
Abstract
BACKGROUND AND PURPOSE: Dural fistulas with cortical venous drainage often present with hemorrhage or neurologic deficit, and prompt treatment is indicated. Occlusion of the draining vein by endovascular techniques or surgical disconnection is considered curative. We present our first endovascular experience with use of Onyx via the arterial route in these aggressive fistulas.
MATERIALS AND METHODS: Between October 2008 and October 2009, 8 consecutive patients with a dural fistula with exclusive cortical venous drainage were treated with Onyx. Three patients presented with hemorrhage; 3, with hemianopsia; 1 with bruit; and 1 after incomplete coil occlusion of a benign sigmoid sinus dural fistula. Fistula location was the sigmoid sinus segment in 4, the occipital area in 2, the cavernous sinus in 1, and the torcula in 1.
RESULTS: In all 8 patients, it was possible to occlude the proximal venous site of the fistula with Onyx via arterial feeders, resulting in complete cure in all. In 6 patients, a prolonged (17- to 29-minute) single middle meningeal artery injection was sufficient to occlude the venous site of the fistula with retrograde occlusion of other arterial feeders; in the other 2 patients, 2 injections in supplying arteries were needed. Follow-up angiograms after 6–12 weeks confirmed lasting complete occlusion of the fistulas. All patients were clinically cured, there were no complications.
CONCLUSIONS: In this small series, curative embolization of dural fistulas with exclusive cortical venous drainage by using Onyx via the arterial route was possible in all patients.
Abbreviations
- AP
- anteroposterior
- DAVF
- dural arteriovenous fistula
- IPH
- intraparenchymal hemorrhage
Intracranial DAVFs with retrograde cortical venous drainage are aggressive lesions that can present with intracranial hemorrhage, seizures, progressive neurologic deficit, intracranial hypertension, or dementia.1–4 Because the natural history of untreated lesions is associated with a poor prognosis, prompt treatment is indicated.5,6 Dural fistulas are considered multiple-hole fistulas with multiple arterial feeders draining into 1 single vein. Treatment of DAVFs with cortical venous drainage is aimed at occlusion of the venous drainage or occlusion of all arterial supply and can be surgical, endovascular, or a combination.7–13 Endovascular treatment has traditionally included embolization via an arterial or venous route with use of acrylic glue, particles, coils, or a combination. Recently, the use of Onyx (ev3, Irvine, California) via the arterial route has been reported with promising results.14–18 We report our initial experience with arterial injection of Onyx in the endovascular treatment of dural fistulas with drainage exclusively into the cortical veins.
Materials and Methods
Between October 2008 and October 2009, 8 consecutive patients with dural fistulas with exclusive cortical venous drainage were treated with Onyx. Patient characteristics are summarized in the Table. There were 5 men and 3 women with a mean age of 57 years (range, 36–67 years). Three patients presented with hemorrhage; 3, with hemianopsia; and 1, with bruit. One patient was referred after incomplete coil occlusion of a benign sigmoid sinus dural fistula with residual shunt on a trapped sinus segment. Fistula location was the sigmoid sinus segment in 4, the right occipital area in 2, the left cavernous sinus in 1, and the torcula in 1. Diagnosis was confirmed after angiography of all cerebral vessels on a biplane angiographic unit (Integris Allura Neuro; Philips Healthcare, Best, the Netherlands).
Patient and treatment characteristics of 8 patients with DAVFs with exclusive cortical venous drainage that were treated with intra-arterial Onyx injection
Endovascular treatment was performed with the patient under general anesthesia. A 4F or 5F catheter was positioned in the external carotid artery, and an Onyx-compatible microcatheter (Rebar 105-5081-153, ev3) was coaxially advanced in a dural feeding artery as close as possible to the fistula site. Then, Onyx 18 was slowly injected. When reflux occurred, the injection was paused for 1–3 minutes. Usually, reflux occurred several times before Onyx would advance into the fistula site. In some cases with middle meningeal artery injection, more than a 5-cm reflux was accepted. Once Onyx advanced, it was intermittently injected until the draining veins were filled and all feeders were filled retrograde, thereby completely occluding the fistula. In 1 patient with a cavernous sinus DAVF supplied by branches of the maxillary artery, the maxillary artery was blocked with a microballoon (HyperForm, ev3) to prevent reflux and promote advancement of Onyx into the cavernous sinus.18 The duration of Onyx injections was calculated from time prints on angiographic images. Follow-up angiography was scheduled after 6–12 weeks in all patients. After the procedure, pain was controlled with medication as needed, including morphine or fentanyl. Illustrative cases are provided in Figs 1⇓–3.

