- calcitonin gene-related peptide
- CHP
- cortical hyperperfusion
- HIT-6
- Headache Impact Test-6
- MHDs
- monthly headache days
- PCA
- posterior cerebral artery
- PM
- posterior part of the territory of the MCA
- PPV
- positive predictive value
- rCBF
- regional CBF
SUMMARY
PREVIOUS LITERATURE:
Concentrations of calcitonin gene-related peptide (CGRP), a neuropeptide and potent endogenous vasodilator, are reportedly higher in patients with migraine, during both attacks and interictal periods, reflecting ongoing activation of the trigeminal nervous system. This state of high endogenous CGRP levels, including during interictal periods, likely causes cortical hyperperfusion (CHP) on MR imaging arterial spin-labeling (ASL). Migraine is associated with depression and insomnia, both of which are independently associated with decreased CBF. Therefore, studies during migraine attacks, when CBF fluctuations are dramatic or studies that do not take into account the presence or absence of depression and insomnia have not yielded useful results.
KEY FINDINGS:
Patients with migraine may have CHP on ASL during the interictal period. Especially in patients with migraine without insomnia, the frequency of CHP (89 of 97, 92%) was significantly higher than in control subjects (1 of 26, 4%). This finding demonstrated excellent diagnostic accuracy for interictal migraine.
KNOWLEDGE ADVANCEMENT:
The present study suggests that findings of CHP on ASL during the interictal period as the only characteristic imaging findings of migraine at present may be clinically very useful as an auxiliary diagnostic tool in addition to medical history.
Previous studies have provided suggestive-but-fragmentary knowledge about regional CBF (rCBF) during migraine attacks and auras.1,2 This issue is because CBF fluctuates dynamically during a migraine attack and significant results are difficult to obtain from sporadic rather than continuous measurements. Furthermore, migraine has been widely shown to be associated with depression and insomnia.3 Depression and insomnia are interrelated, and both may be independently associated with decreased CBF and impaired CBF autoregulation.4,5 Moreover, CBF autoregulation in patients with migraine is also impaired.6 Different results would, therefore, seem likely when studying CBF during attacks in patients with migraine without considering the presence or absence of depression or insomnia.
Calcitonin gene-related peptide (CGRP) is an important neurotransmitter in the migraine headache-generating trigeminovascular system and is believed to play a crucial role in migraine pathophysiology.7 CGRP, a highly potent microvascular vasodilator, is the most abundant neuropeptide in the trigeminal system, and is found in capsaicin-sensitive C fibers that follow the cerebral and meningeal arteries to innervate tissues.8 CGRP induces endothelium-independent vasodilation via direct actions on vascular smooth-muscle cells in the cerebral and coronary vascular beds. CBF autoregulation is, in part, mediated by CGRP.9 CGRP concentrations in plasma, tears, and saliva are reportedly higher during migraine attacks as well as in patients with migraine during nonattacks than in healthy subjects.10,11 In addition to CGRP, molecules such as vasoactive intestinal peptide and nitric oxide, which are intricately related to the pathologic mechanism of migraine, are all involved in vasodilation of the intracranial vasculature.12 We have previously encountered findings on interictal MR imaging and arterial spin-labeling (ASL) in migraineurs that resemble cortical hyperperfusion (CHP) seen immediately after epileptic seizures.13,14 These findings may have been due to the effects of vasodilator molecules related to the pathophysiology of migraine described above.
Many image-analysis studies using fMRI have been conducted on patients with migraine but have only aimed to elucidate the pathophysiology of migraine. The advantages of ASL compared with SPECT and PET include absolute quantification, repeatability, avoidance of IV contrast administration and, overall, superior spatial resolution and sensitivity.2 Additionally, because functional near-infrared spectroscopy is a noninvasive method for measuring cerebrovascular reactivity, it is more suitable for evaluating the vascular effects of migraine drugs rather than for diagnostic imaging.15
Studies of ASL performed during the interictal period also reported that patients with migraine showed hyperperfusion of the some gyri, compared with healthy subjects.2,16 These ASL studies attempted to identify migraine-specific imaging markers that reflect brain tissue perfusion through voxel-based CBF analysis. However, clinically useful image findings have not yet been obtained. Although the main purpose of MR imaging is to exclude secondary headaches, structural changes in the brains of patients with migraine are known to include an increase in cortical thickness, which reflects abnormal neuron hyperexcitability.17 However, because there are individual differences in baseline cortical thickness depending on factors such as age, structural MR imaging findings are not suitable for diagnosing migraine itself.
