
Abstract
Summary: A 29-year-old woman presented with dilated epidural veins and incapacitating headache after undergoing a lumbar puncture. Two months later, the results of follow-up MR imaging were normal. These findings suggest that temporary dilation of the epidural vein may occur in association with post-lumbar puncture intracranial hypotension syndrome. In these cases, it seems useful to confirm whether the patient has recently undergone a lumbar puncture.
Giant cervical epidural veins are rarely seen on imaging studies. In most cases, major enlargement has been caused by an unknown arteriovenous malformation or a jugular vein thrombosis. We present a rare case of cervical epidural vein dilation.
Case Report
A previously healthy 29-year-old woman presented with vertigo and neck pain. A neurologic examination revealed a positive right Romberg's sign. The remaining results of the neurologic examination were normal. The results of CT of the head were normal. A lumbar puncture revealed a normal opening pressure, a normal WBC, a protein level of 83 mg/dL, and a normal glucose level. Cultures were negative, and the results of a cytologic examination were normal. Extensive study of the CSF disclosed no other abnormalities.
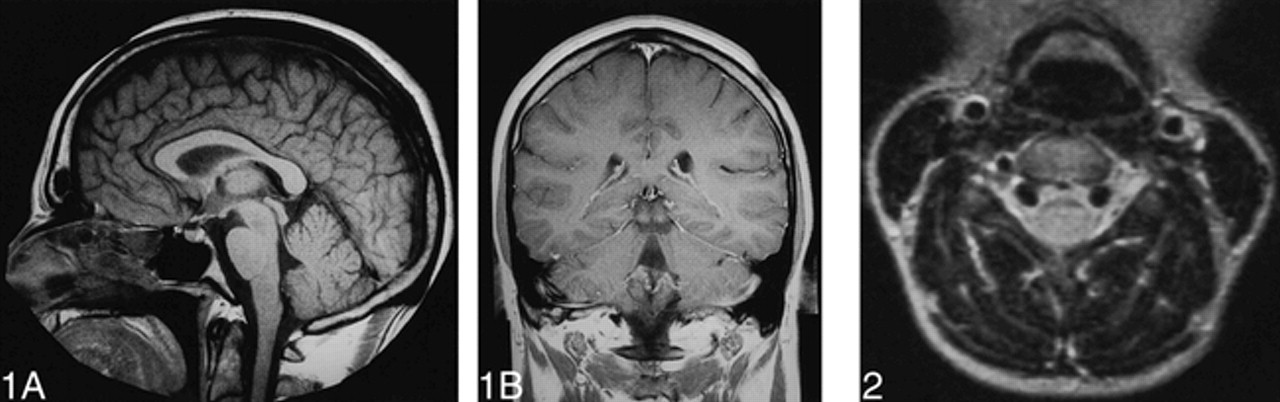
A few hours later, a very incapacitating postural headache occurred. The results of a neurologic examination were unchanged, and MR imaging of the head showed no parenchymal abnormalities (Fig 1A and B). MR images of the cervical spine (Fig 2) and contrast-enhanced CT of the neck (Fig 3A–B) revealed dilated cervical epidural veins. No intracranial or spinal arteriovenous fistula (AVF) or compressive lesion of the spine was identified. The internal jugular veins were asymmetrical, with a small left jugular vein (Fig 2). The left vertebral artery was not visible. Transcranial and cervical Doppler sonography revealed a small but patent left vertebral artery. The patient was treated by analgesic medication and improved with rest. Two months later, the results of a clinical examination and MR imaging of the cervical spine were normal. Asymmetrical internal jugular veins were unchanged (Fig 4).

MR images show no intracranial abnormalities.
A, Sagittal spin-echo T1-weighted MR image.
B, Frontal spin-echo T1-weighted MR image with contrast enhancement.
fig 2. Axial spin-echo proton density–weighted MR image shows bilateral giant epidural cervical venous plexus.

Contrast-enhanced CT scans show epidural vein dilation.
A, Axial view.
B, Frontal view.
fig 4. Two months later, axial gradient-echo T2-weighted MR images show venous dilation disappearance.
