
Abstract
Summary: Murray Valley encephalitis (MVE) is caused by a flavivirus related to West Nile and St. Louis encephalitis viruses. We report a case of MVE resulting in quadriplegia and respiratory failure. MR imaging demonstrated thalamic hyperintensity on T2-weighted images, with similar involvement of the red nucleus, substantia nigra, and cervical cord. These findings preceded serologic diagnosis and are similar to those of Japanese encephalitis. In the appropriate setting, thalamic T2 hyperintensity is suggestive of flavivirus infection.
Murray Valley encephalitis (MVE) is caused by infection with a flavivirus belonging to the Japanese encephalitis (JE) antigenic complex, which also includes St. Louis encephalitis (StLE) and West Nile (WN) virus. The natural transmission cycle of the JE group involves infection of a mosquito vector alternating with viral amplification in a variety of vertebrate hosts. Human disease is incidental to this cycle. They are neurotropic viruses, which are becoming increasingly important globally as their geographic ranges steadily increase. WN virus, for example, has recently caused a major epidemic of flaccid paralysis in New York (1), and cases of JE have now been reported in northeastern Australia, where the virus may have become established in the wild pig population (2). The radiologic features of JE (3) and StLE (4) have been reported recently. Herein we describe the MR findings in a case of severe MVE. To our knowledge, these findings have not been described previously and correlate well with both the known clinical features of the disease and with the neurotropism of other members of the JE group.
Case Report
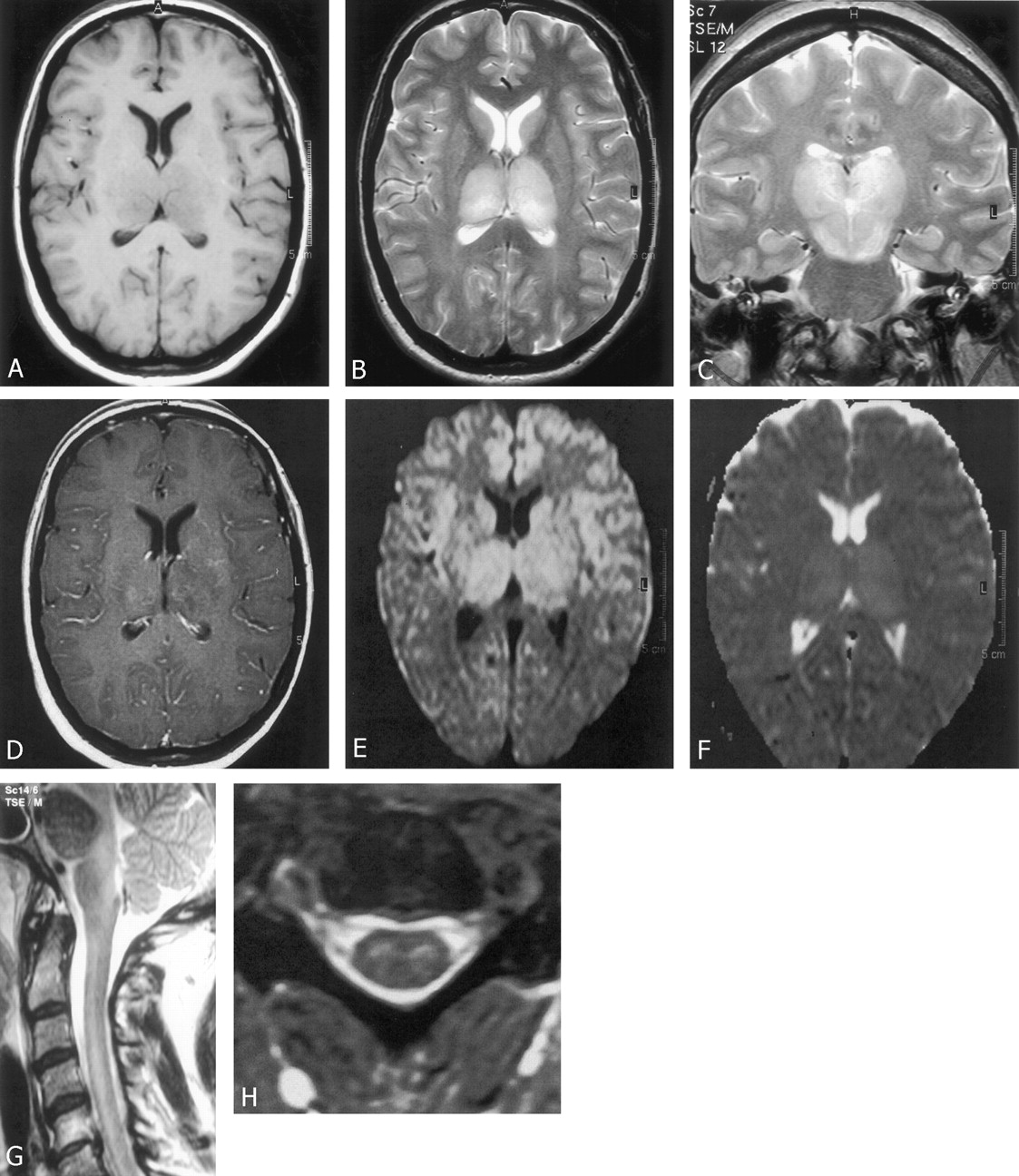
A 49-year-old American woman residing in central Australia for the past 18 months presented with a 3-day history of fever, headache, vomiting, and increasing confusion. On examination, she was febrile (temperature 40°C), with an expressive and mild receptive dysphasia. Tone was increased, with clonus in the lower limbs and her reflexes were symmetrically brisk. Findings on neurologic examination were otherwise normal. Cranial CT findings were normal. CSF examination revealed a prominent lymphocytic pleocytosis (20 polymorphonuclear cells, 800 lymphocytes, and 20 rbc/mm3) and an elevated protein concentration (1.9 g/L). The concentration of glucose was