Abstract
BACKGROUND AND PURPOSE: Stent-like, self-expandable devices, the so-called flow diverters, are increasingly used for the treatment of wide-neck cerebral aneurysms. The immediate and short-term results are promising, but no long-term results are available. The purpose of our research was to report the long-term angiographic and cross-sectional imaging results after placement of a PED in 12 patients with wide-neck intracranial aneurysms.
MATERIALS AND METHODS: Twelve wide-neck or otherwise untreatable cerebral aneurysms in 12 patients were treated with the PED. Angiography was performed at 6 and 24 months after treatment. Additional MR and CT angiograms were acquired.
RESULTS: In all patients, angiographic or cross-sectional imaging follow-up of at least 27 months demonstrated complete occlusion of the aneurysms treated with the PED. There were no cases of aneurysm recurrence. Angiography at around 6 months showed complete occlusion in all cases, except 1 that showed complete occlusion at the 29-month follow-up. In 1 patient, a clinically asymptomatic 75% in-stent stenosis was seen on the angiography at 6 months but was resolved completely by balloon dilation. Device placement was successful in all patients. Distal embolization had occurred in 1 patient, but the clot was resolved completely without clinical sequelae. Almost immediate angiographic occlusion was achieved in 2 aneurysms and flow reduction in 10 aneurysms.
CONCLUSIONS: Treatment of wide-neck intracranial aneurysms by PED placement led to successful and durable occlusion in all cases, without severe complications. Endovascular treatment for in-stent stenosis should be considered cautiously, because the underlying stenosis may be transient and disappear within 12 months after treatment.
ABBREVIATIONS:
- CPR
- curved planar reconstruction
- GOS
- Glasgow Outcome Scale
- PcomA
- posterior communicating artery
- PED
- Pipeline Embolization Device
- PITA
- Pipeline for the Intracranial Treatment of Aneurysms
The treatment of wide-neck and giant intracranial aneurysms remains challenging; high recanalization rates and severe periprocedural complications have been reported.1,2 Stent-assisted coil embolization or balloon-remodeling techniques are not possible in all cases. A novel approach to the treatment of wide-neck aneurysms was proposed with the development of flow diverters, which are flexible, self-expandable stentlike devices with a high metal surface area coverage.3⇓⇓⇓–7
The PED (Chestnut Medical Technologies, Menlo Park, California) is 1 of 2 currently available flow diverters. Early reports about the use of the PED for endoluminal reconstruction have shown promising results.5⇓–7 However, the published data of the PITA trial include angiographic follow-up data for only 6 months.5⇓–7 No long-term results are available concerning the time course of aneurysm occlusion or the occurrence of late complications. In addition, case reports about the occurrence of late stent thrombosis and in-stent stenosis fuel the need for long-term follow-up data.8
In this study, we report the cross-sectional imaging and angiographic follow-up results for 24 months in a cohort of 12 consecutive patients treated for wide-neck intracranial aneurysms with the PED.
Materials and Methods
Patient Characteristics
Between February and June 2007, 12 consecutive patients with wide-neck intracranial aneurysms were prospectively treated with the PED in the context of the PITA trial. The study was approved by the institutional ethics committee. Written informed consent was obtained from every patient.
Indication for treatment was either the presence of a wide-neck intracranial aneurysm (neck >4 mm or dome/neck ratio of <1.5) or a failed previous attempt at endovascular treatment. Exclusion criteria were SAH within 60 days, unstable neurologic deficit, or >50% stenosis of the parent artery.
PED
The PED is a flexible, microcatheter-delivered self-expanding stent composed of 48 braided strands of cobalt chromium and platinum.7 The construct provides approximately 30–35% metal surface coverage. Further technical details are published elsewhere.5⇓–7
Antiplatelet Medication Regimen
All patients received 75 mg of clopidogrel and 100 mg of aspirin per day for at least 72 hours before, and 6 months after, the procedure. Aspirin (100 mg/day) was given for an indefinite period. During the procedure, intravenous heparin was administered to achieve an activated clotting time of >250 seconds.