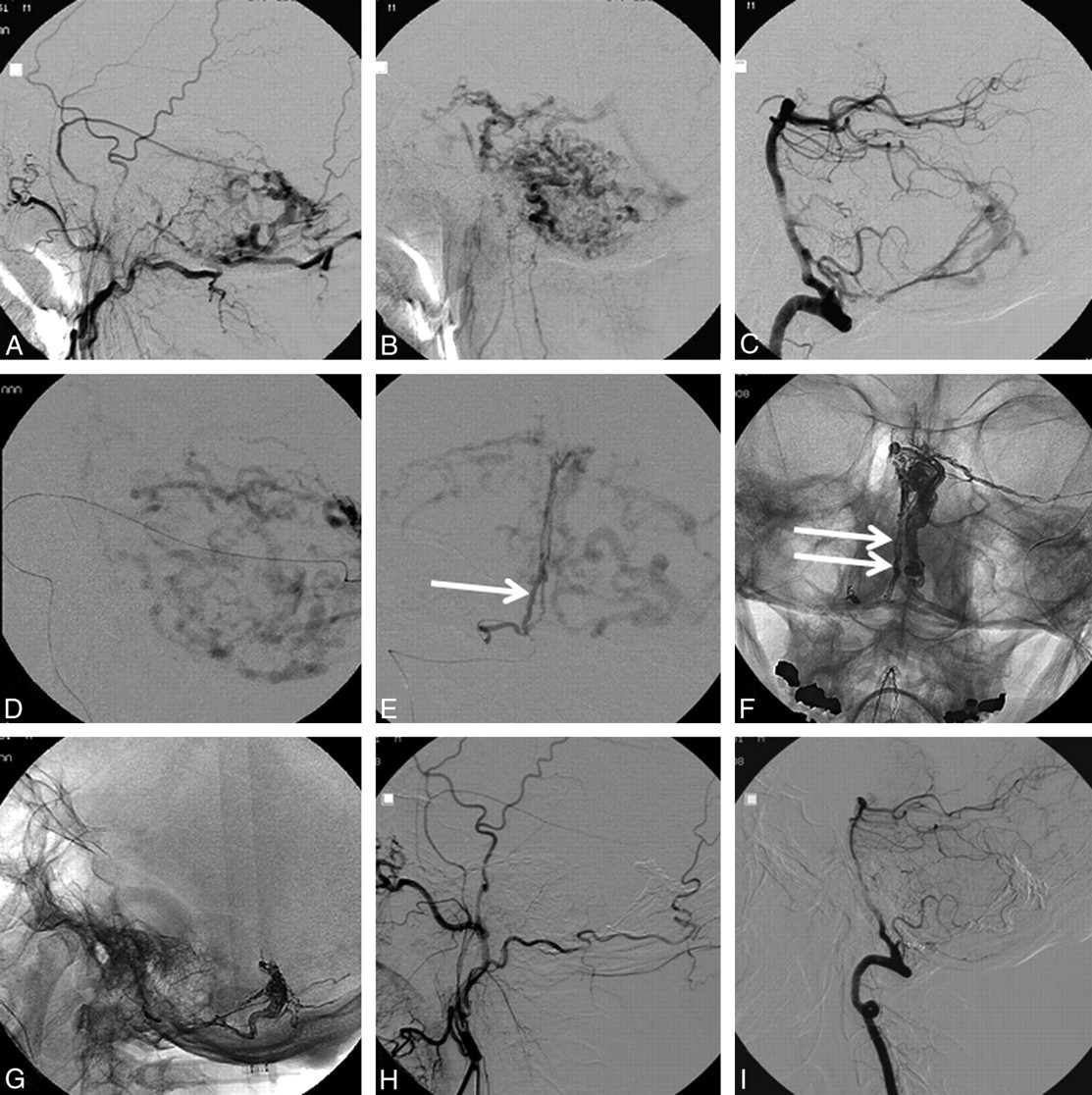
A 58-year-old man (patient 1) with a good-grade (Hunt and Hess II) subarachnoid hemorrhage from a torcular DAVF that was cured with a single Onyx injection from the middle meningeal artery. A and B, Left external carotid angiograms in arterial (A) and venous (B) phases demonstrate a DAVF located on the torcula supplied by the middle meningeal and occipital arteries with marked congestion of cerebellar and even perimedullary veins. C, Supply to the DAVF by the posterior meningeal artery arising from the right vertebral artery. D, Microcatheter distally in the middle meningeal artery close to the fistula used for Onyx injection. E, AP view of selective angiography of the posterior meningeal artery (arrow) arising from the right vertebral artery. F, Same view as in E shows an Onyx cast in the draining vein and retrograde in the posterior meningeal artery (double arrows). G–I, Lateral views of Onyx cast (G), external carotid (H), and right vertebral (I) angiogams 10 weeks after embolization demonstrate complete occlusion of the DAVF.

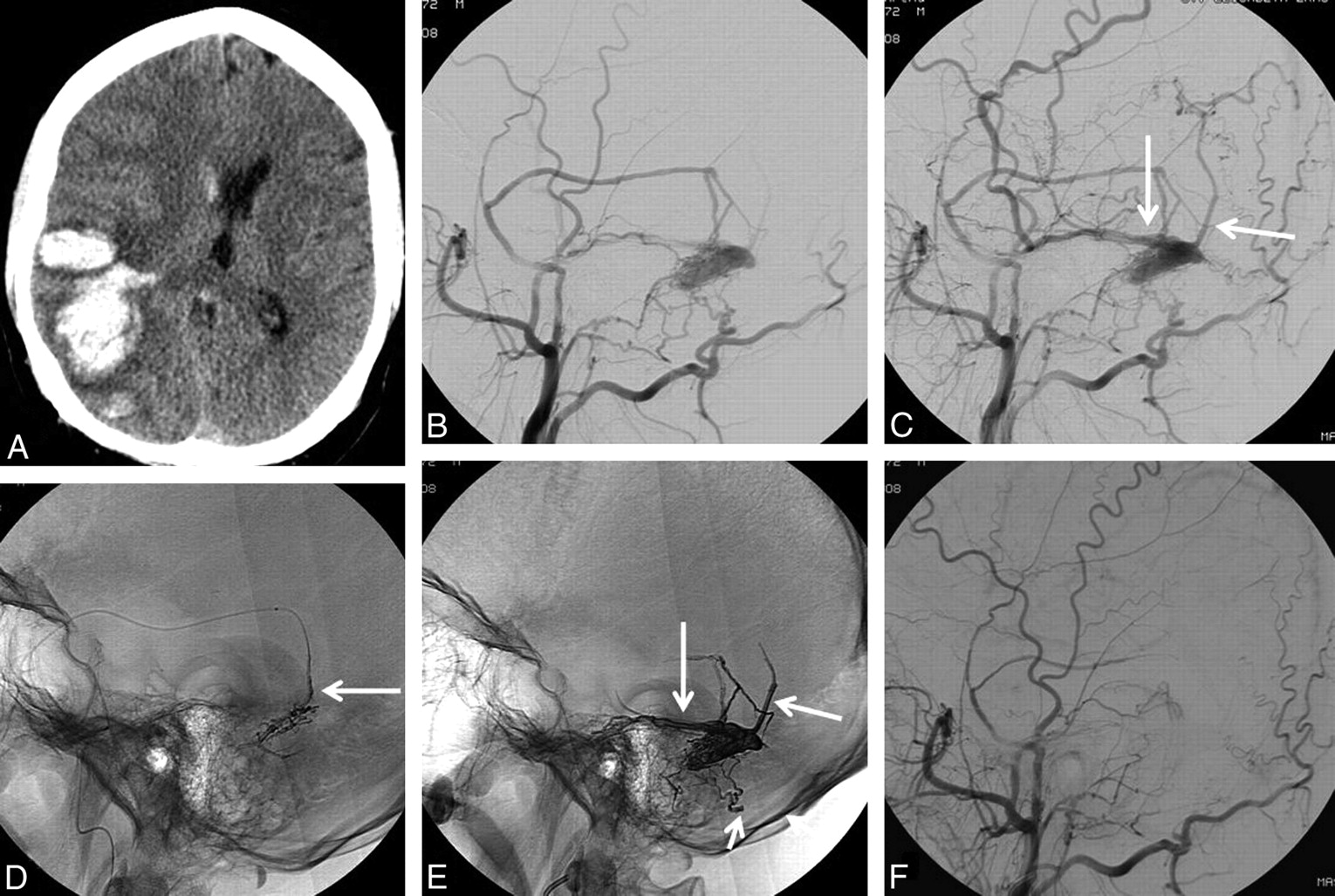
A 36-year-old man (patient 2) with a parenchymal hemorrhage from a DAVF. A, CT scan demonstrates a right parenchymal hematoma. B and C, Early (B) and later (C) phases of a right external carotid angiogram reveal a DAVF located on an isolated open segment of an occluded transverse sinus. The fistula is supplied by the middle meningeal, posterior auricular, and occipital arteries with drainage to the vein of Labbé and a posterior cortical vein (arrows in C). D, Early phase of Onyx injection through a microcatheter, which was positioned close to the fistula in the middle meningeal artery (arrow). Onyx is injected slowly and first fills the