In this prospective study, we measured CBF during the interictal period of patients with migraine using minimally invasive MR imaging ASL and compared the findings with those of healthy volunteers as control subjects. Given the results, we considered the factors of depression and insomnia in patients with interictal migraine and examined whether there are cerebral circulation characteristics such as CHP findings due to ongoing activation of the trigeminal nervous system, including during the interictal period.
MATERIALS AND METHODS
Institutional Review Board Approval
All study protocols were approved by the Institutional Review Board for Clinical Research (approval no. 22R-078) and the Conflict of Interest Management Committee (approval No. 22–168) at our university. The study protocol was implemented in accordance with the Declaration of Helsinki, and all patients provided written informed consent before participating in the study. In all patients with migraine, written informed consent for participation was obtained for the prospective study of data acquired during routine medical treatments based on national legislation and institutional requirements. Our report complies with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies.
Patients
All patients with migraine fulfilled the diagnostic criteria for migraine established in the third edition of the International Classification of Headache Disorders by the International Headache Society.18 Each patient with migraine showed normal results from neurologic examinations, MR imaging, and MRA. Excluded were patients younger than 18 years of age; smokers; patients with diabetes mellitus, epilepsy, cardiovascular disorders, ongoing treatment with calcium blockers or beta blockers, alcohol abuse, cerebrovascular disease; or those with known systemic diseases such as anemia and hypertension. None of the patients had received Botulinum Toxin injections or CGRP inhibitors.
Of the 266 patients with migraine attending our facility during the study period, 242 patients (age range, 18–75 years; male/female ratio: 27/215) with a clinical diagnosis of migraine who were outpatients at our institution between October 2022 and May 2023 were included in this prospective cross-sectional study.
Patients with migraine were compared with a control group of 26 healthy volunteers (age range, 22–45 years; male/female ratio: 9/17) selected from our hospital staff with no history of headaches, insomnia, and depression using exclusion criteria identical to those for the groups of patients with migraine.
MR Imaging Perfusion Protocols
CBF studies using MR imaging ASL were performed for all patients with migraine during the interictal period (at least 48 hours after the last attack and migraine treatment such as triptanes). The upper limit from the last migraine attack to the scan was 7 days (168 hours). Consumption of caffeine was forbidden on the day of MR imaging ASL. We performed all MR imaging studies at our hospital on a 1.5T MR imaging scanner (Signa Explorer; GE Healthcare) with an Express head-neck array coil. All MR imaging examinations were completed within 16–18 minutes and included conventional axial T1WI, FLAIR, DWI, MRA, and ASL. The total scanning time of the ASL sequence was approximately 2 minutes 30 seconds. In addition to routine imaging sequences, we acquired 3D pulsed continuous ASL (also known as pseudocontinuous ASL) images with background suppression using the following parameters: TR, 4548 ms; TE, 10.5 ms; FOV, 24 cm; 512 sampling points on 6 spirals (matrix size, 512 × 6); spatial resolution, 5.0 mm; section thickness, 4 mm; number of sections, 30; excitations, 2; bandwidth, 62.50 Hz; and labeling time, 1.5 seconds. On the basis of a recently published white paper,19 pseudocontinuous labeling, background suppression, a segmented 3D readout without vascular crushing gradients, and calculation and presentation of both label/control difference images and CBF in absolute units using a simplified model are recommended for optimal default implementation of ASL. The ASL performed in this study used the latest ASL sequence by GE Healthcare, which meets all these recommended conditions. We routinely used 2 postlabeling delays (short ASL, 1525 ms; delayed ASL, 2525 ms). In this study, a postlabeling delay of 1525 ms was used for the CBF analysis because no patients with severe cerebrovascular stenosis were included. Another reason is that longer postlabeling delays reduce the SNR due to relaxation of T1.
