
Abstract
SUMMARY: Noninvasive tumor control of vestibular schwannomas through stereotactic radiosurgery allows high rates of long-term tumor control and has been used primarily for small- and medium-sized vestibular schwannomas. The posttreatment imaging appearance of the tumor, temporal patterns of growth and treatment response, as well as extratumoral complications can often be both subtle or confusing and should be appropriately recognized. Herein, the authors present an imaging-based review of expected changes as well as associated complications related to radiosurgery for vestibular schwannomas.
ABBREVIATIONS:
- FSRT
- fractionated stereotactic radiation therapy
- ISRS
- International Stereotactic Radiosurgery Society
- SRS
- stereotactic radiosurgery
- VS
- vestibular schwannoma
Vestibular schwannomas (VSs) are benign, slow-growing tumors that most often arise from the vestibular component of the eighth cranial nerve, with the patient commonly presenting clinically with unilateral hearing loss and tinnitus. Less commonly, disequilibrium, ipsilateral trigeminal hypoesthesia or neuralgia, or hydrocephalus may occur.1,2 Advances and wider availability of MR imaging have allowed an earlier diagnosis of these lesions, at times when patients may have only minimal hearing loss or are asymptomatic.3 This has led to an increasing role of minimally invasive management strategies such as stereotactic radiosurgery (SRS) in VS management.2
The International Stereotactic Radiosurgery Society (ISRS) practice guidelines consider both observation and SRS as reasonable treatment options for newly diagnosed VSs without substantial mass effect.4 On the other hand, microsurgical resection can be used for any-sized tumor and is currently considered the treatment of choice for larger tumors.5 In general, lesions up to 2.5 cm in maximal cerebellopontine angle diameter are considered appropriate for SRS treatment, though more recent studies have also explored SRS for larger lesions with acceptable results.4,6,7 The ISRS practice guidelines recommend a dose of 11–14 Gy to the tumor margin for single-fraction SRS in VSs.4 Fractionated stereotactic radiation therapy (FSRT) may also be used and provides a similar 5-year tumor control rate.2 No randomized trials have evaluated the efficacy of SRS versus FSRT for tumor control in VS. Limited available data, however, do not suggest any definite advantage of one technique over the other.8 Unlike SRS, which involves 1–5 fractions, FSRT delivers the prescribed radiation dose in 25–30 fractions to maximize targeting tumor cells during the radiation-sensitive phase of the cell cycle.8
Acute radiation effects following SRS are not uncommon and have been reported in up to 22%–24% of patients. These generally include vertigo, hemifacial spasm, gait disturbance, and exacerbation of pre-existing hearing loss and may appear in the first few months.9,10 SRS, however, can also lead to myriad imaging appearances in VS, which may be more apparent over the ensuing months to years. Herein, we present an imaging-based review of both the common (and often expected) as well as atypical appearances in VS post-SRS. An increased awareness of these findings may help avoid imaging pitfalls as well as recognize complications at an earlier stage.
