Abstract
BACKGROUND AND PURPOSE: Intraocular silicone oil injection has been used to treat complicated retinal detachments, and recently its retrolaminar and intracranial migration has been reported. The purpose of this study was to document the prevalence of posterior migration of intraocular silicone oil on head CT and describe the clinical and radiologic findings.
MATERIALS AND METHODS: This retrospective study included 57 patients with intraocular silicone oil injection who underwent unenhanced head CT between November 2008 and July 2018. All images were visually evaluated for subretinal and retrolaminar migration of intraocular silicone oil involving the anterior visual pathway (optic nerve, optic chiasm, and optic tract) and the ventricular system. Attenuation values of those structures were measured and compared with those of the contralateral or adjacent normal structures.
RESULTS: We detected subretinal and retrolaminar silicone oil migration in 7 of the 57 patients (12%), noting silicone oil at the optic nerve head (n = 2), retrolaminar optic nerve (n = 5), optic chiasm (n = 3), optic tract (n = 3), and in the lateral ventricles (n = 1). Attenuation values of the structures with silicone oil migration were significantly higher than those of the control regions (optic nerve head, 69.2 ± 12.4 vs 29.8 ± 10.2 HU, P < .001; retrolaminar optic nerve, 59.9 ± 11.6 vs 30.9 ± 8.6 HU, P < .001; optic chiasm, 74.2 ± 11.0 vs 25.6 ± 6.9 HU, P < .001; optic tract, 70.1 ± 4.7 vs 28.7 ± 7.2 HU, P < .001). No significant ophthalmic or neurologic complications were documented in the patients with silicone oil migration.
CONCLUSIONS: Subretinal and retrolaminar migration of intraocular silicone oil is common. Although there were no apparent complications associated with silicone oil migration, the radiologist and clinician should be aware of this phenomenon.
ABBREVIATION:
- SiO
- silicone oil
Retinal detachment is a serious medical condition that may lead to blindness if not adequately treated.1 Intraocular silicone oil (SiO) injection following vitrectomy is commonly used as an endotamponade technique to repair complex retinal detachments.2 Although considered relatively safe, the use of intraocular SiO is not without complications. The development of glaucoma, cataracts, and keratopathy is a known complication resulting from the diffusion of SiO from the vitreous cavity into adjacent structures.3,4
Retrolaminar SiO migration is a lesser known complication of intraocular SiO injections, occurring when the SiO diffuses posteriorly into the optic apparatus (optic nerve, chiasm, and tract) and potentially into the subarachnoid space and ventricular system.5-7 Vision loss due to optic neuropathy has been reported as a consequence of this posterior migration.8 Although several histologic and immunohistopathologic studies have demonstrated SiO migration in the ophthalmologic literature,6,9 data about the prevalence and/or radiologic findings of SiO migration are limited.5,10-21
The purpose of this study was to document the prevalence of retrolaminar migration of intraocular SiO on head CT and describe the clinical and radiologic findings.
Materials and Methods
Patients
The institutional review board approved this retrospective study. The requirement to obtain written informed consent was waived. Patients with SiO injection treatment who underwent head CT from November 2008 to July 2018 were searched through the Radiology Information System of our department using a keyword “silicone.” The start date of the study was set as November 2008 when we started including thin-section (1.25 mm) images in our routine unenhanced head CT protocol. Patients who did not have 1.25-mm images were excluded from the study. Patients with severe motion artifacts were also excluded. The electronic medical records were evaluated for patient demographics, relevant medical history, indication of SiO injection treatment, indication for CT examinations, interval between SiO injection treatment and CT examination, ophthalmic examination findings, and intraocular pressure (millimeters of mercury) (Table 1 and On-line Table).
Comparisons of clinical features between cases positive and negative for silicone oil migration
CT Imaging Techniques
All unenhanced head CT examinations were axially acquired at 5- and 1.25-mm section thickness using 64–detector row CT scanners (LightSpeed VCT; GE Healthcare, Milwaukee, Wisconsin) with soft-tissue and bone algorithm reconstructions per our institutional clinical protocol. Axial soft-tissue algorithm-reconstructed 1.25-mm images were used for analysis.
Qualitative Imaging Analysis
All images were visually evaluated for subretinal and retrolaminar migration of SiO, which was defined as areas of increased attenuation of ≥1 component of the visual tract (optic nerve head, retrolaminar optic nerve, optic chiasm, and optic tract) or within the ventricular system. Posterior migration of silicone was assessed by 2 radiologists (M.A. and K.T., with 3 and 17 years of experience in head and neck radiology, respectively) who independently reviewed the CT images; any discrepancies between the 2 radiologists were resolved during a third analysis session in which a decision was reached zby consultation with a third radiologist (O.S., with 25 years of experience in head and neck radiology).
