
Abstract
BACKGROUND AND PURPOSE: Vertebroplasty is rapidly disseminating as a treatment for vertebral compression fractures, but its efficacy has not been assessed with a well-validated, back pain–specific instrument. We report the use of the Roland-Morris Disability Questionnaire (RDQ) in patients undergoing vertebroplasty for painful osteoporotic compression fractures.
METHODS: Retrospective review of patients treated with vertebroplasty who completed the RDQ and 2 verbal pain scales (0–10) for pain at rest and pain with activity at baseline, 1 week, 1 month, 6 months, and 1 year post-vertebroplasty. Changes in outcome measures were analyzed by using a paired t test and correlations were assessed with Spearman ρ. Multiple linear regression was used to analyze the relationship between baseline scores and independent variables.
RESULTS: One hundred thirteen patients were treated at 164 vertebral levels. At baseline, RDQ scores were associated with rest and activity pain (P < .001 and P = .002, respectively) but were not associated with other independent variables. All 3 outcome scores decreased by 1 week and remained improved through maximal follow-up (P < .001). RDQ scores improved by a mean of 7.0 points at 1 week and remained improved at 1 year (P = .02). RDQ scores correlated with both rest and activity pain, but the absolute correlation was slightly better (+0.15 on average) with activity pain.
CONCLUSIONS: Patients who underwent vertebroplasty experienced relief of back pain and symptoms, as shown by improvement in verbal pain and RDQ scores. The RDQ correlates well with measures of pain, shows clinically significant improvement and is responsive to changes across time. More important, the RDQ provides an easily administered, well-validated, back pain–specific outcome measure that could be adopted to assess vertebroplasty outcomes.
First used in the United States in the 1990s, vertebroplasty has rapidly approached standard of care for treatment of medically refractory, painful vertebral compression fractures. Because of difficulties in study design and execution there have been no randomized, blinded, controlled studies comparing vertebroplasty to placebo or conservative therapies. Instead, investigators have sought to validate use of the procedure through changes in measures of perceived pain. These studies have shown significant improvement in pain and other symptoms as assessed by these instruments (1–3). There is no continuity, however, in the type of instrument used or the symptom variables that have been assessed in the vertebroplasty literature.
A critical review of the vertebroplasty literature reveals that, to this point, there exists a dearth of studies that have used validated outcome measures to assess the efficacy of this treatment. Visual analog scoring of perceived pain is the most common method of assessment. Although this addresses the patient’s pain and provides a well-validated variable for assessment of pain control (4), this instrument fails to address the other symptoms and disabilities experienced by the patient. Because vertebroplasty aims at improving both the pain and disability experienced by the patient, both of these elements should be included in outcome measures when determining treatment efficacy.
We report the application of a widely applied, back pain–specific, well-validated outcomes instrument, the Roland-Morris Disability Questionnaire (RDQ), to a consecutive cohort of patients undergoing vertebroplasty for the treatment of painful, osteoporotic compression fractures. In addition, we correlated the RDQ with 2 11-point graded pain scales and tracked these measures across time. We believe that the RDQ should be used as the primary outcome measure for vertebroplasty research and practice.
Methods
We performed a retrospective review of 113 patients who underwent vertebroplasty between April 21, 2003, and September 27, 2004, at our institution. Institutional review board approval was obtained for this study. Vertebroplasty typically was offered to patients with radiologic evidence of acute or subacute vertebral compression fractures of thoracic or lumbar vertebrae. Exclusion criteria included improvement with conservative management, technical contraindications, and noncorrelating pain. Patients included in this study were limited to those with compression fractures due to underlying osteoporosis.
Vertebroplasty Procedure
Vertebroplasties were performed by staff radiologists according to the methods outlined previously (5). Specifically, patients were treated by using intravenous conscious sedation. Biplane fluoroscopy was used in all cases. Local anesthesia was administered over the skin, subcutaneous tissues, muscular tissues, and periosteum of the targeted pedicle. Transpediculate or parapedicular trajectories were used in all cases. After local anesthetic administration, 11- or 14-gauge biopsy needles (Cook Inc., Bloomington, IN) were advanced into the central aspect of the vertebral bodies for unipediculate approaches, whereas placement of the needle was made into the midportion of the hemivertebra for bipediculate approaches.
