Abstract
BACKGROUND AND PURPOSE: Endovascular treatment with detachable coils is an accepted alternative to surgical clip placement for intracranial aneurysms. The purpose of this study was to evaluate the safety and reliability of the Sapphire coil, a new platinum coil for the treatment of intracranial aneurysms.
METHODS: Between August and September 2003, 20 consecutive patients (13 women, seven men; mean age, 49 years; range, 33–77 years) with 20 intracranial aneurysms were referred to our department for endovascular treatment. Fifteen patients presented with subarachnoid hemorrhage, whereas five had asymptomatic, unruptured aneurysms. All patients were treated by selective endosaccular coil placement with the new coils. The remodeling technique was used in five wide-neck aneurysms. Clinical outcomes were assessed with the modified Glasgow Outcome Scale.
RESULTS: Aneurysmal occlusion with the new coils alone was successful in 16 patients and resulted in 12 complete occlusions and four neck remnants. Because of the limited Sapphire product line, additional Guglielmi detachable coils (GDCs) were required in four patients, two of whom received one 3D GDC of 3 mm diameter and two of whom received Ultra-Soft GDCs. Technical complication (stretching of a coil) occurred in one patient. Clinical outcomes were excellent in 14 patients and good in two.
CONCLUSION: Although the study was limited by its small patient population, the results show that selective endovascular treatment of intracranial aneurysms with Sapphire coils was not associated with an unexpected incidence of adverse events. Excellent anatomic and clinical results that were obtained in most patients suggest that Sapphire coils may have value in the treatment of intracranial aneurysms.
During the past decade, endovascular treatment has gained acceptance as a therapeutic alternative in the care of patients with intracranial aneurysms (1). Detachable balloons (2) and nondetachable coils (3) have been widely used, but they are associated with a relatively high complication rate. With the development of the first controlled-detachable coil (4), the indications for treating intracranial aneurysms have changed. Several detachable coils are now available; their detachment is electrically or mechanically controlled (5, 6). Sapphire coils (Micro Therapeutics, Irvine, CA) are newly designed coils with interesting features: the variable detachable system (VDS) that allows the detachment of coils at variable lengths (7, 8), a short detachment time, and 3D coils are useful to create a basket in the aneurysm with the first coil. We prospectively assessed the immediate angiographic and clinical results in 20 patients with an intracranial aneurysm treated by means of selective embolization with Sapphire coils.
Methods
Population
Between August and September 2003, 20 consecutive patients with an intracranial aneurysm were referred to our department for endovascular treatment. As shown in the Table, they included 13 women and seven men, with a mean age of 49 years (range, 33–77 years). Fifteen patients presented with SAH and were classified according to the Hunt and Hess scale (9): 11 patients had a grade of I or II SAH; two, grade III; and two, grade IV. In five patients, the aneurysm was asymptomatic. Aneurysms were located in the anterior circulation in 17 patients and in the posterior circulation in three. All aneurysms were smaller than 12 mm; five had an unfavorable neck size (>4 mm) or neck-to-sac ratio (>0.7). All patients underwent conventional angiography of both carotid arteries and vertebral arteries. The neurosurgical and neurointerventional teams discussed the therapeutic alternatives.
Endovascular treatment of 20 intracranial aneurysms in 20 patients
Sapphire Detachable Coils
The Sapphire detachable coil consists of an embolization coil made of a platinum alloy attached to a stainless steel guiding system with a radiopaque positioning coil. It is designed for use with the Sapphire detachment system. These coils are available in both 3D (Sapphire Atlas 3D coil; Micro Therapeutics) and helical shapes (Sapphire Helix Standard and Soft coil, Sapphire VDS coil, Sapphire Tension Safe coil, Sapphire Multi-Diameter, and Sapphire Curved Tip; Micro Therapeutics). The Atlas 3D coil has a 3D structure that forms a spherical cage of loops within the aneurysmal sac. All sizes from 4 to 18 mm are presently available. The Tension Safe coil is a helical coil braided with a nitinol filament that reduces the risk of stretching during repositioning. The Multi-Diameter coil is a helical coil that presents a decrease in coil diameter along its length, allowing for better compaction. The VDS coil (Fig 1) is the first coil with multiple detachment sites along its length. It is currently available in two sizes with 3- and 4-mm diameters; both are 12 cm long with four detachable segments. Each detachment site measures 300 μ and is clearly visible with good-quality fluoroscopy. All coils are provided mounted and ready for introduction.

Schematic drawing of a VDS coil.