Procedure
The treatment was performed under general anesthesia in all patients. A transfemoral approach was used. The procedure was carried out on a biplane angiographic unit (Artis zee; Siemens, Erlangen, Germany). 3D rotational angiography was used to identify the optimal working angle.
The PED was deployed by a standard procedure.5 First, a 0.027-inch microcatheter (Renegade Hi-Flo; Boston Scientific, Fremont, California) was manipulated across the aneurysm neck. The PED, which was mounted on a delivery wire and constrained within a sheath, was inserted into the rotating hemostatic valve and introduced into the hub of the microcatheter. By pushing the delivery wire, the PED was brought into position for exact deployment. A foreshortening of the device must be considered during positioning, as the constrained PED is 2.5 times its maximally expanded length after deployment. The self-expanding device was deployed by a combination of forward pressure on the delivery wire and retraction on the microcatheter.
To shorten the time to complete aneurysm occlusion, additional placement of platinum coils in a loose packing before PED deployment was performed in 2 out of 3 patients with a ruptured and surgically clipped aneurysm of the contralateral ICA.
Procedural Assessment and Follow-Up Examination
The PED placement was considered technically successful if the aneurysm neck was completely covered with the PED, the patency of the parent artery was assured, and no adverse events were clinically evident. Careful neurologic assessment was performed before and after the procedure, and at discharge, by an independent neurologist.
Follow-up angiographies were scheduled at around 6 and 24 months. To depict any residual flow within the aneurysms, standard projections and the original working projection for PED deployment were used. Aneurysm occlusion was graded with a 3-point modified Raymond scale.9 In-stent stenosis was calculated on the basis of the minimal lumen diameter, and was graded as none (0 to <25%), mild (>25 to <50%), moderate (>50 to <75%), or severe (>75–100%).
In addition to angiography, MR and MRA were performed after approximately 18 and 30 months, respectively, in 6 patients. CTA, on a 320-section volume CT scanner (Aquilion One; Toshiba Medical Systems, Neuss, Germany), was performed at around 36 months in another 6 patients. The imaging protocol included CPR of the stent-bearing vessel segment to assess the PED patency.
Results
Patient Characteristics
Demographic data, clinical presentation, aneurysm location, aneurysm size, and time of angiographic and cross-sectional imaging follow-ups are summarized in the Table. The mean age of the patients was 56.3 ± 10.2 years (range 37–76 years).
Summary of patient characteristics and follow-up results
In 4 patients, the aneurysm was diagnosed incidentally. One patient suffered from mass effect due to a large paraophthalmic aneurysm. In another 2 patients, a neurostent (Neuroform2; Boston Scientific) had been placed as a first step for endovascular treatment of the wide-neck aneurysm. In these patients, a failed attempt at transstental coiling had been made. Two aneurysms showed extensive recurrence after endovascular coil placement (Figs 1 and 2).