normal (3.1 mmol/L). No organisms were seen. An initial diagnosis of viral encephalitis was made, and therapy with intravenous acyclovir and ceftriaxone was commenced. Increasing confusion and a deteriorating level of consciousness necessitated intubation and transfer to a tertiary referral center for further treatment. Cranial CT performed on arrival, 4 days after the onset of her illness, revealed reduced attenuation of both thalami. MR imaging was performed on day 5 of her illness. This revealed bilateral thalamic involvement with hypointensity on T1-weighted images (Fig 1A) and hyperintensity on T2-weighted images (Fig 1B). Similar changes involved the reticular formation, substantia nigra, and red nuclei within the midbrain with sparing of the long tracts (Fig 1C). There was only minor contrast enhancement (Fig 1D), and diffusion-weighted images showed hyperintensity (Fig 1E) most likely because of T2 shine-through in view of the high signal intensity observed on the corresponding apparent diffusion coefficient map (Fig 1F). More diffuse disease was noted throughout the cervical spinal cord (Figs 1G and H). MR imaging was repeated on day 22 of her illness and revealed persistent but reduced hyperintensity within the thalami on T2-weighted images.

A, Axial spin-echo T1-weighted image (560/14 [TR/TE]) shows hypointensity of the thalami.
B, Axial fast spin-echo T2-weighted image (3641/80) showing hyperintensity of the thalami.
C, Coronal fast spin-echo T2-weighted image (3641/80) shows hyperintensity of both thalami, red nuclei, and substantia nigra.
D, Axial spin-echo T1-weighted image (570/14) reveals subtle heterogeneous enhancement within the thalami.
E and F, Single-shot spin-echo echo-planar axial diffusion-weighted image (E) with diffusion sensitivity of b = 1000 s/mm2 (4832/81) demonstrates bilateral thalamic high signal intensity. Corresponding apparent diffusion coefficient map (F) shows increased diffusion in the region of the thalami. This indicates that high signal intensity demonstrated on the diffusion-weighted images represents T2 shine-through rather than cytotoxic edema.
G, Sagittal fast spin-echo T2-weighted (2654/100) image of the cervical spine show diffuse hyperintensity of the central cord.
H, Axial gradient-echo T2-weighted (697/14; flip angle, 25°) image of cervical spine shows hyperintense gray matter within the cord.
