SUMMARY:
The parasellar ligaments have been previously described in cadaver specimens and intraoperatively, but identification on MR imaging has eluded radiologists. Using high-resolution T2-weighted MR imaging, we identified the parasellar ligaments as T2-hypointense, bandlike structures that emanate from the medial wall of the cavernous sinus. Subsequent dissection of the same specimen provided matching anatomic images of the parasellar ligaments identified on MRI. This imaging finding is important because resection of the medial wall of the cavernous sinus has been tied to improved outcomes for gross total resection and endocrinologic remission of functioning pituitary adenomas.
ABBREVIATIONS:
- MWCS
- medial wall of the cavernous sinus
- NEX
- number of excitations
The cavernous sinus is a complex structure that houses critical anatomy such as the ICAs and cranial nerves.1 Recent studies have underscored the importance of the medial wall of the cavernous sinus (MWCS) in improving outcomes for functional pituitary adenoma surgery.2 Within the cavernous sinus, the parasellar ligaments are important structures that extend from the MWCS to the ICAs and cranial nerves.3 Despite their anatomic significance, the parasellar ligaments have remained elusive on MR imaging. The purpose of this report is to describe the imaging appearance of the parasellar ligaments on MR imaging.
Imaging
All imaging was performed on a research-only compact 3T scanner (GE Healthcare).4 A standard coronal T2-weighted sequence that mimics our clinically used protocol was initially run (slice thickness, 3 mm; TR, 3025 ms; TE, 101 ms; 160-mm field of view; number of excitations (NEX), 1; acquisition time 55 seconds). This clinical sequence demonstrated hazy T2-isointense signal in the cavernous sinus, immediately adjacent to the pituitary gland (Fig 1A). In our experience, ill-defined signal in the cavernous sinuses on the coronal T2-weighted sequence is a typical finding, without having sufficient spatial resolution to identify the parasellar ligaments.

A, A standard 3-mm-thick coronal T2-weighted sequence shows hazy signal (arrows) in the cavernous sinus. B, High-resolution 0.5-mm slice thickness imaging resolves these hazy structures as distinct T2-hypointense bands that represent the parasellar ligaments (upper arrow indicates the anterior horizontal ligament; lower arrow, the periosteal ligament).
An additional high-resolution T2-weighted sequence was then performed to further resolve the structures within the cavernous sinus (slice thickness. 0.5 mm; TR, 4372 ms; TE, 100 ms; 160-mm field of view; NEX, 6; acquisition time, 21 minutes 13 seconds).
The higher-resolution imaging further resolved the ill-defined signal in the cavernous sinus as distinct T2-hypointense bands (Fig 1B). The bands run from the MWCS that directly abuts the lateral aspect of the pituitary gland and fan outward as they extend laterally toward the ICA and the lateral wall of the cavernous sinus. These distinct bands correlate with the parasellar ligaments (Fig 2), specifically the anterior horizontal ligament and periosteal ligament.