For the quantitative ROI analysis of the ASL map, we used the fully-automated ROI-based analysis software 3D stereotaxic ROI template (3DSRT Neuro; FUJIFILM) for the positioning or selection of an ROI offering objectivity and excellent reproducibility.20 The obtained quantitative CBF images were registered anatomically to the standard brain atlas. The 3D stereotaxic ROI template software has ROIs predefined on the standard brain atlas and provides rCBF values for each of the right and left sides of the following 9 regions: callosomarginal, precentral, central, parietal, angular, temporal, posterior cerebral, pericallosal, and thalamus. We determined rCBF in the territories of major cerebral arteries as previously described (Online Supplemental Data).21
We confirmed that there was no significant laterality in rCBF by calculating the asymmetry index (AI) for control subjects and patients with migraine. If there was no significant lateral difference in rCBF, we averaged the left and right regional CBFs and calculated the mean (SD).
AI was calculated for the rCBF as follows:

An absolute AI value of >10 indicated asymmetric perfusion.14
In this study, as with the diagnostic criteria for hyperperfusion immediately after an epileptic seizure or postoperative Moyamoya disease, an ROI was defined as exhibiting hyperperfusion if CBF in the ROI was at least 2 SDs higher than the mean reference value for CBF in control subjects.13 CHP was considered present if ≥2 hyperperfusion cortical ROIs were identified in each cerebral lobe in the unilateral hemisphere.13
Variables, Data Extraction, and End Points
The primary end point of this study was to identify the appearance of CHP findings on MR imaging ASL as a feature of the cerebral circulation in patients with migraine during headache-free periods.
One or 2 months before performing MR imaging, we extracted the number of monthly headache days (MHDs) from headache diaries. A headache day was defined as any day on which a patient recorded any type of headache. Moreover, we extracted the following characteristics from the patient medical records: sex; age; age range (in groups of 18–40, 41–60, and 61–75 years of age); episodic migraine; chronic migraine; aura; Headache Impact Test-6 (HIT-6)22; morning migraine; Athens Insomnia Scale (AIS);23 Beck Depression Inventory, second edition (BDI-II);24 menstrual migraine; weather-related migraine; medication overdose headache; tension-type headache; selective serotonin reuptake inhibitor use; and concomitant prophylactic treatment. We defined “morning migraine” as waking up in the morning with a migraine caused by dehydration, sleep deprivation, or stress. Insomnia was defined as AIS ≥ 4, and depression, as BDI-II ≥ 11.
Statistical Analysis
All statistical analyses were performed using commercially available software (SPSS Statistics for Windows, Version 27.0; IBM).
Distributions of each variable were checked for normality using the Shapiro-Wilk test. The significance of clinical factors potentially associated with a finding of CHP on MR imaging ASL was determined using the Fisher exact test. Continuous variables (age, MHDs, HIT-6, AIS, and BDI-II) were tested using an independent samples Student t test. The homogeneity of variance was analyzed using the Levene test. Values of P < .05 were considered statistically significant. All data are presented as mean (SD) unless otherwise specified. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value were calculated using standard formulas.
RESULTS
Frequencies and Clinical Features of CHP in Patients with Migraine
No lateral differences in rCBF were identified according to AI in any patient with migraine. We, therefore, averaged left and right local CBF on the basis ROIs in control subjects and patients with migraine and then calculated the mean (SD). The baseline CBF values for hyperperfusion obtained from the mean (SD) of rCBF for each cortical region (anterior cerebral artery [ACA], anterior part of the territory of the MCA, posterior part of the territory of the MCA, posterior cerebral artery [PCA]) in control subjects were ≥60 in all regions (Table).