The polymethylmethacrylate (PMMA) cement mixture was prepared under a vacuum hood. Approximately 30 g of PMMA powder (Codman Cranioplastic, Raynham, MA) was mixed with 12 g sterile barium sulfate (Cardinal Health, McGaw Park, IL) and 1 g gentamicin powder (Hawkins Inc., Minneapolis, MN). Liquid PMMA monomer was mixed with the powder mixture until the fluid reached a viscosity similar to that of cake glaze. The mixture was then loaded either into an injector device (Cook Inc.) or into 1-mL syringes and injected under continuous lateral and intermittent AP fluoroscopy. Cement injection was considered complete when the cement reached the posterior fourth of the vertebral body on the lateral projection. Injection was also terminated when epidural, venous, or transendplate extravasation was noted. Following needle removal, patients were left on strict bed rest for 1 hour and then discharged.
A maximum of 4 vertebral levels were treated in a single session based on clinician comfort levels. Additional levels were treated in repeat sessions as required.
Outcome Measures
The RDQ (appendix 1) and 2 verbal scales (scored 0–10) to assess “pain at rest” and “pain with activity” were administered in person by trained nurses at the time of evaluation for vertebroplasty. The original RDQ contained 24 questions and was derived from statements contained in the Sickness Impact Profile (6). Each question was selected on the basis of its likelihood of being influenced by back pain and the qualification “because of my back pain” was added to further target the responses (7). The modified RDQ used in this study is that proposed by Patrick et al (8) and contains 23 yes/no questions. Nineteen of these 23 items are taken from the original RDQ, and 4 were derived from other statements in the Sickness Impact Profile (8). These modifications were suggested by the authors in an effort to reduce redundancy and add in items that were previously shown to better reflect changes in patient condition (8). The modified instrument takes approximately 3 minutes to complete and can be self-administered or administered via the telephone. It is scored from 0 to 23 on the basis of the number of “yes” responses. The authors have demonstrated that the modified version had a high level of internal consistency, construct validity, and responsiveness (8).
Follow-up data for all 3 outcome scales were gathered by telephone by the same trained nurses at 1 week, 1 month, 6 months, and 1 year post-vertebroplasty. Patients who were telephoned 3 times, without successfully obtaining follow-up data, were designated as nonrespondents for that time period. Nonrespondent status at a given time point did not preclude contacting that patient at the next designated time point.
Statistical Analysis
Changes in pain scores across time were analyzed by using a paired t test comparison to the preceding time point. Correlation between outcome measures was assessed with the Spearman ρ correlation coefficient and differences in the strength of correlation were assessed through statistical bootstrapping of the data. Multiple linear regression was used to analyze the relationship between outcome scores and independent variables (age, sex, lumbar versus thoracic treatment, number of levels treated) at baseline and 1 week.
Results
Data were collected from 113 patients who underwent vertebroplasty at 164 vertebral levels. Compression fractures in this population were all osteoporotic in origin. The mean patient age at the time of the procedure was 74 years (range, 28–96 years). Ninety (80%) of the 113 patients were women. As of this study, 113 patients were immediately post-vertebroplasty, 108 (96%) patients 1 week post-vertebroplasty, 93 (82%) patients 1 month post-vertebroplasty, 52 (46%) patients 6 months post-vertebroplasty, and 19 (17%) patients 1 year post-vertebroplasty. RDQ scores were available for 108 (96%) patients at baseline, 93 (86%) patients at 1 week, 73 (79%) patients at 1 month, 46 (89%) patients at 6 months, and 15 (79%) patients at 1 year. Four patients were excluded at 1 year because of secondary injury or processes that may have skewed their RDQ scores. Three of the excluded patients had falls resulting in pelvic fractures in one and new vertebral fractures in another. The fourth patient was excluded because of a subsequent diagnosis of fibromyalgia as the cause of her pain.