A diagnosis of MVE was made on day 8, when her CSF tested positive for MVE RNA by polymerase chain reaction. Seroconversion to MVE IgM and IgG occurred on days 8 and 22, respectively. Serologic tests for other pathogens, including those for the related JE and Kunjin virus (an endemic flavivirus that occasionally causes a less severe encephalitis), were negative.
Her admission was complicated by elevated intracranial pressure and obstructive hydrocephalus, requiring the insertion of an external ventricular drain, hyponatremia due to inappropriate antidiuretic hormone secretion, and respiratory failure due to respiratory muscle paralysis and intermittent apnea. After 52 days of management in the intensive care unit she was transferred to a facility in the United States of America for ongoing care and was lost to further follow-up. Her condition at transfer had improved only marginally. A flaccid quadraplegia and right seventh cranial nerve palsy persisted, and she remained ventilator dependent.
Discussion
MVE is enzootic in northern Australia, where environmental conditions allow the major mosquito vector, Culex annulirostris, to maintain persistent MVE activity in mosquito-avian cycles. In these regions, human cases are reported almost yearly (2). In contrast, disease occurring elsewhere in Australia is uncommon but may be epidemic following extreme weather conditions that favor mosquito breeding and the introduction of the virus by migratory wading birds (2). Indeed, the virus was first isolated and named after environmental conditions led to an epidemic within the Murray River basin in southeast Australia in 1951. Both endemic and epidemic MVE are seasonal, with almost all cases being reported between February and July, after heavy summer rains (5).
Serologic studies suggest that clinical disease may occur in as few as 1 in 1000 cases of infection (2). In susceptible individuals such as immunologically naïve children within endemic regions or individuals from nonendemic areas, as in the present case, disease is frequently severe. Respiratory failure due to brain stem involvement and respiratory muscle paralysis was associated with a mortality rate in excess of 40% in earlier case series. This has been significantly reduced by the ready availability of supportive ventilation. Nevertheless, the reported case fatality rate remains over 30%, with severe neurologic sequelae resulting in nearly 20% of survivors (5). Fewer than 50% of patients make a complete recovery (5).
MVE generally presents after a brief, nonspecific prodromal febrile illness. Seizures are a prominent manifestation in children; however, adults usually present with more obviously encephalitic symptoms (5). Cranial nerve palsies, particularly of the seventh nerve, occur in 50% of cases (5). Movement disorders are a major feature in 40% of patients and include choreiform movements, Parkinsonism, and other tremors (5). A flaccid paralysis has recently been described and is a predictor of a poor neurologic outcome and death. Electrophysiologic studies in these cases indicate extensive anterior horn cell involvement (5).
The present case therefore illustrates many of the clinical features of severe MVE with rapid progression to respiratory failure and a flaccid quadriplegia. The imaging findings presented here provide some insight into the neurotropism of the virus and the pathologic basis of the disease. MR imaging performed on day 5 of the illness revealed extensive and bilateral thalamic involvement with hypointensity on T1-weighted images and hyperintensity on T2-weighted images. CT performed the previous day had also demonstrated reduced attenuation within both thalami. Disease extended to involve subthalamic structures, including the substantia nigra, red nucleus, and reticular formation within the midbrain, with extensive involvement of the cervical spinal cord. No hemorrhage was seen within these structures; no cytotoxic edema existed on diffusion-weighted images, and little contrast enhancement was present, indicating only minor blood-brain barrier deficit. Some improvement was noted after several weeks, when MR imaging was repeated.
To our knowledge, only one other report illustrating MR findings of MVE has been published(5). This case was of a 15-month-old aboriginal girl from the far north of Australia who developed a flaccid quadriplegia, similar to that reported here, but who died after 56 days. MR imaging performed after 6 weeks of illness reportedly showed cerebral and cerebellar atrophy with necrosis of the posterior thalami. The only accompanying image published was T1 weighted and revealed bilateral hypointensity of the thalami with prominence of the ventricles. These findings are in accord with the only published autopsy study of MVE, which described extensive and early bilateral destruction of neurons within the thalamus (6). Cellular infiltration of brain stem motor nuclei and the anterior horn of the spinal cord were also prominent autopsy findings. Necrosis of areas of white matter, the thalamus, and cerebellar cortex was demonstrated pathologically later in the disease (6).
