
Abstract
Summary: Two patients had acute left carotid rupture from radiation therapy-induced pseudoaneurysms, resulting in hemodynamic collapse. Because the patients were semicomatose and in shock, an immediate salvage procedure was needed. Location of the pseudoaneurysm at the skull base made surgical treatment less possible. Endovascular therapy was the treatment of choice. Preserving patency of the carotid artery was a desirable option. The successful use of a covered stent in the emergency treatment of massive epistaxis due to active bleeding from pseudoaneurysm in the petrous internal carotid artery (ICA) is described.
Saccular aneurysms of the petrous carotid artery are rare. Most of the aneurysms are pseudoaneurysms that are related to congenital, traumatic, mycotic, and inflammatory causes. Because of the location within the petrous bone, a direct surgical approach is difficult, if not impossible.
Case Reports
Case 1
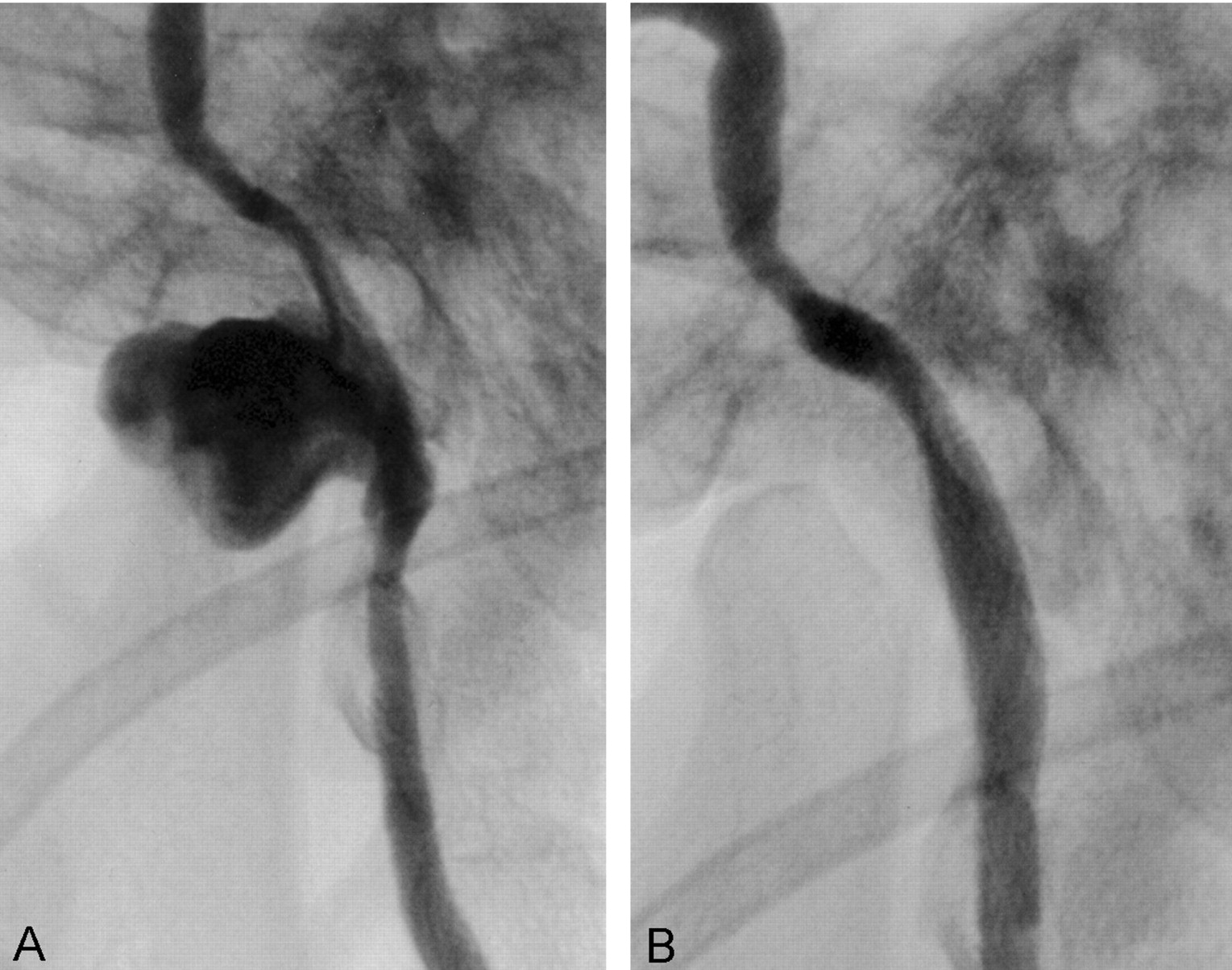
A 52-year-old Chinese woman had recurrent nasopharyngeal carcinoma treated with radiation therapy in 1981. She was found to have local recurrence and received radioactive gold grain brachytherapy in 1989. Her condition was complicated by right temporal lobe necrosis and osteoradionecrosis of the sphenoid and temporal bones. In July 2002, she presented with massive epistaxis that could not be stopped with nasal packing. Endoscopic examination found active oozing of blood from the nasopharynx. Initial emergency conventional angiography revealed some bleeding from both internal maxillary arteries. She developed shock and unconsciousness during the procedure. Therefore, bilateral external carotid artery ligation was performed, and hemodynamic stabilization was achieved. A total of 6 U of blood was given to the patient. However, epistaxis recurred the next day. Further angiography demonstrated a small pseudoaneurysm located at the petrous portion of the left ICA, with a small false sac demonstrated at its apex (Fig 1A). Although the nasopharynx was packed with an inflated balloon catheter, active oozing of blood was observed while the patient had unstable blood pressure and pulse. Without further delay, placement of a covered stent was performed with the patient under general anesthesia. A 7F femoral arterial sheath was placed over a guidewire. The patient did not have systemic hepariniziation since she was having massive bleeding. A 0.014-inch microguidewire was placed into the left ICA, with the distal end located at the left middle cerebral artery. A 4.0 × 20.0-mm Symbiot stent (Boston Scientific/Scimed, Maple Grove, MN) was then placed over the exchange wire under road-map guidance and was deployed across the corresponding segment with pseudoaneurysm. Abciximab (Reopro; Centocor, Malvern, PA) was given immediately before deploying the covered stent to prevent massive platelet aggregation and stent thrombosis. Follow-up angiography after the procedure revealed occlusion of the pseudoaneurysm (Fig 1B). The patient became hemodynamically stable and was discharged from the intensive care unit 1 day after the procedure. No recurrent hemorrhage was reported on follow-up for 6 months. No evidence of neurologic deficit was found.

Case 1.
A, Conventional angiogram shows a small pseudoaneurysm in the distal portion of the left ICA. The pseudoaneurysm points inferomedially.