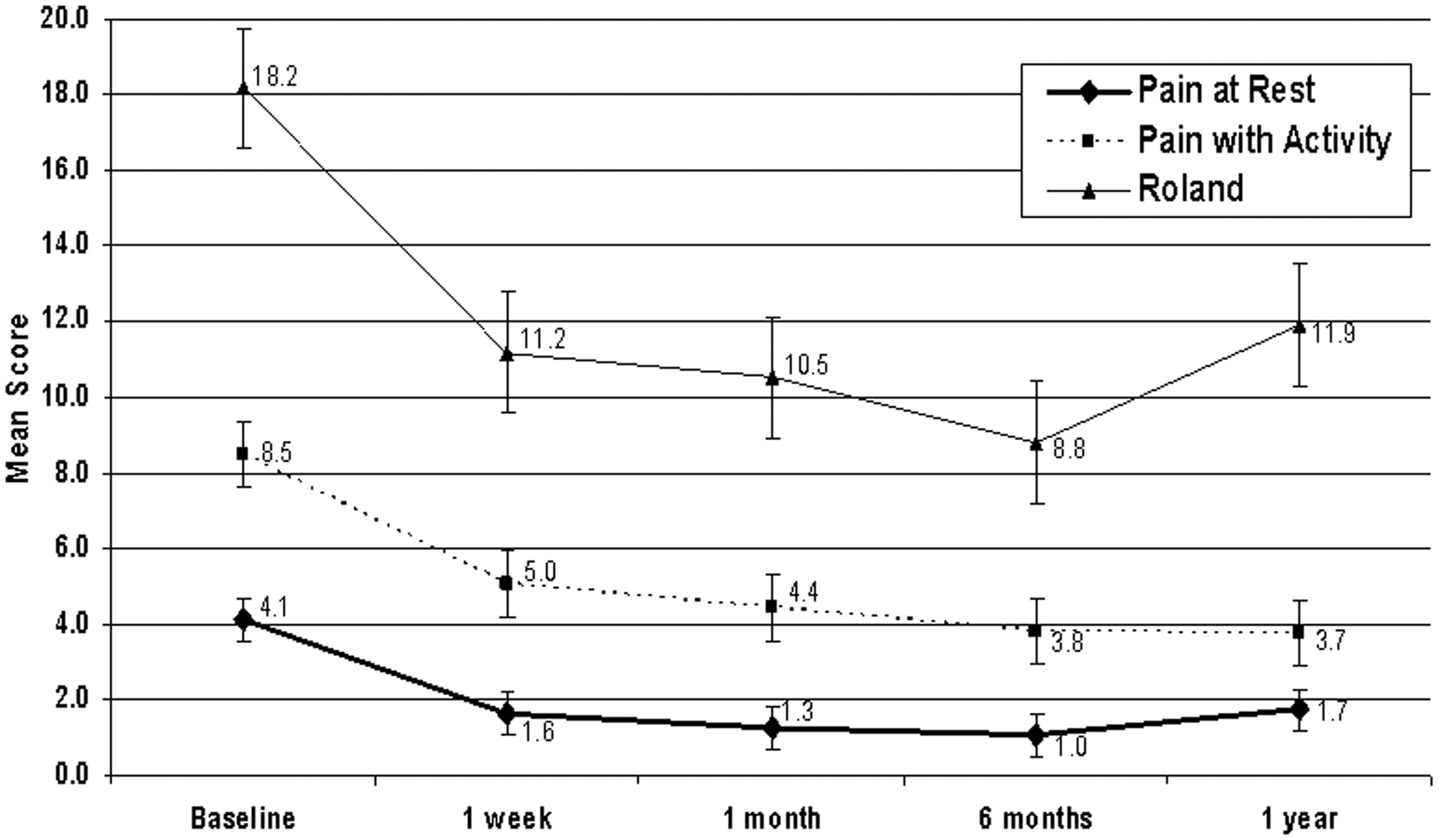
All 3 outcome measures (rest pain, activity pain, and RDQ score) showed a significant decrease at 1 week (P < .001), with RDQ scores improving by a mean of 7.0 points. These improvements in all 3 outcome measures persisted through 1-year follow-up (Fig 1). Absolute values continued to decline at each time point, but the changes between time points were not statistically significant. There was a statistically significant increase in RDQ scores at 1 year (P = .003), but the score remained significantly improved over that at baseline (P = .02).

Mean RDQ and pain scores, with SDs, across follow-up. There is significant improvement in all 3 outcome measures at 1 week that persists throughout follow-up.
RDQ scores correlated with both rest pain and activity pain at all time points (Table 1). On average, the correlation between RDQ scores and activity pain scores was +.15 better than that with rest pain scores. This difference approached but did not reach statistical significance (P = .07).
Correlation between Roland score and pain scales at each time point throughout follow-up
Multiple linear regression analysis of outcome measures showed an association between baseline RDQ scores and baseline activity pain and rest pain (P < .001 and P = .002, respectively) but showed no significant correlation with other patient or procedural variables (Table 2). Scores at 1 week were not found to be associated with baseline scores or any of the other variables.
Linear regression of baseline Roland and pain with activity scores
Discussion
Although vertebroplasty is rapidly disseminating as a treatment for vertebral compression fractures, the evidence for efficacy is weighed largely on symptomatic improvement in perceived pain from case series. Although pain control is an important element of vertebroplasty, the procedure is also designed to reduce disability in the treated individual. Few investigations have used validated outcome measures to address the impact of vertebroplasty on patient disability.