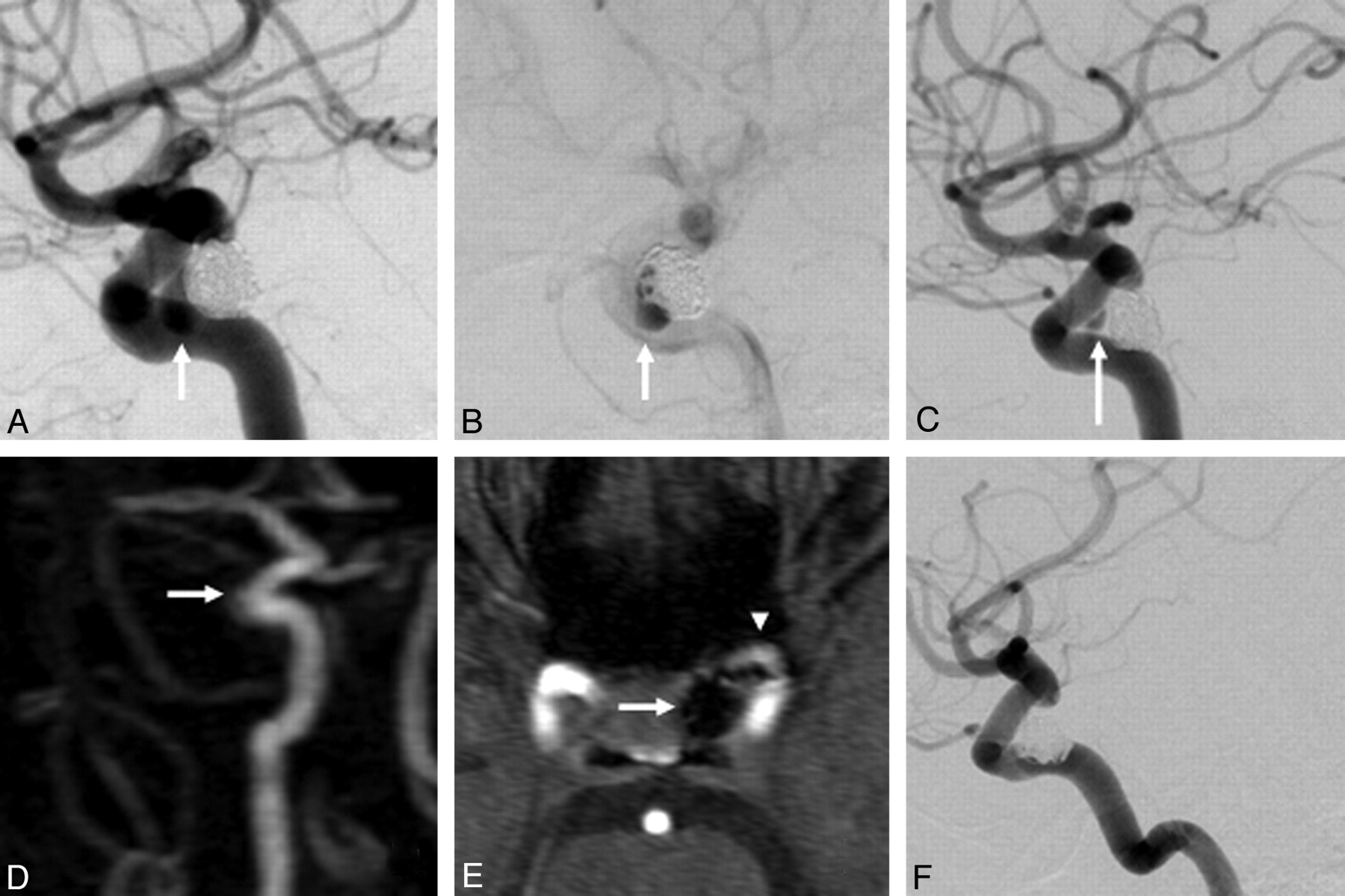
A 76-year-old woman (patient 2) presents with a lobulated 4.1-mm recurrence of a previously coiled 8-mm ICA aneurysm (arrow, A). After placement of a single PED, the recurrence remains visible (arrow, B). At the 6-month angiographic follow-up, recurrence of the aneurysm neck is smaller, but still visible (arrow, C). MRA performed 13 months after PED placement demonstrates complete occlusion of the aneurysm (arrows, D–E) and patency of the parent artery (arrowhead, E). Angiography at 30 months confirms the results of the MR angiography, demonstrating complete occlusion of the aneurysm and excellent reconstruction of the parent artery (F).