| Cases | ACA | AM | PM | PCA | Tha | |
|---|---|---|---|---|---|---|
| Healthy control | 26 | 48 (SD, 6)b | 49 (SD, 7)b | 48 (SD, 6)b | 47 (SD, 6)b | 45 (SD, 6)b |
| Baseline for hyperperfusion | 60 | 63 | 60 | 59 | 57 | |
| Migraine without insomnia | 97 | 62 (SD, 6) | 64 (SD, 5) | 63 (SD, 5) | 61 (SD, 5) | 56 (SD, 6) |
| Migraine with insomnia | 145 | 51 (SD, 7)b | 52 (SD, 7)b | 51 (SD, 7)b | 50 (SD, 8)b | 48 (SD, 6)b |
| Migraine without depression | 166 | 57 (SD, 8) | 59 (SD, 8) | 58 (SD, 8) | 56 (SD, 8) | 53 (SD, 7) |
| Migraine with depression | 76 | 51 (SD, 8)b | 53 (SD, 8)b | 52 (SD, 8)b | 51 (SD, 8)b | 49 (SD, 7)c |
| Migraine without both insomnia and depression | 91 | 62 (SD, 6) | 64 (SD, 5) | 63 (SD, 5) | 60 (SD, 5) | 56 (SD, 6) |
| Migraine with either insomnia or depression | 151 | 51 (SD, 8)b | 53 (SD, 8)b | 52 (SD, 8)b | 50 (SD, 8)b | 49 (SD, 7)b |
Note:—Tha indiates thalamus; AM, anterior part of the territory of the MCA; PM, posterior part of the territory of the MCA.
aData are means. Insomnia was defined as a score of ≥4 on the AIS. Depression was defined as a score of ≥11 on the BDI-II. The unit for CBF is mL/100 g/min. rCBF data in migraineurs without insomnia (or depression) were compared with those in healthy controls and migraineurs with insomnia (or depression) and evaluated by ANOVA followed by the Tukey honestly significant difference test.
bP < .001.
cP = .01.
Comparison of CBF using MR imaging of ASL in control subjects and patients with migraine with and without insomnia and/or depressiona
The overall frequency of CHP was significantly higher in patients with migraine (115 of 242, 48%) than in control subjects (1 of 26, 4%) (Online Supplemental Data).
Clinical features associated with CHP in patients with migraine are shown in the Online Supplemental Data. Because data for MHDs and HIT-6 were not normally distributed, nonparametric tests were used for analyses. As a result, the clinical factor significantly associated with CHP in patients with migraine was the age group of 18–40 years as a positive factor. Negative factors for CHP findings were the age group of 41–60 years, morning migraine, AIS, AIS ≥ 4, BDI-II scale, BDI-II ≥ 11, and the use of an oral selective serotonin reuptake inhibitor (Online Supplemental Data). Episodic migraine, chronic migraine, and aura were not significantly associated with CHP findings.
Clinical factors with a significance level of P < .10 were subjected to multivariable logistic regression analysis with the presence of CHP as the dependent variable. Multivariable analysis revealed that significant positive clinical factors associated with CHP in patients with migraine were the age group of 18–40 years (OR = 2.985; 95% CI, 1.381–6.452; P = .005) and AIS <4 (absence of insomnia) (OR = 53.598; 95% CI, 22.519–127.57; P < .001). In multivariable analysis, the association between patients with migraine with depression and CHP was not significant.
Comparison of CBF in Patients with Migraine with/without Insomnia
Among 145 patients with migraine with insomnia, 70 (48%) had depression. Of the 76 patients with migraine with depression, 70 (92%) also had insomnia.