Quantitative Imaging Analysis
Attenuation values of the intraocular SiO and the visually identified regions in the visual pathway and ventricles were measured in Hounsfield units. We placed single, as-large-as-possible, freeform ROIs within each region on the image with the largest cross-sectional area, avoiding partial volume effects. The attenuation value of the optic nerve was measured at the midportion of the intraorbital segment. Care was taken not to include calcification, partial volume effects, or artifacts within the ROIs. The difference between each region and its contralateral side was calculated as the absolute difference in the attenuation value. When measuring the optic chiasm or bilateral lesions, comparison with an adjacent normal structure was performed instead.
Statistical Analysis
We compared the clinical information, ophthalmologic findings, and CT features between cases positive and negative for migration. The Fisher exact test was used to compare sex, age, the interval between SiO injection and CT examination, intraocular pressure, and attenuation values were compared using the Mann-Whitney U test. All data for continuous variables are presented as mean ± SD. A P value < .05 was significant in all analyses. All statistical analyses were performed using SPSS, Version 23.0 (IBM, Armonk, New York).
Results
Patients
Fifty-eight patients with a history of intraocular SiO injection who underwent unenhanced head CT examinations for various clinical indications between November 2009 and July 2018 were identified. Among these, 1 patient who did not have 1.25-mm images was excluded. Ultimately, 57 patients (31 men and 26 women; mean age, 57 years; range, 18–87 years) with intraocular SiO injection were included in this study. Nineteen patients were treated with intraocular SiO injection on the right side, and 34 patients, on the left side; 4 patients were treated on both sides.