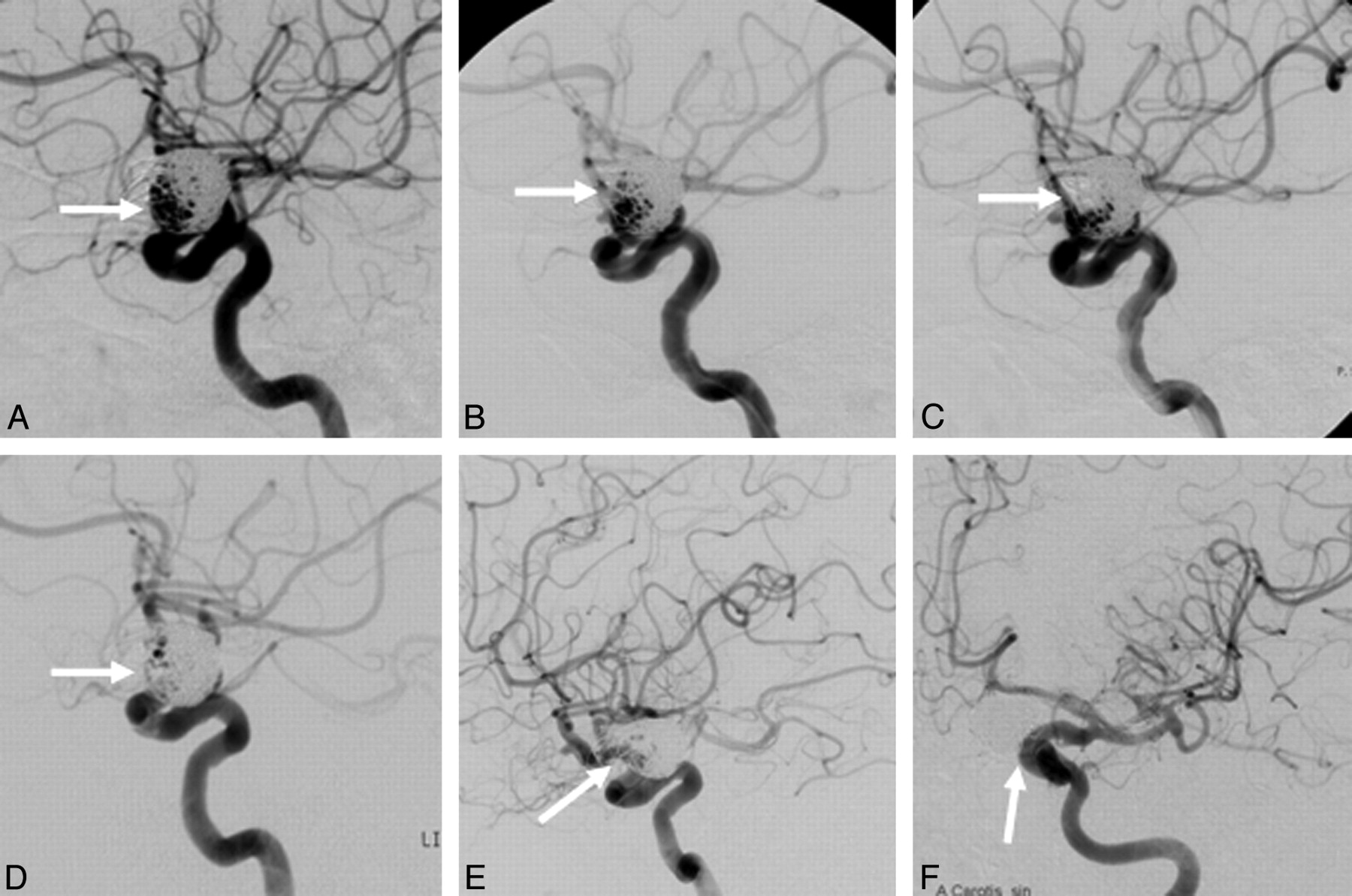
A 61-year-old woman (patient 9) presents with a 16 × 13 mm recurrence of a previously ruptured and subsequently coiled 22-mm ICA aneurysm at the origin of the posterior communicating artery (arrow, A). After placement of a single PED, flow reduction in the superior compartment of the aneurysm recurrence is demonstrated (arrow, B). Due to the broad base of the recurrence, a second PED is placed in a telescopic fashion to sufficiently cover the aneurysm neck and the adjacent arterial segments. After placement of the second PED, significant flow reduction is demonstrated (arrow, C). At the 6-month angiographic follow-up, complete occlusion of the aneurysm recurrence is visible (arrow, D). At the 30-month angiographic follow-up, the aneurysm recurrence is still completely occluded, with excellent reconstruction of the parent artery (arrows E and F).