Endovascular Procedure
Endovascular treatment was performed with all patients under general anesthesia and systemic heparinization. The adequacy of systemic anticoagulation was monitored by using frequent measurements of the activated clotting time (ACT). A baseline ACT was obtained before a bolus injection of heparin (50–75 IU/kg body weight) and hourly thereafter. This was followed by a continuous infusion (1000–1500 IU/h) with the purpose of doubling the baseline ACT. In most patients, systemic heparinization was stopped at the end of the procedure. In case of wide-necked aneurysms or periprocedural complications, systemic heparinization was prolonged for 48–72 hours.
All patients were treated by means of selective embolization with Sapphire coils: 3D coils were initially delivered in the aneurysmal sac to obtain a good basket, and then helical coils (Helix Soft, Tension Safe, and/or VDS coils) were placed to obtain dense packing. VDS coils were mostly used at the end of the procedure to assess the reliability of the variable detachment systems. In all cases, we used a microcatheter (Excelsior 10 or 18; Target Therapeutics, Fremont, CA) to deliver the coils into the aneurysm. In five cases with an unfavorable neck-to-sac ratio, the remodeling technique (10) was used to avoid coil protrusion into the parent artery. Failure of endovascular treatment was defined as the inability to completely occlude the aneurysm with Sapphire coils alone. In these cases, GDCs were used to complete aneurysmal obliteration. After endovascular treatment, patients were transferred to the intensive care unit; their fluid balance, neurologic status, and blood pressure were carefully monitored.
Immediate Outcomes
Patients were evaluated by means of angiography to document aneurysmal obliteration. Angiographic results were classified as complete occlusion (no contrast agent filling the aneurysmal sac), a neck remnant (residual contrast agent filling the aneurysmal neck), and residual flow (residual contrast agent filling the body of the aneurysm). A senior neurosurgeon (J.P.L.) recorded the patient’s clinical course, including worsening of symptoms and death. Clinical outcome was graded according to a modified Glasgow Outcome Scale (GOS) (11), as follows: Excellent indicated neurologically intact. Good was mild hemiparesis, cranial nerve palsy, or other deficit that did not interfere with daily functioning or work. Fair was substantial hemiparesis, aphasia, confusion, or other deficit that interfered with daily activities or prevented a return to work. Poor indicated coma or severe neurologic deficit rendering the patient dependent on his or her family or nursing staff. Two senior neuroradiologists (B.L., X.L.) together reviewed the conventional angiographic findings in all patients.
Results
Illustrative Cases
A 54-year-old man (patient 8) complained of headaches and underwent brain imaging. An unruptured aneurysm of the MCA bifurcation was discovered on the left side, and the patient was referred to our department for endovascular treatment. Conventional angiography (Fig 2A) revealed a wide-necked aneurysm involving a branch of the MCA bifurcation. The patient was treated with the balloon-assisted technique (10). A 4 × 7 mm Hyperform balloon (Micro Therapeutics, Irvine, CA) was placed in the involved branch to protect the artery and seal the aneurysmal neck (Fig 2B and C). Five Sapphire coils were delivered in the aneurysmal lumen, including one 3D coil, two Helix Soft coils, and two Tension Safe coils. Conventional angiography (Fig 2D) at the end of the procedure showed complete aneurysmal occlusion. The patient had transient ischemic attacks 6 hours after treatment and received heparinization for 72 hours. He made an excellent recovery and was discharged home 5 days after treatment.

Incidental aneurysm discovered at MR imaging and MR angiography in a 54-year-old man with headaches.
A, Left ICA angiogram shows a wide-necked MCA aneurysm involving a branch of the bifurcation.
B, Nonsubtracted angiogram shows the placement of a Hyperform balloon microcatheter in the involved branch.
C, Control angiogram obtained during coil deployment shows the balloon protecting the branch and bulging into the MCA bifurcation to optimally seal the neck.
D, Control angiogram obtained immediately after treatment shows complete occlusion of the aneurysm and patency of the MCA bifurcation branches.