Clinical, Ophthalmic, and Radiologic Characteristics of Posterior Migration of Intraocular Silicone Oil
The clinical and CT imaging features of SiO migration cases are summarized in the On-line Table. Posterior migration of intraocular SiO was identified in 7 of the 57 patients (12.3%) (4 men and 3 women; mean age, 56 years; range, 23–71 years) with 7 eyes of the 61 SiO-treated eyes (11.5%), with SiO at the optic nerve head (n = 2), retrolaminar optic nerve (n = 5), optic chiasm (n = 3), optic tract (n = 3), and in the lateral ventricles (n = 1). Two patients had migration to 3 locations each (optic nerve, optic chiasm, and optic tract), and 1 patient, to 4 locations (optic nerve, optic chiasm, optic tract, and lateral ventricles). Representative cases of retrolaminar SiO migration are shown in Figs 1–3.

Subretinal silicone oil migration (case 2). Axial CT image obtained 1 week following right intraocular silicone oil injection demonstrates a punctate region of increased attenuation at the optic nerve head (arrow).

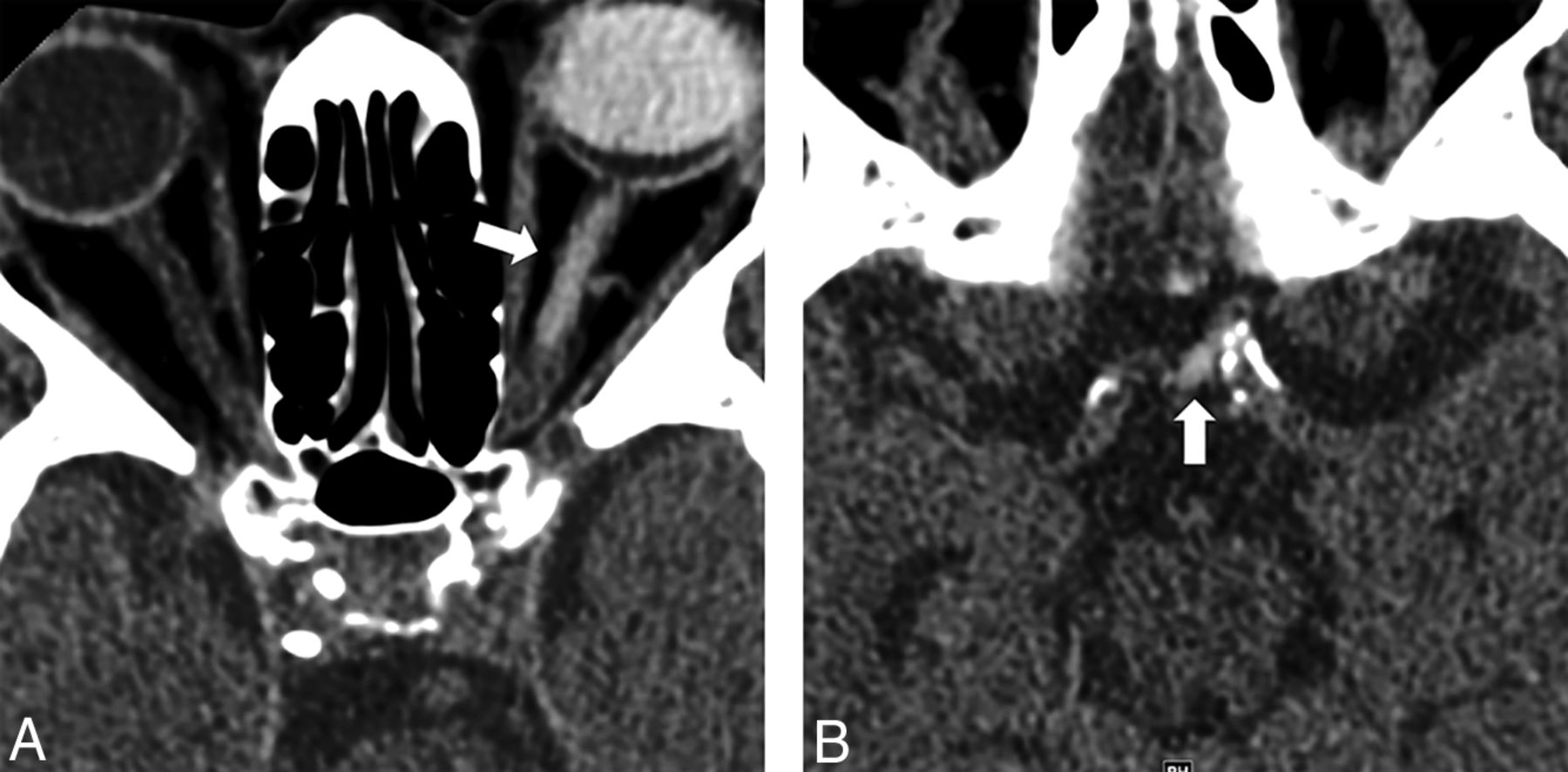
Retrolaminar silicone oil migration at the level of the retrolaminar optic nerve and optic chiasm (case 6). A and B, Axial CT images 1 year after left intraocular silicone oil injection demonstrate abnormal increased attenuation of the intraorbital segment of the left optic nerve (A, arrow) and nodular increased attenuation at the optic chiasm (B, arrow).

{kind=link}
{kind=link}
{kind=link}
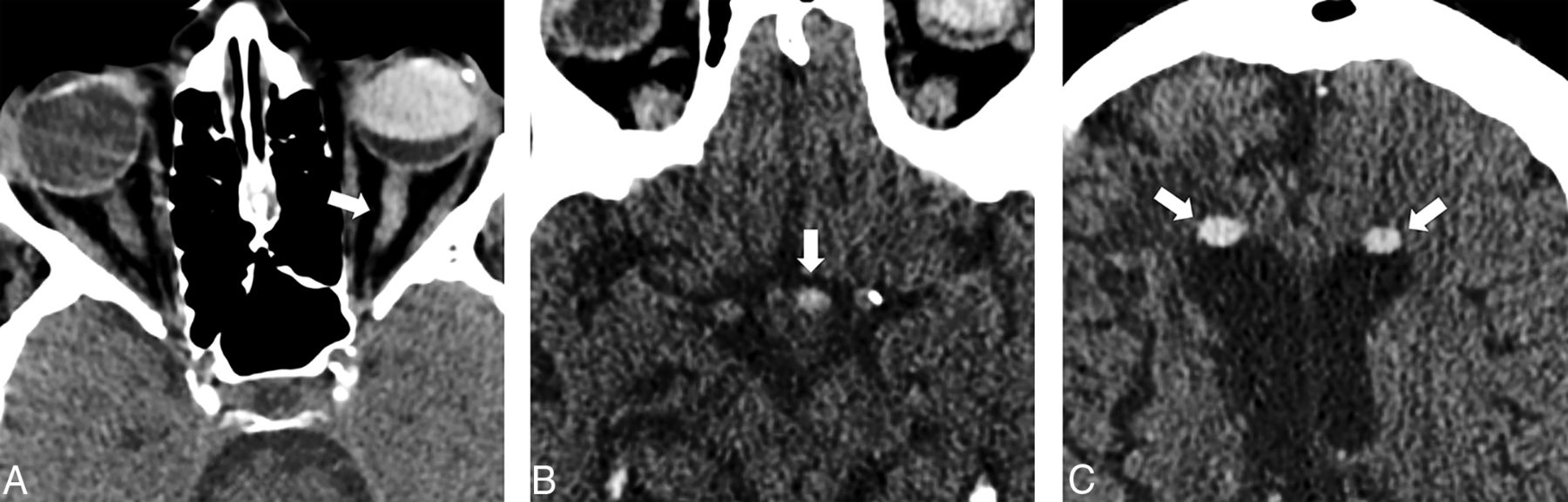
Retrolaminar silicone oil migration to the retrolaminar optic nerve and optic chiasm and within the lateral ventricles (case 4). Axial CT images 6 years after left intraocular silicone oil injection demonstrate tubular increased attenuation of the intraorbital segment of the left optic nerve (A, arrow), nodular hyperattenuation in the optic chiasm/optic tract (B, arrow), and biconvex hyperattenuation in the nondependent regions of the frontal horns of the lateral ventricles (C, arrows).