In the current study, we applied the RDQ to the practice of vertebroplasty. We selected the RDQ because it fulfills criteria that are important for outcome measures used to evaluate the efficacy of vertebroplasty: (1) back pain-specific measurement; (2) well validated in the literature; and (3) easily administered by telephone to elderly patients. The RDQ was specifically designed to assess physical disability due to lower back pain (6). In addition, this instrument was determined to be reliable and well validated when it was initially proposed and has been validated in many studies since that time (7, 9).
We showed substantial improvement in RDQ scores that persisted with time. Mean improvements were on the order of 7–9 points at all follow-up intervals. This level of improvement far exceeds the change of 2–3 points that is considered clinically important by the authors of the instrument (7). Further, we showed that RDQ scores correlate with the well-established 11-point verbal pain scales frequently used in the literature. Both RDQ scores and pain scale measurements improved significantly at 1 week and remained improved over baseline through 1-year follow-up. Last, we found the RDQ instrument to be highly user-friendly, generating acceptable response rates and facilitating telephone follow-up with vertebroplasty patients. These findings are relevant because they show that the RDQ is well suited to measure vertebroplasty outcomes as it is both sensitive to change across time and correlates well with the patient’s level of pain and disability.
Previous authors have applied a variety of validated outcomes scales to vertebroplasty and have shown improvement in measured disability and symptoms (Table 3). With the exception of the Oswestry Low Back Pain Disability Questionnaire (ODI), however, these instruments do not focus on the most relevant criteria in tracking outcomes in vertebroplasty patients. Back pain specificity is the most important of these criteria. Many of the patients who receive vertebroplasty have coincident health problems that influence their overall level of health and functioning. Back pain and symptom data that are gathered through global health measures are likely confounded by the influence of other health conditions on these assessments.
Results of previous outcome measure studies
The SF-36, McGill Mezlack questionnaire, and Nottingham Health Profile were designed as generic measurements of health and are not specific to back pain (10–12). It is important to note that the RDQ shows more responsiveness to change than the SF-36 and thus may be more useful in assessing outcomes (13). Also the McGill Mezlack questionnaire is more complex than other instruments both to administer and to score.
The ODI might be considered to be the most appropriate instrument that has been previously used in the literature to assess outcomes after vertebroplasty. This instrument was specifically designed to describe back pain and disability and has been found to be both reliable and valid (7). It has also been effectively administered in person and by telephone. The only study in the literature to use the ODI in vertebroplasty outcomes assessment is the study by Winking et al (14), which enrolled 38 patients and tracked their outcomes for 1 year. The authors showed a significant decrease in ODI score 2 days postvertebroplasty that persisted unchanged to 6 weeks. Although ODI scores were tracked out to 1 year, statistics were only given on these data out to 6 weeks, and thus the authors could not comment on long-term outcomes.
Comparisons of the RDQ to the ODI have shown small but important differences. Stratford et al (9) found an increased rate of incomplete responses with the ODI when compared with the RDQ. This may be inherent in the instrument or may reflect the fact that the ODI has more questions specific to “sex life,” “social life,” and “travel,” which may be less relevant in the day-to-day function of the elderly population. Regarding the applicability of the 2 instruments, Roland and Fairbank (7) concluded that the RDQ may be better suited to settings in which patients have mild to moderate disability that is expected to improve, whereas the ODI is suited to situations in which patients have persistent severe disability. These 2 conclusions lead us to believe that the RDQ is not only more appropriate in vertebroplasty patients who are expected to rapidly improve, but also may generate more complete responses and data.
In our practice, we have observed substantial clinical utility for the RDQ. Primarily, the RDQ is more useful than pain scores for assessment of the impact of vertebral fractures on the patient’s daily life. Pain scores are influenced by the patient’s perception and tolerance for pain and the reported value relates only loosely to functional limitation. The RDQ, however, gives care providers an objective assessment of the functional limitation suffered by the patient. This is useful both for the treating physician and for ancillary health staff. For the physician, thinking of RDQ scores in categories similar to those defined by Patrick et al (8)—10.8 = low; 15.7 = mild; 17.5 = moderate; 19.0 = severe—allows informal categorization of the severity of the patient’s impairment and provides some basis for treatment and management decisions. For ancillary health staff, specific limitations indicated in the RDQ can provide a basis for physical/occupational therapy or other directed lifestyle interventions. Finally, tracking both specific items on the RDQ and the RDQ score in general, allows effective monitoring of a patient’s progress following vertebroplasty.