Pseudoprogression
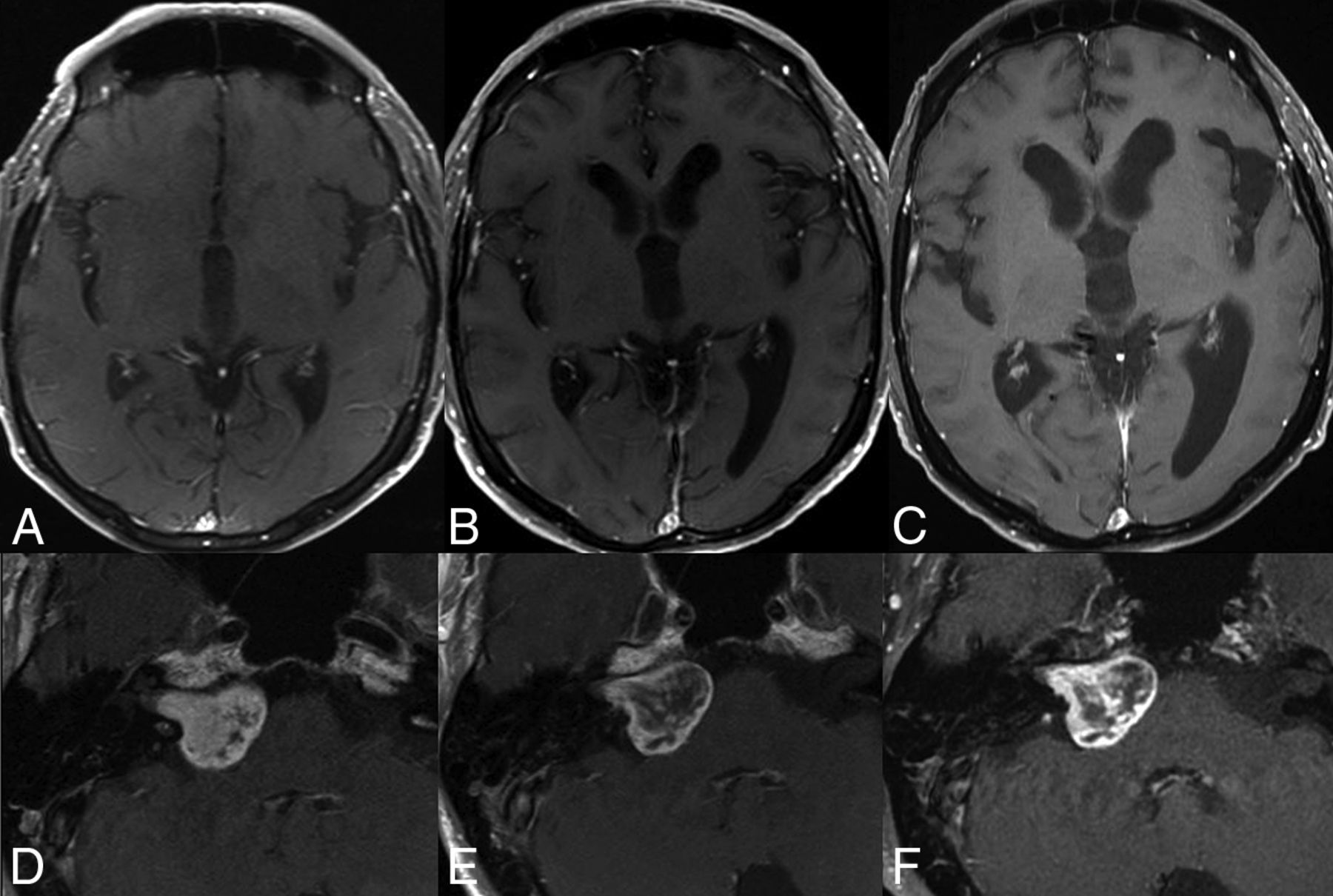
VS treated with SRS may show transient tumor enlargement in the first 3 years after SRS, often referred to as pseudoprogression (Fig 1).5 In such cases, the tumor will develop early swelling or growth but then stabilize or shrink. In contrast, true progression (ie, radiation failure) implies sustained tumor growth over serial MR imaging studies. The incidence of pseudoprogression is variable, ranging between 5% and 74% in different studies.11⇓-13 This wide variability is due to considerable heterogeneity in imaging techniques, measurement methodology (2D versus 3D), and the criteria used to define pseudoprogression, which is variably considered as a 10%–20% increase in the volume of VS over baseline, with some studies even considering any increase in VS volume over baseline as pseudoprogression.13 Regardless, findings are often accompanied by variable loss of central enhancement on MR imaging. Even though several studies have not shown any correlation between pseudoprogression and post-SRS clinical deterioration, a few others have noted a higher incidence of cranial nerve impairment, an increased risk of hydrocephalus requiring shunt placement, and loss of serviceable hearing.13⇓-15

Pseudoprogression in a VS treated with SRS. The tumor volume on the planning scan (A) was 3.9 mL, which increased to 4.4 mL 6 months posttreatment. A follow-up study at 4 years (C) showed tumor regression with a volume of 0.6 mL.
During pseudoprogression, the increase in tumor volume can be quite impressive, with a reported median of 20%–88% over baseline and up to 800% in some cases.13,16 The underlying risk factors for pseudoprogression remain unclear, though 1 study noted higher probability with solid VSs (OR = 2.79; P = .017).12
Pseudoprogression generally peaks around 6 months post-SRS and resolves between 12 and 18 months. However, these timelines are approximate at best, and up to 17% of patients may show late pseudoprogression peaking around 3–4 years, while some may show delayed resolution during the next 2–3 years.11,13 Given the wide variabilities in timelines for pseudoprogression and overlap with treatment failure, there are no well-defined timelines for adjudicating treatment failure. In general, pseudoprogression should be considered when tumor volumes increase in the first 3 years post-SRS.4 A recent systematic review of 300 patients who underwent microsurgical decompression post-SRS also noted that the mean time to surgery post-SRS was 39.4 months, with the overwhelming indication (92%) being tumor growth post-SRS.17
Loss of central lesion enhancement often follows a similar timeline but likely has a different pathogenesis from pseudoprogression (Fig 2). Some authors believe it reflects an early effect of radiation and is not necessarily indicative of long-term tumor control. The reported prevalence varies between 45% and 93% in the literature.11,13 In authors’ personal experience, the loss of central enhancement can vary considerably in individual cases, reaching up to 50%–60% of the tumor volume.