Comparison of Clinical Findings between Cases Positive and Negative for Migration
Clinical characteristics in cases positive and negative for migration are summarized in Table 1.
Comparisons of attenuation values in the visual tract structures between silicone oil migration lesions and normal regionsa
We had recorded vision for 34 of the 57 patients in the cohort (4/7 patients positive for SiO migration and 30/50 negative for SiO migration). For the cases positive for SiO migration, 1 patient had 20/400 vision, 1 had finger-counting vision, and 4 had no light perception vision. For the SiO cases negative for migration, 3 patients had 20/400 vision, 3 had finger-counting vision, 5 had hand motion vision, 8 had light perception vision, and 11 had no light perception vision. On the basis of the available acuity data, there did not appear to be a difference between the cohorts positive and negative for SiO migration (P = .517). The best-corrected acuity in both groups ranged from 20/400 to no light perception vision.
There was no significant difference in age and sex between cases positive and negative for migration (P = .942, .691, respectively). The interval between silicone injection treatment and CT examination was not significantly different between cases positive and negative for migration (45.8 ± 41.8 versus 37.4 ± 31.7 months, P = .779). Retrolaminar SiO migration was present as early as 1 week and as late as 4 years after injection. Intraocular pressure elevation had been documented in 3 patients with SiO migration. Intraocular pressure on the side of silicone injection treatment showed no significant difference between cases positive (n = 5) and negative for migration (n = 20) (23.6 ± 21.4 versus 15.2 ± 5.2 mm Hg, P = .291).
Quantitative CT Analyses
The attenuation value of intraocular SiO was 91.5 ± 12.5 HU, with no significant difference between cases positive and negative for migration (94.1 ± 2.2 versus 91.1 ± 13.3 HU, P = .228). Attenuation values of the normal structures were not significantly different between the silicone injection side and the contralateral side (optic nerve head, 30.6 ± 13.8 versus 31.4 ± 9.5 HU, P = .173; retrolaminar optic nerve, 34.4 ± 12.9 versus 30.4 ± 7.6 HU, P = .206; optic tract, 31.5 ± 11.5 versus 27.9 ± 7.1 HU, P = .108; whole region 32.2 ± 12.8 versus 30.0 ± 8.2 HU, P = .717). Attenuation values of the regions with SiO migration were significantly higher than those in the control regions (optic nerve head, 69.2 ± 12.4 versus 29.8 ± 10.2 HU, P < .001; retrolaminar optic nerve, 59.9 ± 11.6 versus 30.9 ± 8.6 HU, P < .001; optic chiasm, 74.2 ± 11.0 versus 25.6 ± 6.9 HU, P < .001; optic tract, 70.1 ± 4.7 versus 28.7 ± 7.2 HU, P < .001; whole region, 67.0 ± 10.9 versus 29.2 ± 8.6 HU, P < .001) (Table 2). One case showed high attenuation in both lateral ventricles (right side, 80.1 HU; left side, 78.8 HU) (Fig 3).