B, Follow-up angiogram after stent placement depicts patency of the artery, with no evidence of pseudoaneurym
Case 2
A 52-year-old Chinese man had nasopharyngeal carcinoma, with radiation therapy performed in December 2001. He was found to have residual disease after radiation therapy. Stereotactic radiosurgery was performed because of the nasopharyngeal tumor in May 2002. In August 2002, he was admitted to the hospital because of epistaxis. Nasoendoscopy revealed bleeding from the nasopharynx. He presented with severe epistaxis and hemorrhagic shock. A brief cardiac arrest was recovered by resuscitation. CT angiography showed a 1.5-cm left ICA pseudoaneurysm pointing medially to the nasopharynx. He again developed a brief cardiac arrest in the CT suite after sudden profuse bleeding from the mouth. An emergent angiogram disclosed a large pseudoaneurysm at the petrous portion of the left ICA (Fig 2A). Since the patient was hemodynamically unstable, the decision was made to perform placement of a covered stent. A similar procedure to that in case 1 was performed, except this patient was given aspirin and clopidogrel before the procedure to avoid massive platelet aggregation. A 4.0 × 45.0-mm Symbiot covered stent was inserted to cover the neck of the psuedoaneurysm. Follow-up angiography after the procedure confirmed total obliteration of the psuedoaneurysm (Fig 2B). The patient was hemodynamically stable after stent placement. No further hemorrhage was noted. Three-month follow-up CT angiography showed patency of the left ICA with no pseudoaneurysm depicted (Fig 3A). No sign of infarct was identified at the left cerebral hemisphere. However, a portion of the left ICA with stent was exposed to the nasopharynx without being covered by any nasopharyngeal soft tissue (Fig 3B).

Case 2.
A, Conventional angiogram with left ICA injection demonstrates a large pseudoaneurysm in the petrous portion of the ICA.
B, Follow-up angiogram after stent placement shows total isolation of the pseudoaneurysm and patency of the ICA

Case 2 (3-month follow-up).
A, Follow-up oblique sagittal reformation of a CT angiogram of the neck depicts patency of the portion of the left ICA with stent, with no evidence of pseudoaneurysm.
B, Follow-up axial CT scan shows that some portion of the ICA with stent is exposed to the nasopharynx.
Discussion
Treatment of a pseudoaneurysm in the petrous carotid artery includes either sacrifice or preservation of the carotid artery. Sacrifice of the carotid artery would lead to severe cerebrovascular events, and therefore a balloon occlusion test should be performed in advance. If a temporary occlusion test is successful, trapping or parent artery occlusion is an option. If the patient cannot tolerate the test, bypass extracranial-to-intracranial surgery should be contemplated. However, preserving patency of the carotid artery as far as possible is a more desirable goal. Some reports have revealed cerebral aneurysm formation or growth after permanent carotid occlusion (1–3). Furthermore, 5–22% of patients passing the balloon occlusion test developed ischemic complications, including cerebral infarct (4–6). Our patients were semicomatose and in a state of cardiovascular collapse. The balloon occlusive test was not possible or reliable. A quick therapeutic procedure is essential in emergency situations.