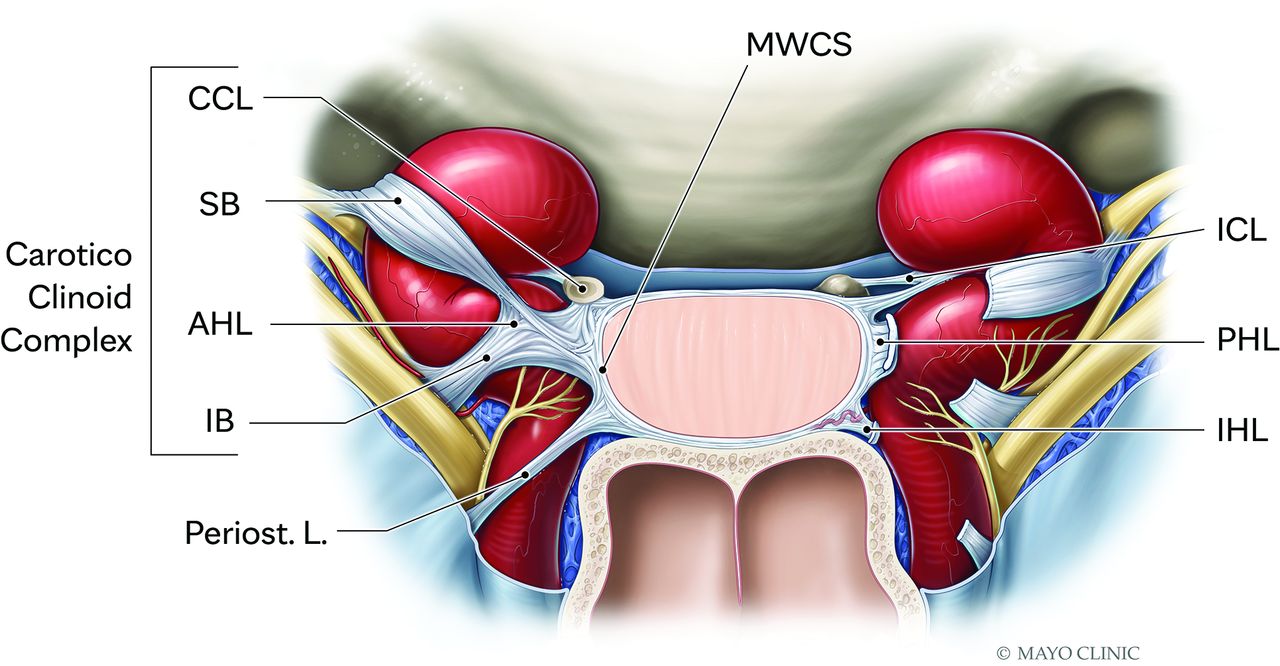
Illustration of the parasellar ligaments demonstrate the “candy wrapper” configuration that originates on the MWCS and fans out laterally as the ligaments extend to the cavernous segment of the ICA and the lateral wall of the cavernous sinus. CCL indicates carotid-clinoid ligament; AHL, anterior horizontal ligament and the associated SB, superior branch; IB, inferior branch; Periost. L., periosteal ligament; ICL, interclinoid ligament; PHL, posterior horizontal ligament; IHL, interclinoid ligament. This illustration has been modified from the original version.3
Anatomy Report
For this study, we used 1 embalmed cadaveric specimen prepared as previously described.5 Briefly, for the latex injection both the common carotid and vertebral arteries as well as internal jugular veins were isolated and cannulated with stainless steel cannulas and perfused with red and blue latex, respectively.
To expose and describe the pituitary region and ligaments, we performed a regular transsphenoidal approach. With a zero-degree endoscope, both middle and superior turbinates on both sides of the nasal cavity were lateralized, revealing the ostium of the sphenoid sinus. A Kerrison rongeur was used to enlarge the ostium and enter the sphenoid sinus cavity. Within the sphenoid sinus, the septum was drilled, and the bony landmarks, recesses, and prominences were exposed. The dissection proceeded by drilling the sellar prominence and moving laterally to the carotid prominence. Once the dura covering the pituitary gland and anterior bend of the ICA were exposed, a retractable knife was used to incise and expose the dura. The incision was performed at the level of the anterior intercavernous sinus, moving laterally to open the anterior wall of the cavernous sinus and its contents. Last, using 0° and 30° scopes, we dissected the pituitary region and cavernous sinus and photo documented them, preserving the pituitary ligaments and their landmarks, in particular their origins and insertions in the surrounding structures (Fig 3, Supplemental Data).

{kind=link}
{kind=link}
{kind=link}
Endoscopic image from the same cadaver specimen from Fig 1. The distinct T2-hypointense bands in the right cavernous sinus seen on MRI correspond to the right parasellar ligaments. Specifically. the anterior horizontal ligament (upper arrow) and the periosteal ligament (lower arrow).
DISCUSSION
The cavernous sinus is an important anatomic region to understand during resection of functioning pituitary adenomas. Resection of the MWCS, even in the absence of macroscopic invasion, has been shown to be associated with improved outcomes including gross total resection and endocrinologic remission.2 Surgical resection of the MWCS is not without risk, with many important structures including the ICA and cranial nerves residing in the cavernous sinus. The parasellar ligaments have been described as key anatomic structures that connect the MWCS to the ICA and are therefore required to be transected during MWCS resection. Preoperative identification of the parasellar ligaments could therefore help with surgical planning to avoid carotid artery injury. While these structures have been described in cadaver specimens, we present a case of MR imaging of the parasellar ligaments with anatomic correlation.
The MWCS is a thin single-layer structure comprising the meningeal dura that is difficult to see on MRI.3 The resection of the MWCS has been shown to be of increasing importance in achieving biochemical cure of functioning pituitary adenomas and to prevent recurrence in nonfunctioning adenomas.6⇓-8 Parasellar ligament transection is important in the resection of the MWCS from the surrounding neurovascular structures.3
Kehrli et al9 theorized that the fetal pituitary gland is wrapped in a mesenchymal mass, of which the parasellar ligaments are remnants, a process that leads to variability in the ligaments. The parasellar ligaments are fan-shaped structures originating from the MWCS and extending to the tunica adventitia of the ICAs and laterally to the cranial nerves in what has been described as a “candy-wrapper” configuration.3 The parasellar ligaments, when studied in cadaver models, have a variable configuration but are grossly organized into anterior and posterior groups. The anterior horizontal ligament and posterior horizontal ligament, identified on our specimen, reside in the anterior and posterior groups, respectively.
Case Summary
We present high-resolution MR imaging of the parasellar ligaments. These ligaments are important structures that connect the MWCS to the ICAs and cranial nerves and have previously been described with gross visualization in cadaver models and intraoperatively, but not previously, with MR imaging. The MWCS is an increasingly important structure in achieving endocrinologic remission following the resection of functioning pituitary adenomas; therefore, the parasellar ligaments have newly recognized relevance for surgical planning.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- Received November 19, 2024.
- Accepted after revision January 11, 2025.
- © 2025 by American Journal of Neuroradiology