Discussion
Intraocular SiO injection is widely used in the management of complex retinal detachments and is considered relatively safe and effective in vitreoretinal surgery.2,22,23 Despite its relatively safe profile, SiO may diffuse into various ocular and extraocular tissues, resulting in complications such as glaucoma, keratopathy, and cataract formation.3,4 It may also diffuse posteriorly into the subretinal space, optic nerve, optic chiasm, subarachnoid spaces, and potentially the ventricular system. This phenomenon, first described by Ni et al, in 1983,6 is known as subretinal or retrolaminar migration of intraocular SiO. The term “retrolaminar” refers to the migration of silicone droplets past the lamina cribrosa, the main structural element where the retinal ganglion cell axons and the central retinal vein and artery enter or exit the eye.24 Although many case reports have described retrolaminar SiO migration, no radiologic studies addressing the frequency or the radiologic features of this phenomenon were found. We believe this is the first study to show the frequency of retrolaminar SiO migration on CT images along with clinical correlation. In this study, migration was detected in 12% of patients, which is comparable with histopathologic studies performed on enucleated eyes with silicone injection (11%–24%).9,25,26 Migration of SiO was noted at the optic nerve head, retrolaminar optic nerve, optic chiasm, optic tract, and in the lateral ventricles, and those findings were confirmed by quantitative analyses.
Retrolaminar SiO migration is believed to be a benign phenomenon usually detected incidentally on cross-sectional imaging.5 However, visual symptoms have been reported and are thought to be related to silicone-induced optic neuropathy secondary to macrophage infiltration.9,26,27 In our series, no significant neuro-ophthalmologic or neurologic complications related to SiO migration have been documented in the medical records.
The exact mechanism of SiO migration remains uncertain. The role of elevated intraocular pressure in SiO migration was first described by Shields in 1989.5 However, not all of our cases or all the published cases were associated with pre-existing elevated intraocular pressure.28 Intraocular pressure at the side of SiO injection treatment in cases positive for migration was slightly higher than that in cases negative for it in our results, though the difference was not statistically significant.
More recent studies suggest that SiO may infiltrate or diffuse directly into the retinal layers and then into the optic nerve by infiltrating along the retinal nerve fibers through the lamina cribrosa. In 2006, Kuhn et al29 proposed that optic pits (congenital abnormalities of the optic nerve head) may serve as an entry point for the retrolaminar migration of SiO. This infiltration may be facilitated by increased intraocular pressure.5 The entry of SiO into the subarachnoid space and then the ventricular system may be explained by passage of the SiO droplets directly from the vitreous space or from the optic nerve into the perioptic subarachnoid spaces through the perivascular spaces of the central retinal vessels where they pierce the optic nerve.5,8,15 The diffusion of SiO into the ventricular system is less frequently encountered than into the optic nerve. Boren et al5 found 15 case reports of intraventricular SiO.
Silicone oil is usually reported as hyperattenuating on CT images with attenuation ranging between 60 and 140 HU, depending on the viscosity and the location of the SiO.10,30 Our qualitative results, supported by quantitative analysis, showed that attenuation values of the regions with SiO migration were significantly higher than those in control regions. At the optic chiasm, only ipsilateral nodular high attenuation was detected. Within the ventricular system, the SiO characteristically floats in nondependent locations because of its lower specific gravity relative to CSF. On MR imaging, SiO has been reported to be hyperintense relative to CSF or contralateral normal vitreous on T1-weighted images. MR imaging may detect SiO droplets as small as 1 mm3.31
Radiologists should be aware of the occurrence of SiO migration, though it is relatively rare and often without clinical symptoms. Knowledge of the appearance and common locations on CT is important to avoid misdiagnosis of subarachnoid or intraventricular hemorrhage or tumor.
Our study has several limitations. Because posterior migration of SiO is relatively rare, the number of cases positive for migration was small, limiting the statistical power and accuracy of the prevalence. Second, this was a retrospective study that may have been subject to selection bias. Determination of the timing of and chronologic changes in migration was not possible for many patients because imaging follow-up after intraocular injection or after identifying migration is not routinely performed. A detailed ophthalmologic examination including intraocular pressure was not available in all cases, and none had histopathologic confirmation.
Conclusions
Retrolaminar migration of intraocular SiO is a common phenomenon. Radiologists should be aware of its occurrence and familiar with its imaging characteristics and patterns of migration to prevent misdiagnosis.
Footnotes
Paper previously presented, in part, as an oral presentation at: Annual Meeting of the American Society of Neuroradiology and the Foundation of the ASNR Symposium, April 22–27, 2017, Long Beach, California.
Disclosures: Margaret M. Chapman—UNRELATED: Consultancy: Boston Imaging Core Lab. Glenn D. Barest—UNRELATED: Consultancy: Boston Imaging Core Lab. Osamu Sakai—UNRELATED: Consultancy: Boston Imaging Core Lab.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- Received February 27, 2019.
- Accepted after revision July 8, 2019.
- © 2019 by American Journal of Neuroradiology