dural feeders in the sinus wall. E, Note the Onyx cast at end of injection. The open sinus segment, the proximal draining veins (long arrows), and dural supply from the occipital artery (short arrow) are occluded. F, Complete occlusion of the DAVF is confirmed by postprocedural and follow-up angiography.

A 59-year-old woman (patient 5) with a right occipital parenchymal hemorrhage from a DAVF. A, CT scan demonstrates a right parenchymal hematoma. B, AP view of a right external carotid angiogram shows a DAVF mainly supplied by the middle meningeal artery. Note the aneurysm on the occipital draining vein. C, Onyx cast after embolization through the middle meningeal artery. All dural supply and the draining veins together with the venous aneurysm are occluded. D, Follow-up carotid angiogram after 12 weeks confirms complete occlusion of the DAVF.
Results
All DAVFs could be cured in a single session, in 6 patients with a single Onyx injection and in 2 patients with 2 injections each. The duration of the Onyx injection in the 6 patients with a single injection was 17–29 minutes (mean, 23 minutes). In all cases, removal of the microcatheter was uneventful, despite sometimes long segments of reflux. Follow-up angiography in all patients confirmed durable obliteration. There were no complications of treatment. Radiation-induced hair loss did not occur. Six patients experienced postprocedural pain, probably because of dural ischemia. Morphine was needed in 2 patients. and fentanyl, in 1 to control the pain. Patients treated electively were discharged home the day following embolization. At the time of follow-up angiography, all patients were pain-free without medication. In 3 patients with hemianopsia as a result of venous congestion in the occipital lobe, visual fields were restored to normal within 12 weeks.