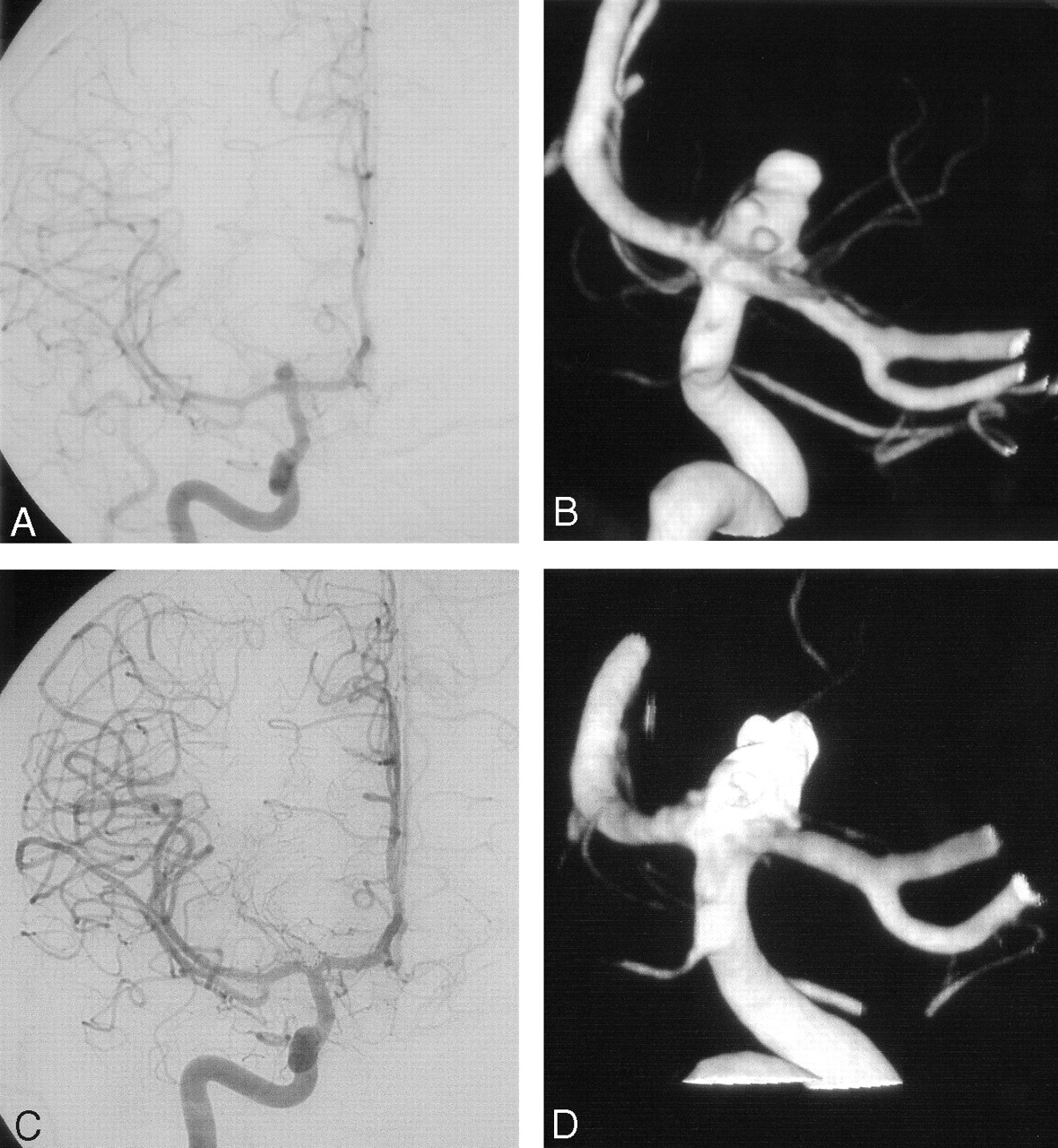
A 33–year-old woman (patient 2) presented with an emergency grade II (9) SAH. Cerebral angiography showed a ruptured ICA bifurcation aneurysm (Fig 3A and B). The patient was treated by means of selective embolization with five Sapphire coils, including two 3D coils, and three Tension Safe coils. Control angiograms obtained at the end of the procedure (Fig 3C and D) showed complete aneurysmal occlusion. Results of clinical examination remained unchanged, and the outcome was excellent.

{kind=link}
{kind=link}
{kind=link}
SAH in a 33-year-old woman.
A and B, Conventional (A) and 3D (B) angiograms of the right ICA obtained before treatment show an ICA bifurcation aneurysm with multiple daughter sacs.
C and D, Conventional (C) and 3D (D) control angiograms obtained after selective embolization with Sapphire coils show complete occlusion of the aneurysm, with the coils filling the daughter sacs.
Reliability of the Material
Endovascular treatment with Sapphire coils alone was successful in 16 patients. In four patients (patients 5, 6, 18, and 19), additional GDCs were required: One 3D GDC of 3-mm diameter was needed to create a good basket in two patients, and one Ultra-Soft GDC was required to occlude the aneurysmal neck at the end of the procedure in two patients. Endovascular treatment with Sapphire coils failed in these patients (20%).