Discussion
The cervical epidural venous system provides independent accessory venous drainage from the intracranial compartment. In a normal patient, the cervical epidural veins are opacified from the occipital foramen down to the superior thoracic spine by bilateral injections of the vertebral veins (1). There is no posterior epidural vein in the cervical spine as in the lumbar spine. The entire cervical epidural vein system is located in the anterolateral angles of the spinal canal. The epidural veins on each side communicate with each other by a venous anastomosis located behind each vertebral body, and the cervical epidural veins anastomose with extravertebral veins superiorly and laterally. The cervical epidural veins are connected superiorly to the suboccipital plexus and to the anterior condyloid vein, which is in continuity with the inferior petrosal sinus. Laterally, the cervical epidural veins are connected to the vertebral plexus that surrounds the vertebral artery in the transverse foramen (2). Contrary to standard anatomic description, the vertebral vein is individualized as a single vein only at its terminus; the vertebral vein drains into the subclavian vein medial to the internal jugular vein.
In a healthy person, the cervical epidural vein may enlarge in the upright position (major route for venous intracranial outflow) or during the rise of the intraabdominal or interthoracic pressure (accessory route of venous return). It is also involved in regulating intracranial pressure by transmitting the respiratory and cardiac pressures to the intracranial compartment and stabilizing the pressure within the venous system (1).
It may also enlarge in pathologic situations such as when compressive lesions of the spinal cord or disk disease is present. Enlarged epidural veins are often seen in association with intracranial or spinal AVF or processes causing impaired drainage of the internal jugular circulation, where the epidural veins serve as a collateral pathway (ie, superior vena cava thrombosis).
Intracranial hypotension syndrome is defined as a syndrome with which reduced CSF pressure may occur after spinal puncture, surgery, trauma, or severe dehydration or from spontaneous dural tear (“spontaneous intracranial hypotension syndrome”) (3, 4). After lumbar puncture, an opening may occur in the dural and the arachnoid membranes, which results in CSF leakage. The characteristic intracranial hypotension headache is prompted or aggravated by sitting in an upright position and may be associated with nausea and vomiting. Less frequently, patients experience vertigo, diplopia, or tinnitus, as well as photophobia, neck stiffness, and anomalies in hearing and taste (3, 5). When the syndrome is not recognized, lumbar puncture may be performed and may reveal an abnormal WBC, high protein level, or both. CSF pressure is low or may be unobtainable (3, 4). Suspicion of meningeal infection, tumor, or vascular lesion may lead to further investigation, including MR imaging.
Intracranial imaging findings of intracranial hypotension have been well described in the literature and are thought to be a result of low CSF pressure (3–5). On contrast-enhanced T1-weighted sequences, there is an intense pachymeningeal enhancement secondary to dura mater venous plexus dilation, in accordance with the Monro-Kellie rule (3). Other intracranial MR findings may include subdural fluid collections, a downward displacement of midline brain structures, and slitlike ventricles (3, 4).
The spinal MR findings of intracranial hypotension have been mentioned only scarcely in the literature (3–6), particularly in cases of spontaneous intracranial hypotension. Spinal MR imaging may reveal extradural fluid collection that appears isointense with CSF on T1- and T2-weighted MR images and could be hyperintense related to CSF on proton density–weighted images (7). Mild enhancement of the fluid collection or the adjacent dura may also occur. CT myelography or radionuclide cisternography are generally used to locate the direct site of the CSF leak.
In our patient, the only abnormal MR findings were giant lateral epidural veins. The principal differential diagnosis of dilated epidural veins were disk disease, lesion of the spinal cord, and vascular malformations; however, these abnormalities are associated with other findings, including signal abnormalities, direct evidence of pial lesions, focal lesions, or internal jugular vein thrombosis. Additional imaging planes usually easily clarify the nature of this type of lesion. In our patient, internal jugular veins were asymmetrical, which was considered normal. The left vertebral artery was initially diagnosed as thrombosed based on MR images but was later observed as normal based on a Doppler sonogram. Two months later, the clinical signs had disappeared and the cervical epidural veins were normal.
According to the Monro-Kellie doctrine, CSF volume and intracranial blood volume vary inversely. The Monro-Kellie doctrine, however, refers to the closed, nonexpansible system of the head, so it should not strictly apply to the spinal canal. Even so, we hypothesize that cervical epidural dilation was in part related to the leak of CSF. We have no explanation for the absence of other signs of MR findings of intracranial hypotension syndrome in our case. We conclude that the simultaneous disappearance of the MR findings after the disappearance of the clinical signs strongly suggests a causal relationship.
Acknowledgments
We thank R. Medeiros for valuable advice in editing the manuscript.
Footnotes
↵1 Address reprint requests to Franck Clarot, MD, Service de Neuroradiologie, CHU Ch. Nicolle, 1 rue de Germont, 76000 Rouen, France.
References
- Received June 30, 1999.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}