Discussion
Our initial experience in a small patient group by using Onyx for DAVFs with cortical venous drainage is hopeful and confirms the good results reported by others.14–18 Since we adopted Onyx as treatment of choice for these aggressive and rare lesions, all patients could be cured in a single session and mostly with only 1 Onyx injection of less than a half-hour duration. The technique we used to inject Onyx in DAVFs is comparable with the technique for the treatment of brain arteriovenous malformations19: Once a distal position of the tip of the microcatheter in a dural feeder close to the fistula is reached, reflux is slowly built up with a 1- to 3-minute pause between injection attempts until the feeding artery is plugged and Onyx starts to advance into the fistula and the draining veins. Sometimes 5–15 attempts are needed before Onyx advances; thus, patience is required. When in a long feeding vessel (mostly the anterior division of the middle meningeal artery), a distal position is obtained, reflux of 5 cm or even more can be accepted, and many injection attempts are possible. Even after injections of almost half an hour with a long segment of reflux, the Rebar microcatheter could be retrieved without difficulty. Thus, the length of reflux in these dural arteries is not directly related to the possibility of removal of the microcatheter. Onyx does not react with or stick to the vessel wall; it merely fills the vessel lumen.20 Therefore, it is important to completely fill all vessels involved in the fistulous complex; deposition of Onyx in the proximal draining vein only may not be sufficient to completely occlude the fistula or may give rise to recurrence at follow-up.