Three patients suffered from SAH, and the ruptured aneurysms were treated by surgical clipping. However, in all 3 patients, an additional unruptured wide-neck aneurysm, which was then treated with PED, was present. Two of these patients were harboring aneurysms with a size of 7 and 10 mm, respectively. The risk of aneurysm rupture in these 2 patients was considered high, and thus additional placement of platinum coils was performed.
Of the 12 total aneurysms, 2 (17%) were located at the origin of the PcomA, 6 (50%) originated from the paraophthalmic segment of the ICA, 3 (25%) from the intracavernous segment of the ICA, and 1 (8%) originated from the vertebral artery at the origin of the PICA. The mean aneurysm size was 7.8 ± 3.3 mm (range 4.1–16 mm). The size of the aneurysms was calculated from the nonthrombosed lumen or residual lumen, as visualized on angiography.
Technical Outcome
The following sizes of PEDs were used: 3.5 × 14 mm (in 4 patients), 3.75 × 14 mm (3×), 3.75 × 17 mm (1×), 4 × 18 mm (1×), 4.25 × 14 mm (1×), 4.5 × 14 mm (4×), and 4.75 × 14 mm (1×). In 3 patients, the longest available PED was considered too short to sufficiently cover the aneurysm neck and the arterial segment immediately proximal and distal to the aneurysm. Thus, placement of 2 PEDs in a telescopic fashion was necessary (Fig 2). Device placement was successful in all patients. In 2 out of 4 patients with previously ruptured and surgically clipped aneurysms of the contralateral ICA, additional coil placement was performed.
In 1 patient, a distal embolization to a branch of the middle cerebral artery occurred during PED placement. In this patient, 15 mg of abciximab were administered and the clot resolved completely.
Clinical Outcome
Clinical outcome, as assessed by the GOS, was 5 in all patients. In 1 patient, a single episode of amaurosis fugax occurred on the day after the procedure. Mild aphasia was observed in 1 patient with distal embolization. In both patients, the symptoms resolved completely within 24 hours after treatment, without permanent deficits. During follow-up, no procedure-related symptoms or adverse events were recorded.
Angiographic and Imaging Follow-Up
In all patients, the first angiographic follow-up was performed after approximately 6 months (range 5–7 months). In all but 1 patient, another follow-up angiography was performed at approximately 30 months after PED placement (range 27–31 months). One patient, who had experienced a SAH 3 months before and had been treated surgically, did not wish to be followed by angiography at 24 months due to severe mental depression. However, the angiography at 6 months in this patient showed complete occlusion of the aneurysm. In addition to the scheduled angiographic follow-up, all patients were scheduled for MRA or CTA on a regular basis (range 12–47 months).
At the final angiogram after PED placement, 2 aneurysms were almost completely occluded, with only minimal observable residual flow (Fig 3). In another 2 patients, a residual perfusion of <50% was observed. In each of 7 (58.3%) aneurysms, a residual perfusion of approximately 80% was observed. One aneurysm showed almost complete perfusion despite PED. Angiography at around 6 months showed complete occlusion in all cases, except 1 that showed complete occlusion at 29-month follow-up. Once completely occluded, no aneurysm showed recurrence.