There are several methods of preserving the carotid artery. The choice of endovascular carotid stent placement combined with Guglielmi detachable coils (GDCs) has been advocated (7, 8). However, pseudoaneurysm differs from other aneurysms because there is no true wall. The surrounding osteonecrotic bone cannot offer enough support to the artery and pseudoaneurysm. We had an experience of successful treatment of a radiation therapy-induced pseudoaneurysm by using stent-assisted GDC embolization (unpublished data). Although initially the pseudoaneurym was totally obliterated, progressive enlargement was noted on follow-up images. This occurred because the postradiation arterial wall was weakened; also there was a lack of support from the surrounding osteonecrotic bone. Eventually, a new and larger pseudoaneurysm developed. Furthermore, the GDCs in the pseudoaneurysm could be visualized with otoscopy. Future migration or infection of the coils would be possible in the exposed metallic stent and GDCs. In our second case, the follow-up CT scan depicted exposure of a portion of the left ICA with stent to the nasopharynx. The GDC coiling technique was not possible because the GDCs could not be held or contained locally by the soft tissue or bone. In view of the pitfall of a stent-assisted GDC coiling technique, we found placement of a covered stent especially useful in this kind of pseudoaneurysm. However, in another report, a double-stent technique was used to promote stasis by placing two balloon-expandable stents over each other (9). This has proved effective in promoting stasis within the pseudoaneurysm. This technique, however, may increase the risk of delayed stenosis.
Because our first patient was hemodynamically in shock with active oozing of blood even though the nasopharynx was packed with an inflated balloon, an immediate salvage procedure was essential. There was not enough time for antiplatelet treatment. To avoid malignant platelet aggregation, abciximab was given just before deploying the covered stent. In the second patient, however, the bleeding from the nasopharynx was temporilary controlled. The antiplatelet agent, aspirin and clopidogrel, could be given well before the stent placement procedure. Although no acute massive platelet aggregation occurred in either case, we prefer to administer an antiplatelet agent before the stent placement procedure. Our usual practice is clopidogrel 75 mg four times (ie, total dose 300 mg) before the stent placement procedure.
Covered stents or stent-grafts have been used in the treatment of aortic aneurysms (abdominal or thoracic aorta), lacerations, dissections, or arteriovenous fistulas. Stent-grafts reportedly have been used in the popliteal artery, subclavian and brachial arteries, iliac and femoral arteries, abdominal aorta, and even extracranial carotid artery (10–20). The Symbiot stent is a small, nitinol, self-expandable, flexible stent that is covered on both the luminal and abluminal sides with a highly porous polytetrafluoroethylene. The stent was designed for vascular use in coronary saphenous vein grafts and is very flexible so that it is ideal for intracranial vascular application. The internal and external lining could exclude blood flow through the stent. In addition, it may also serve as a physical barrier to prevent late neointimal proliferation and restenosis, and it may decrease embolization during stent deployment by trapping debris that otherwise would have been extruded through the stent struts (21, 22). The available lengths consist of 20, 31, and 45 mm. The stent placement procedure is safe and quick. We completed the procedure in less than 1½ hours. The immediate exclusion of the pseudoaneurysm led to arrest of arterial bleeding and instant stabilization of the patient’s blood pressure and pulse. The covered stent has advantages in the treatment of pseudoaneurysm, especially in cases of pseudoaneurysms that lack surrounding support. However, no data concerning long-term patency of the covered stent are yet available. The covered stent may occlude the arterial branches from the artery, whereas porous stents can maintain the patency of branches. Since there are few arterial branches originating from the petrous ICA, the covered stent is deemed to be more useful as compared with its use in other portions of the ICA that have major branches or perforating branches. In our second case, the covered stent was exposed to the nasopharynx with no soft tissue or bony coverage. Even though the covered stent successfully isolated the ICA from massive bleeding, infection or mechanical damage of the covered stent would be possible in the future. Furthermore, the rate of thrombosis of the stent could be higher. Closer follow-up of the second patient is very important.
Conclusion
Two patients with radiation therapy-induced psuedoaneurysm in the petrous carotid artery underwent successful implantation of a covered stent on an emergency basis, with complete obliteration of the aneurysm and alleviation of symptoms. Although long-term follow-up and larger samples are required for evaluating the efficacy, we demonstrated the usefulness and versatility of placement of a covered stent in the rapid treatment of carotid arterial pseudoaneurysms. The stent placement procedure is quick, safe, feasible, and less invasive for maintaining vessel patency while effectively isolating the pseudoaneurysm.
References
- Received January 28, 2003.
- Accepted after revision February 18, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular management of intracranial carotid blowout syndrome in patients with head and neck cancer
- A rare but morbid neurosurgical target: petrous aneurysms and their endovascular management in the stent/flow diverter era
- Primary endovascular treatment of post-irradiated carotid pseudoaneurysm at the skull base with the Pipeline embolization device
- Cervical-petrous internal carotid artery pseudoaneurysm presenting with otorrhagia treated with endovascular techniques
- Cervical-petrous internal carotid artery pseudoaneurysm presenting with otorrhagia treated with endovascular techniques
- Pipeline embolization device and subsequent vessel sacrifice for treatment of a bleeding carotid pseudoaneurysm at the skull base: a case report