We suspend the injection for a short period of time when Onyx starts to fill the veins. With repeated injection, additional Onyx often initially is deposited more proximally, including retrograde filling of other dural feeders, before further distal advancement in the veins. This technique can be repeated several times, thereby slowly achieving complete occlusion of the fistula, all dural feeders, and the proximal draining veins with complete luminal filling. In selected cases, a microballoon proximal to the tip of the Onyx microcatheter can help in this injection process by preventing reflux and stimulating advancement of the Onyx.18 In our experience, confirmed by others,15,17 the middle meningeal artery is the most suitable for Onyx injection; it is often involved in dural fistulas and can be readily catheterized to a distal position, and long segments of reflux can be accepted because microcatheter removal proved to be easy in such cases. Whenever this artery contributes to the fistula, we try to use it for embolization.
Other vessels such as the occipital artery are mostly more tortuous and less easy to catheterize. When the tentorial artery is involved and has to be used as access for embolization, we probably still prefer injection of acrylic glue under protection of a microballoon across the origin in the internal carotid artery.21 Although we had no complications of treatment, postprocedural pain was experienced by most patients, and adequate pain medication was needed in some patients. Pain is probably related to ischemia of the dura as a result of occlusion of dural arteries. Pain usually gradually decreased in the following days to weeks, and at the time of follow-up angiography after 6–12 weeks, no patients used analgesics.
Another matter of concern is the radiation dose. Often many angiographic runs are necessary to document the dural fistula. In addition, prolonged Onyx injection during fluoroscopy adds to this dose. For dose reduction, we avoid simultaneous biplane fluoroscopy, and we approximate the flat panels as near as possible to the patient's head.
As with other embolic agents, complications with Onyx may occur. Ischemic damage to the trigeminal and facial nerve may be associated with too proximal reflux of Onyx in the middle meningeal artery beyond the foramen spinosum when occlusion of cavernous and petrosal branches may occur. Reflexive bradycardia may be associated with the treatment of tentorial DAVFs. When anastomoses of external carotid artery branches to the vertebrobasilar system remain unrecognized, migration of Onyx may cause posterior circulation infarctions.22–24 However, in our opinion, with proper technique and sufficient anatomic knowledge, these complications can mostly be avoided.
Conclusions
In conclusion, our limited experience with the use of Onyx for arterial embolization of DAVFs with cortical venous drainage is encouraging, with complete cure in all 8 patients without complications.
References
- Received December 21, 2009.
- Accepted after revision February 20, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantifying the Cerebral Hemodynamics of Dural Arteriovenous Fistula in Transverse Sigmoid Sinus Complicated by Sinus Stenosis: A Retrospective Cohort Study
- Intracranial Dural Arteriovenous Fistulae: Clinical Presentation and Management Strategies
- Onyx embolization of dural arteriovenous fistulas of the cavernous sinus through the superior pharyngeal branch of the ascending pharyngeal artery
- Onyx embolization of dural arteriovenous fistulas of the cavernous sinus through the superior pharyngeal branch of the ascending pharyngeal artery
- Angioarchitecture of Transverse-Sigmoid Sinus Dural Arteriovenous Fistulas: Evaluation of Shunted Pouches by Multiplanar Reformatted Images of Rotational Angiography
- Coiling of a carotid cavernous sinus fistula via microsurgical venotomy: recommendation of a combined neurosurgical and endovascular approach
- Middle Cranial Fossa Sphenoidal Region Dural Arteriovenous Fistulas: Anatomic and Treatment Considerations
- Endovascular Treatment of Ruptured Brain AVMs in the Acute Phase of Hemorrhage