The MR features of MVE are very similar to those previously described in JE. Bilateral thalamic involvement is a characteristic radiologic feature of JE and was seen in 29 of 31 patients in whom MR imaging was performed in one series (3). Thalamic lesions are most frequently hypointense on T1-weighted images and hyperintense on T2-weighted images, but high signal intensity on T1-weighted images, consistent with subacute hemorrhage, has also been described (3). The basal ganglia and midbrain are frequently involved by JE. These lesions are more likely to be asymmetric than are those within the thalami, but otherwise have a similar MR appearance (3). The MR findings in JE correlate well with earlier pathologic descriptions of necrolytic and hemorrhagic lesions predominantly within the thalamus, striatum, and pons (7).
Neuroimaging in infections with other JE group flaviviruses is less well documented. Autopsy studies have shown that diffuse neurologic injury occurs in fatal StLE (8), yet there is generally a paucity of radiologic findings (9). Focal lesions that are hypointense on T1-weighted images and hyperintense on T2-weighted images have, however, been described within the substantia nigra (4), and quantitative analysis of autopsy specimens has revealed much more extensive involvement of the substantia nigra than in other areas of the brain, suggesting a degree of specificity for this structure by StLE virus (8). During the recent outbreak of WN virus in New York, MR imaging was performed in 27% of patients; nearly one third of them had enhancement of the leptomeninges or periventricular regions, but there were no reports of specific subcortical regions being affected (1).
The clinical and radiologic features of MVE are consistent with the known neurotropism of other members of the JE group. A flaccid paralysis due to anterior horn cell involvement may result from infection with WN (1), StLE (10), and JE (11) viruses. This process presumably prevented the clinical manifestation of tremor in the case of MVE reported herein. Movement disorders are, however, well described in MVE and are also a major feature of StLE (10) and JE (11). MR imaging has revealed the anatomic correlates of these clinical features. Isolated lesions within the substantia nigra have, for example, been reported in association with Parkinsonian syndromes in both StLE (4) and JE (12), and focal bilateral involvement of the thalami may also result in extrapyramidal symptoms in JE (13). StLE has not been reported to cause thalamic injury that is detectable by MR imaging. MVE and JE, therefore, appear to have a greater relative propensity to involve the thalamus than do other related flaviviruses. This neurotropism presumably reflects the cell receptors by which these viruses gain entry to specific neurons and requires further study. Whether the MR findings presented herein are typical of severe MVE remains to be determined; however, neuroimaging in the present case clearly demonstrated bilateral thalamic injury and is consistent with the known clinical similarities between MVE and JE. Infection with these viruses has a higher mortality with more frequent and severe long-term neurologic sequelae than that resulting from infection with other members of the JE group (5, 11).
Symmetric involvement of the basal ganglia by infection is otherwise rare but has been described in other unrelated viral encephalitides, including HIV (14), in early Creutzfeldt-Jakob disease (15), and may also occur when cerebral metabolism is altered, for example, by ischemia in a setting of hypoxic encephalopathy or internal cerebral vein thrombosis, hypoglycemia, or osmotic myelinolysis (16). These disorders, however, do not predominantly involve the thalami, and, in the appropriate clinical setting, neuroimaging that demonstrates bilateral thalamic injury should suggest a presumptive diagnosis of a flavivirus infection while confirmatory tests are pending. In the present case, a diagnosis of MVE was made by polymerase chain reaction on day 8 of the illness, with seroconversion to MVE IgM and IgG occurring on days 8 and 22, respectively. Bilateral thalamic lesions were, however, apparent on CT scans by day 4 and MR images on day 5 of the illness, several days before diagnosis by conventional tests.
Conclusion
MVE may present as a severe encephalitic illness. MR findings suggestive of MVE and other flavivirus infections include striking bilateral and symmetrical thalamic involvement with hypointensity on T1-weighted images and hyperintensity on T2-weighted images. Similar changes may be seen in the red nucleus, substantia nigra, and cord and correlate with both the pathologic distribution of necroltyic and hemorrhagic lesions and with the known neurotopism of these viruses. In the appropriate clinical setting, these findings suggest a presumptive diagnosis of flavivirus infection.
References
- Received October 28, 2002.
- Accepted after revision December 19, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}