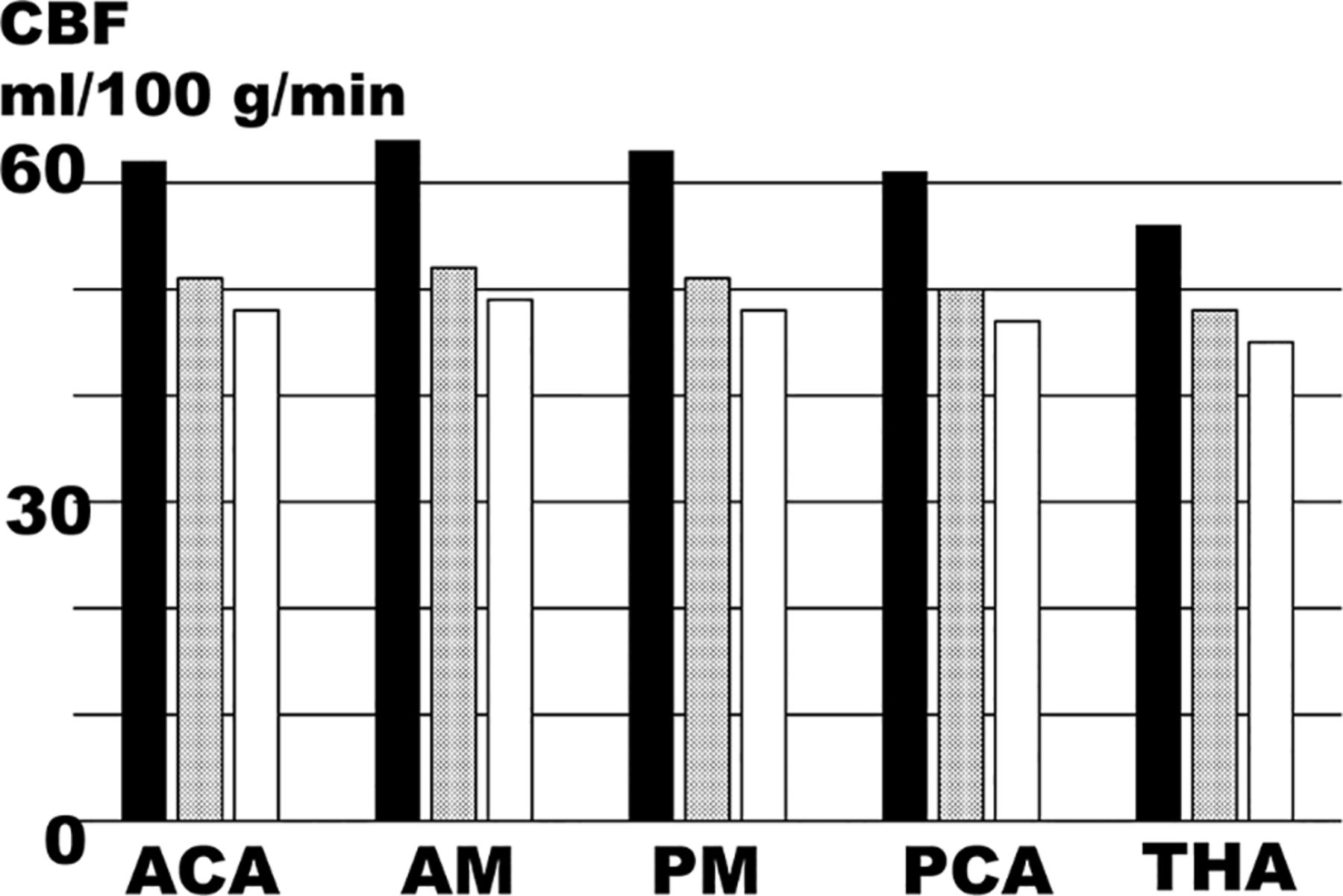
Patients with migraine were subgrouped according to the presence or absence of insomnia and/or depression, and rCBF during headache-free periods in each ROI was compared with that in control subjects (Table and Online Supplemental Data). Because our data for CBF were normally distributed, we used 1-way ANOVA for analysis of multiple comparisons to test for significant differences in CBF data between the clinical groups. Homogeneity of variance was analyzed by using the Levene test. Equal variance of CBF data from each clinical group was confirmed, so the significance of ANOVA was determined by the Tukey honestly significant difference test (Table and Online Supplemental Data). Consequently, in all ROIs, rCBF was significantly higher in patients with migraine without insomnia than in patients with migraine with insomnia or control subjects. However, no significant differences in rCBF were seen between patients with migraine with insomnia and control subjects in any ROIs (Fig 1). Typical CHP findings on ASL in patients with migraine without insomnia, patients with migraine with insomnia, and healthy controls are shown in Fig 2.