A total of 101 Sapphire coils (31 3D coils, 48 Tension Safe coils, 15 Helix Soft coils, and seven VDS coils) were used and easily passed through the microcatheter in most cases. However, 11 coils (11%)—including nine 2-mm, 8-cm Tension Safe coils—could not be delivered because of high friction within the microcatheter. In all aneurysms, one to five 3D coils were initially placed to obtain a good basket. During the delivery process, 3D coils adapted smoothly to the aneurysmal wall without any tendency to move in a tumbling manner. These coils automatically assumed their spherical configuration upon their deployment. Helical coils were added and densely packed the aneurysms without any compartmentalization. All VDS coils could be used and delivered at the desired length. The detachment of all coils occurred in less than 60 seconds, and no absence or premature detachment was observed. In five cases of wide-necked aneurysms treated with the remodeling technique (10), all Sapphire coils were easily placed during balloon inflation. Technical complications occurred in only one patient (patient 3), without any clinical modification. In this 57-year-old man with a ruptured aneurysm of the AcomA, stretching of the last coil was observed during repositioning.
Immediate Angiographic and Clinical Outcomes
In 16 patients, endovascular treatment with Sapphire coils alone resulted in 12 complete occlusions and four neck remnants. Modified GOS scores (11) were excellent in 14 patients and good in two. Patients 11 and 17 with grade IV SAH had hemiparesis despite uneventful and effective endovascular treatment. Patients 3 and 8 had procedure-related complications, including stretching of the last coil in one, and periprocedural transient ischemic attack in one. These patients had presented with an aneurysm of the AcomA or a wide-necked MCA bifurcation aneurysm. Heparinization was maintained for 72 hours in both patients, and they made excellent recoveries.
Discussion
This study shows that Sapphire coils may have value in the endovascular treatment of ruptured and unruptured intracranial aneurysms. Since the introduction of the first controlled-detachable coil (4), the indications for treatment of intracranial aneurysms have enlarged, and several detachable coils systems with mechanical or electrolytic detachment mechanisms are currently available (5, 6). Sapphire coils are newly designed coils with interesting features, including the VDS, a short detachment time, and 3D shapes. Our series showed the reliability and efficacy of these specific properties. VDS coils (7, 8) are the first coils that can be detached at multiple points along their length; these were mostly used at the end of endovascular treatment. When the aneurysmal sac is nearly occluded, the length of the last coil required for complete occlusion may be difficult to estimate. In this situation, VDS coils are helpful for safely occluding the neck remnant. Furthermore, the aneurysm is engaged fewer times; this feature might reduce procedural time and the risk of rupture, and it appears to be a real advantage over other available systems. However, Thammaroj et al (8) reported procedural difficulties with VDS coils in the treatment of small aneurysms because of their stiffness. In our series, VDS coils were delivered at the end of the procedure, and we did not have notable difficulty in deploying them. In all cases, VDS coils could be detached at the desired length to prevent technical difficulties. According to the manufacturer, the technology is evolving, and a new, less-stiff VDS coil (Tension Safe; Micro Therapeutics) will soon be available.
The detachment time for all Sapphire coils was less than 60 seconds and did not increase with progressive coil deployment. Sapphire 3D coils allowed us to create a good basket inside the aneurysm, helping to fill it with helical coils and to obtain dense packing. However, the size of the aneurysmal neck may be a limitation because of coil protrusion into the parent artery. With the development of new tools, including remodeling balloons (10), and bridging-neck devices (eg, stents), most wide-neck aneurysms are now amenable to endovascular treatment (10, 12). In the present study, the remodeling technique with Sapphire coils proved to be effective in wide-necked aneurysms.
Some technical limitations were encountered in this study. For instance, 11% of the coils could not be delivered because of high friction within the microcatheter, and 20% of patients (n = 4) could not be completely treated with Sapphire coils alone. The nondelivered coils were 2-mm, 8-cm Tension Safe coils in nine cases. This problem did not affect the remaining Sapphire product line. In the four patients (patients 5, 6, 18, and 19) who required additional GDCs to complete embolization, one 3D GDC of 3-mm diameter was used in two cases, and one Ultra-Soft GDC was used in two. These patients presented with aneurysms that could not be safely treated without a 3-mm 3D coil at the beginning to bridge the aneurysm neck or without very soft coils at the end to complete treatment. Therefore, limiting characteristics of the Sapphire coils include the lack of a 3-mm 3D coil and very soft coils.
No procedure-related morbidity or mortality was observed in the 16 treated patients, and immediate anatomic and clinical results were good or excellent in all patients.
Conclusion
To our knowledge, our study is the first reported series of intracranial aneurysms treated by selective embolization with Sapphire coils. Although the patient population was small, the results suggest that Sapphire coils may have value in the endovascular treatment of intracranial aneurysms. Despite a still-limited product line, the VDS of Sapphire coil seems to offer a potential advantage over other systems.
References
- Received October 27, 2003.
- Accepted after revision January 15, 2004.
- Copyright © American Society of Neuroradiology