{kind=link}
{kind=link}
{kind=link}
A 51-year-old woman (patient 11) harboring an incidental 10-mm paraophthalmic aneurysm (arrow, A). Immediately after treatment with a single PED, only minimal residual flow is visible on angiography (arrow, B). Angiography also depicts a minimal pre-existing lumen narrowing shortly before the funnel-shaped origin of the posterior communicating artery (arrowhead, A–B). At 6-month follow-up, angiography and 3D reconstruction of the rotational angiography show complete occlusion of the aneurysm and 75% stenosis at the distal end of the PED (arrows, C and D). At that time, the PED is fully deployed (E), but a small translucent rim along the inner surface of the PED is visible (arrows, F–G). Percutaneous balloon angioplasty is performed 7 months after PED placement. Control angiography after 13 months demonstrates only minimal residual stenosis (about 30% lumen narrowing; arrow, H) that is completely resolved, as demonstrated on the 31-month angiographic follow-up (arrows, I). However, a small translucent rim, possibly resembling a neointimal layer, is still visible on angiography (arrows, I). There are no signs of recurrence of the aneurysm, which remains completely occluded.
One patient (patient 2) had been treated by endovascular coil placement 5 years before this study. The recurrence of the coiled aneurysm was treated with a PED in the present study. The aneurysm showed residual perfusion at the 6-month angiography but was occluded completely at the 24-month angiography. The MRA performed at 13 months showed complete occlusion of the aneurysm (Fig 1).
In another patient (patient 5), two Neuroform stents had been placed but subsequent endovascular coil placement had failed. In this patient, angiography at 6 months showed 80% residual perfusion. Angiography at 29 months and CTA at 12 months showed complete occlusion of the aneurysm.
Of the 12 patients, 11 (91.7%) had no stenosis of the parent artery where the PED was placed. In 1 patient (8.3%), severe (75–100%) in-stent stenosis was seen on the 6-month angiography (Fig 3). Balloon dilation (Gateway 3/9 mm; Boston Scientific) was performed at 7 months. At the 13-month angiographic follow-up, mild (>25%–50%) residual stenosis was seen. No treatment was indicated at that time. An additional angiographic follow-up at 31 months showed no significant stenosis (Fig 3). In this patient, a single episode of amaurosis fugax was observed immediately after the procedure and was completely resolved within 24 hours.
Discussion
The development of flow diverters for the thrombosis of wide-neck and giant aneurysms has elicited great enthusiasm in the neurointerventional community. Several early reports about the successful use of such devices, and the immediate technical and clinical outcomes, have been published.5⇓–7 The reported periprocedural and midterm follow-up results have been impressive.5⇓–7,10 Meanwhile, reports about the occurrence of late thrombosis, fatal hemorrhage, and delayed complications, such as stent migration, have also been published.8,11,12 These publications have outlined the possibility of delayed aneurysm rupture in aneurysms treated with flow-diverter stents. Several possible causes for this phenomenon have been discussed, such as intra-aneurysmal flow modification, acute thrombosis of large or giant aneurysms, or inflammatory reactions.13 However, studies that carefully assess any potential early or late unexpected or undesirable effects related to the use of flow diverters are unavailable.
The current study is the first to report long-term angiographic and cross-sectional imaging results after placement of a PED for the treatment of wide-neck or otherwise untreatable aneurysms. The results demonstrate excellent technical success rates and immediate, midterm, and long-term results. No complications leading to permanent neurologic deficits occurred, and all but 2 treated aneurysms showed complete occlusion within the first 6 months after treatment. These results are consistent with previous studies that have reported 93–94% rates of complete aneurysm occlusion after 6 months.6,7
In 1 of the 12 aneurysms, a delayed occlusion of an 8-mm aneurysm was observed, which was probably caused by the previous placement of 2 Neuroform stents. In this patient, CTA after 12 months showed complete occlusion of the aneurysm. The indwelling self-expandable stent may have impaired a contagious and homogeneous neointimal and endothelial coverage of the aneurysm neck, and thereby inhibited complete occlusion.5