Values of rCBF during the interictal period in patients with migraine with/without insomnia. These plots are graphical representations of the data presented in the Table. In bar graphs of mean rCBF, black bars indicate migraine without insomnia, dotted bars indicate migraine with insomnia, and white bars indicate healthy controls. THA indicates rCBF in the territory of the thalamus; AM, anterior part of the territory of the MCA; PM, posterior part of the territory of the MCA.

{kind=link}
{kind=link}
Findings from MR imaging ASL. A, Typical CHP findings in a 41-year-old woman with episodic migraine without insomnia. B and C, Normal findings without CHP in a 48-year-old woman with chronic migraine complicated by insomnia (B) and a 30-year-old woman from the healthy control group (C).
Similarly, in all ROIs, rCBF was significantly higher in patients with migraine without depression than in patients with migraine with depression or control subjects. Moreover, in all ROIs, rCBF was significantly higher in patients with migraine without both insomnia and depression than in patients with migraine with either insomnia or depression or control subjects.
The statistical significance of pair-wise comparisons against rCBF data in patients with migraine was evaluated with ANOVA followed by the Tukey honestly significant difference test. Comparison of patients with migraine with insomnia, depression, and those with migraine with either insomnia or depression, and healthy controls showed no significant difference in rCBF in any ROI.
Accuracy of Migraine Diagnosis Based on Hyperperfusion on MR Imaging ASL
In patients with migraine without insomnia, regarding the diagnostic accuracy of CHP findings for migraine in the interictal period, sensitivity was 0.918, specificity was 0.962, and PPV was 0.989, showing excellent accuracy. In all cases and patients with migraine with insomnia, the sensitivity was low at 0.475 and 0.179, respectively, but the specificity was 0.962 and 0.962, respectively, and the PPV was good at 0.991 and 0.963, respectively.
DISCUSSION
Mechanisms of CHP in Patients with Migraine
This study showed that patients with migraine, especially those without insomnia, may have interictal CHP. Functional MR imaging is useful for identifying changes in functional connectivity in migraine that are thought to be related to cortical spreading depolarization. However, because blood oxygenation level–dependent signals obtained from fMRI do not directly reflect cerebral perfusion,16 there are no studies that can be used as a reference for considering the mechanism of CHP in migraine. We speculate that cortical hyperexcitability, which plays an important role in the development of migraine in the trigeminal nerve-thalamocortical pathway, is the cause of CHP. In fact, a previous study of voxel-based CBF analysis of ASL during the interictal period reported high CBF levels in visual, somatosensory, multisensory integration cortices, superior frontal gyri, and postcentral gyri in interictal ASL in patients with migraine with aura.16
The mechanism of CHP may also involve vasodilatory neurotransmitters that are associated with migraine development. CGRP mediates CBF autoregulation, in part, by inducing endothelial-independent vasodilation through direct effects on cerebral vascular smooth-muscle cells.9 Moreover, CGRP released from the trigeminal perivascular nerve is also a potent direct vascular smooth-muscle dilator that counteracts vasoconstriction and hypoperfusion of the cerebral vascular bed as a rescue mechanism in cerebral ischemia.9,25,26
Concentrations of CGRP in plasma, tears, and saliva are reportedly higher in patients with migraine both during attacks and during the interictal period compared with healthy subjects.10,11 Thus, the presence of elevated CGRP levels not only during headache attacks but also during the interictal period indicates that the trigeminal nervous system is continuously activated during headache attacks and during the interictal period.10 Normally, endogenous CGRP does not change CBF at the steady state. However, migraine,6 insomnia, and depression are never steady states due to impaired CBF autoregulation. Therefore, a state of high endogenous CGRP levels resulting from ongoing activation of the trigeminal nervous system, including during interictal periods, likely causes CHP on ASL.