Although our study is the first to apply the RDQ to vertebroplasty patients and the first to show long-term improvement in a validated, back pain–specific outcome measure, several substantial limitations remain. This study was both retrospective and lacking a control group. Ultimately, to validate the efficacy of vertebroplasty, prospective controlled studies are needed to show significant improvement over conservative management (15). Another potential limitation to this study is that follow-up was done by telephone. Although we felt that one of the characteristics of a good outcome measure was ease of telephone administration, other investigators argue that administering an instrument by telephone introduces a bias to the data (16, 17). This is a valid concern, but the increased response rates and the ability for fragile and significantly disabled patients to complete the instrument outweigh the potential bias. In addition, we took steps to minimize this bias by having designated vertebroplasty nurses administer the RDQ in person and by telephone according to a strict protocol. The low response rate at 1 year is also problematic, with only 17% of subjects achieving that duration of follow-up by the time of this study. On the basis of the small data set, the results for 1 year may be less reliable than those at earlier time points. Finally, a potential issue with our data collection is that our nonrespondents were not carefully tracked. For the purpose of outcomes data, it would be useful to differentiate between patients who were unwilling or unable to complete the instrument versus those who were simply lost to follow-up.
This study undertook to address an underlying deficiency in the vertebroplasty literature and demonstrate the use of a validated outcome measure. It provides useful and valid data about vertebroplasty outcomes but does not preclude the necessity to undertake additional prospective, controlled studies. If we are to draw larger conclusions across studies and populations, it is important that we standardize our outcome assessments.
Conclusion
Patients undergoing vertebroplasty for osteoporotic compression fractures had less pain and symptoms after the procedure. On the basis of background data and the results of this study, the RDQ appears well suited as a standardized measure of the efficacy of vertebroplasty. It is longitudinally validated and back pain–specific, and we have shown it to be effective in assessing outcomes following vertebroplasty. It is our assertion that the RDQ should be adopted as the outcome measure of choice to monitor the long-term efficacy of vertebroplasty.
Appendix 1
Modified RDQ (6, 8)
When your back hurts, you may find it difficult to do some of the things that you normally do. This list contains sentences that people have used to describe themselves when they have back pain. When you read them, you may find that some stand out because they describe you today. As you read the list, think of yourself today. When you read a sentence that describes you today, put a tick against it. If the sentence does not describe you, then leave the space blank and go on to the next one. Remember, only tick the sentence if you are sure it describes you today.
I stay at home most of the time because of my back
I change position frequently to try and get my back comfortable
I walk more slowly than usual because of my back
Because of my back I am not doing any of the jobs that I usually do around the house
Because of my back, I use a handrail to get upstairs
Because of my back, I have to hold on to something to get out of an easy chair
I get dressed more slowly than usual because of my back
I only stand up for short periods of time because of my back
Because of my back, I try not to bend or kneel down
I find it difficult to get out of a chair because of my back
My back is painful almost all the time
I find it difficult to turn over in bed because of my back
I have trouble putting on my sock (or stockings) because of the pain in my back
I only walk short distances because of my back pain
I sleep less well because of my back
I avoid heavy jobs around the house because of my back
Because of my back pain, I am more irritable and bad tempered with people than usual
Because of my back, I go upstairs more slowly than usual
I stay in bed most of the time because of my back
Because of my back problem, my sexual activity is decreased
I keep rubbing or holding areas of my body that hurt or are uncomfortable
Because of my back, I am doing less of the daily work around the house than I would usually do
I often express concern to other people about what might be happening to my health
Footnotes
This research was presented at the 53rd annual meeting of the Association of University Radiologists, Montreal, Quebec, Canada, May 4–7, 2005.
References
- Received March 4, 2005.
- Accepted after revision April 25, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Mortality in the Vertebroplasty Population
- Effectiveness of vertebroplasty using individual patient data from two randomised placebo controlled trials: meta-analysis
- Asymptomatic and Unrecognized Cement Pulmonary Embolism Commonly Occurs with Vertebroplasty
- Local Anesthesia with Bupivacaine and Lidocaine for Vertebral Fracture Trial (LABEL): A Report of Outcomes and Comparison with the Investigational Vertebroplasty Efficacy and Safety Trial (INVEST)
- Baseline Pain and Disability in the Investigational Vertebroplasty Efficacy and Safety Trial
- Clinical Outcomes with Hemivertebral Filling during Percutaneous Vertebroplasty
- Efficacy of Percutaneous Vertebroplasty for Multiple Synchronous and Metachronous Vertebral Compression Fractures
- Vertebroplasty for the Treatment of Traumatic Nonosteoporotic Compression Fractures
- Minimally Invasive Techniques for the Treatment of Osteoporotic Vertebral Fractures