One patient (8.3%) developed severe in-stent stenosis that was seen on the 6-month angiography. Although existing data about the development of in-stent stenosis in flow-diverting devices is sparse, potential stent occlusion due to exaggerated intimal hyperplasia may be relevant. An experimental investigation in 18 rabbits showed no cases of stenosis of the PED after up to 6 months.3 Another previous study reported moderate or severe stenosis in 4 out of 38 (10.5%) PED cases with angiographic follow-up of ≥3 months.5 All of these patients were clinically asymptomatic, and spontaneous regression of the stenoses was reported. Another study found mild stenosis in only 1 out of 30 patients at the 6-month angiography,7 while minimal lumen narrowing at 6-month angiography was seen in 1 of 19 (5.3%) patients of another report.6
In the case with severe in-stent stenosis, balloon dilation at 7 months was performed with the objective to prevent further progression of the stenosis and thus possible stent occlusion. At 13 months, angiographic follow-up revealed mild (>25%–50%) residual stenosis that was completely resolved at 31 months (Fig 3). It is questionable whether the stenosis should have been treated at all; the presence of a circular translucent layer on the inside of the PED (as depicted on the angiogram) likely was only the result of a transient inflammatory response leading to temporary changes at the vessel intima (Fig 3, F–G). Existing data about the development of intimal hyperplasia is derived mainly from the coronary literature. Intimal hyperplasia peaks at 12–16 weeks and very rarely progresses beyond 3–6 months after bare-metal stent implantation.14⇓–16 In 1 study, 8 out of 24 patients developed asymptomatic in-stent stenosis after placement of a Silk stent (Balt, Montmorency, France).12 Thus, progressive in-stent stenosis may be considered a transient finding that is not accompanied by clinical symptoms. However, at the time the in-stent stenosis was detected, the lack of long-term experience with the PED had led to the decision to balloon dilate the stenosis despite the absence of clinical symptoms. In light of the findings of the current study, the authors propose treatment of such a stenosis only if a progressive lumen narrowing is observed or the patient becomes clinically symptomatic.
Another possible complication after PED treatment is the development of late stent thrombosis. In a reported case of very late thrombosis after 23 months, the authors hypothesized whether the event was attributable to the placement of 3 PED devices or the additional use of polyglycolic/polylactic acid–covered bioactive coils.8 In another series, 1 of 19 patients developed stent thrombosis; retrospectively, it was found that the patient had not suitably been prescribed antiplatelet agents.6 The occluded arterial segment reopened later, while the patient was on proper medication. A similar case has been reported for the Silk stent, though no clear explanation for the event could be given.13 Acute thrombosis, inflammatory reactions or intra-aneurysmal flow changes were considered. Another study did not find any delayed in-construct stenoses, but the follow-up time was only 6 months.7 In our series, we did not observe late stent thrombosis.
The present study has the following limitations: First, the number of patients treated with the PED is small. Thus, the results may not be generalized. However, as this is the first investigation reporting long-term angiographic results, including information about the time courses of aneurysm occlusion and possibly transient in-stent stenosis, the presented data may be relevant. Second, the mean size of the treated aneurysms was relatively small and telescopic stent placement was performed only in 3 patients. The rate of in-stent stenosis may be higher if a larger number of patients with more than 1 inserted PED were evaluated.
Conclusions
The use of the PED in patients with wide-neck or otherwise untreatable cerebral aneurysms is a safe and highly effective treatment technique with excellent long-term angiographic results. The occlusion of many aneurysms can be expected within the first 6 months after treatment. The rate of in-stent stenosis is low. Moreover, the endovascular treatment of such stenoses should be cautiously considered, because the underlying stenosis may be transient and disappear within 12 months after treatment. Large-scale prospective trials should be performed to evaluate the long-term patency rates of the PED as well as the rate of delayed complications.
Footnotes
Disclosures: Hannes Deutschmann—UNRELATED: Travel Accomodations: eV3, Comments: Travel expenses for conference in Lyon, France refunded by eV3 (2010); OTHER RELATIONSHIPS: The Pipeline Embolization devices used in the current study were provided by Chestnut Medical, Menlo Park, California. There was neither payment to any of the authors or co-authors nor to the institution. There are no relationships of any kind to Chestnut Medical other than scientific interest in using the device.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- Received March 19, 2011.
- Accepted after revision June 1, 2011.
- © 2012 by American Journal of Neuroradiology