ASL Findings in Patients with Migraine Headache with Insomnia and Depression
A common neurophysiologic mechanism underlying both insomnia and depression is hyperactivation of the hypothalamic-pituitary-adrenal axis, which indirectly results in impaired CBF autoregulation.4,27 There have also been reports of decreased local CBF in the frontal medial, occipital, and parietal cortices and basal ganglia in patients with insomnia.5,28 Studies of CBF in migraine that do not consider the presence or absence of depression or insomnia would thus seem unlikely to yield results in consensus.
CGRP may be involved in the pathophysiology of depression, and a significant increase in CGRP levels has been reported in patients with migraine with depression.11 Thus, although CGRP concentration is known to be high in depression, CBF in this study was low among patients with migraine with depression, and the vasodilatory effects of CGRP were not reflected. Previous studies have shown that homocysteine levels in patients with depression were significantly higher.29 Elevated plasma levels of homocysteine resulted in reduced nitric oxide bioavailability and hypertrophy of vascular smooth-muscle cells, which could decrease the ability of vascular dilation.4,30 On the basis of these findings, we think that because the vasodilatory ability is reduced in depression and/or insomnia, which is strongly associated with depression, the vasodilatory effect of CGRP is less likely to occur. As a result, the frequency of CHP may be low in migraine complicated with depression and/or insomnia. In the future, we believe it is important to study how insomnia and depression affect the trigeminovascular system, CGRP levels, and CBF autoregulation in patients with migraine.
Neuroradiologic Diagnosis of Migraine by CHP Findings on ASL
Previous migraine studies using ASL did not emphasize the presence of CHP.2,16 In contrast, because the strengths of our study compared with previous studies include the large sample size, grouping analysis by presence or absence of insomnia and depression, and strict interictal ASL implementation, we were able to clarify the presence of CHP as a characteristic finding of ASL in patients with migraine.
The CHP findings in this study were more frequent and clinically useful in patients with migraine without insomnia and depression. Moreover, because the CBF value in CHP was ≥10 mL/100 g/min higher than that in healthy controls, the hyperperfusion pattern for the cortex on ASL images is visually impressive. CHP, therefore, seems to allow an easy one-shot diagnosis without checking the CBF value. In addition, if migraine is clearly diagnosed according to the diagnostic criteria, but no CHP findings are evident, insomnia or depression should be suspected, and clinical/psychological medical examinations should be required. These will allow headache specialists to treat migraines more precisely. On the basis of the above, we emphasize that CHP findings on ASL are clinically very useful as one of the supplementary diagnostic tools in addition to interviews, as the only impressive imaging finding for migraine at present.
The differential diagnosis for CHP includes nonconvulsive status epilepticus.13,14 Additionally, those with typical aura without headache18 and patients with a family history of migraine may also present with CHP findings, and this possibility is currently under investigation.
Limitations
This study has some limitations. First, it relied on indirect evidence from previous studies, because we were unable to test our hypothesis by simultaneously measuring CGRP levels in both patients with migraine and control subjects and correlating them with ASL findings.
Second, relatively low SNR and low temporal resolution, as the key limitations of ASL, have been overcome due to technical advances in MR imaging.1 However, ASL remains vulnerable to head-movement artifacts, so the existence of cases that compromised the reliability of CBF values cannot be ruled out. In addition, ASL perfusion findings may be influenced by various factors, such as the MR magnetic field (1.5T versus 3T) and limitation of using single delay, sex, age, and the effect of medications on CBF measures.
Third, the reproducibility of CBF measured with ASL was not assessed. In the future, repeat interval scans will need to be performed to confirm that the results of this study are a consistent phenomenon rather than obtained by chance.
Fourth, because the main purpose of this study was to demonstrate that migraine can be diagnosed on the basis of the finding of CHP on ASL, we did not perform a group-level voxelwise CBF analysis to look for the spatial extent of the abnormalities.
CONCLUSIONS
Patients with migraine without insomnia may have CHP during the interictal period; however, the findings of the present study need to be prospectively validated on a larger scale before clinical applicability can be considered.
Acknowledgments
The authors are grateful to the radiologic technologists and nursing staff at our institute for their assistance in this work.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- Received November 7, 2023.
- Accepted after revision January 25, 2024.
- © 2024 by American Journal of Neuroradiology