Loss of central enhancement. Postcontrast images obtained pre- (A) and 6 months post-SRS (B) show near-complete loss of central enhancement in the right VS.
Treatment Response and Tumor Growth
SRS can achieve long-term tumor control in >90% of cases with a relatively low risk of neurologic deterioration or facial nerve palsy.6,8,18,19 Tumor control is broadly considered as lesion regression or stability, obviating need for additional intervention (Figs 3 and 4).2,19 Kawashima et al,18 in their cohort, noted tumor regression in 62%, stable tumor in 31%, and enlargement in 7% of patients post-SRS. Treatment failures may be more common with larger or fast-growing tumors at baseline (Fig 5).7,20

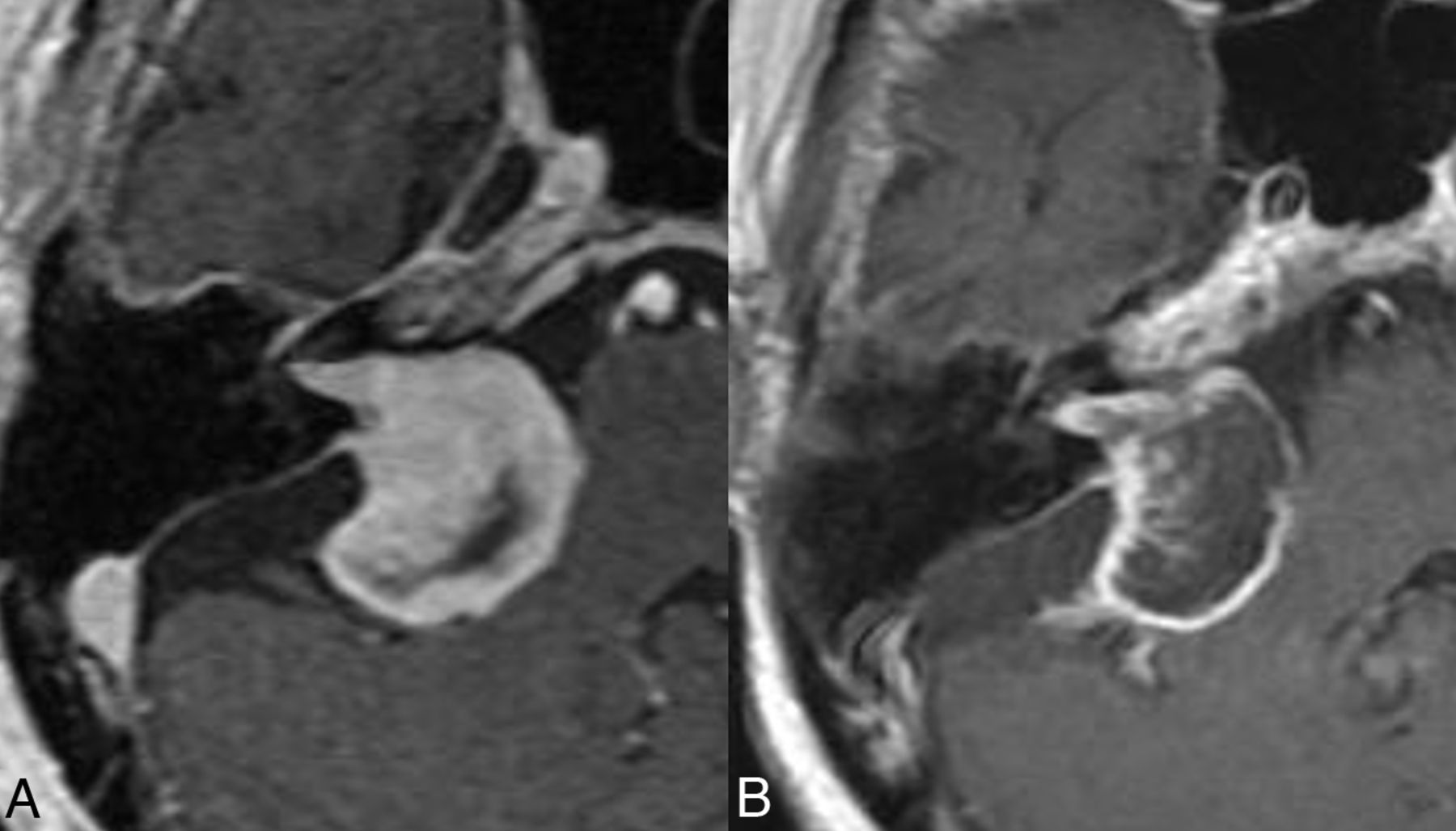
Favorable treatment response post-SRS. Axial postcontrast images obtained pre-SRS (A) and at 8 years post-SRS (B) show considerable lesion regression, consistent with a response.

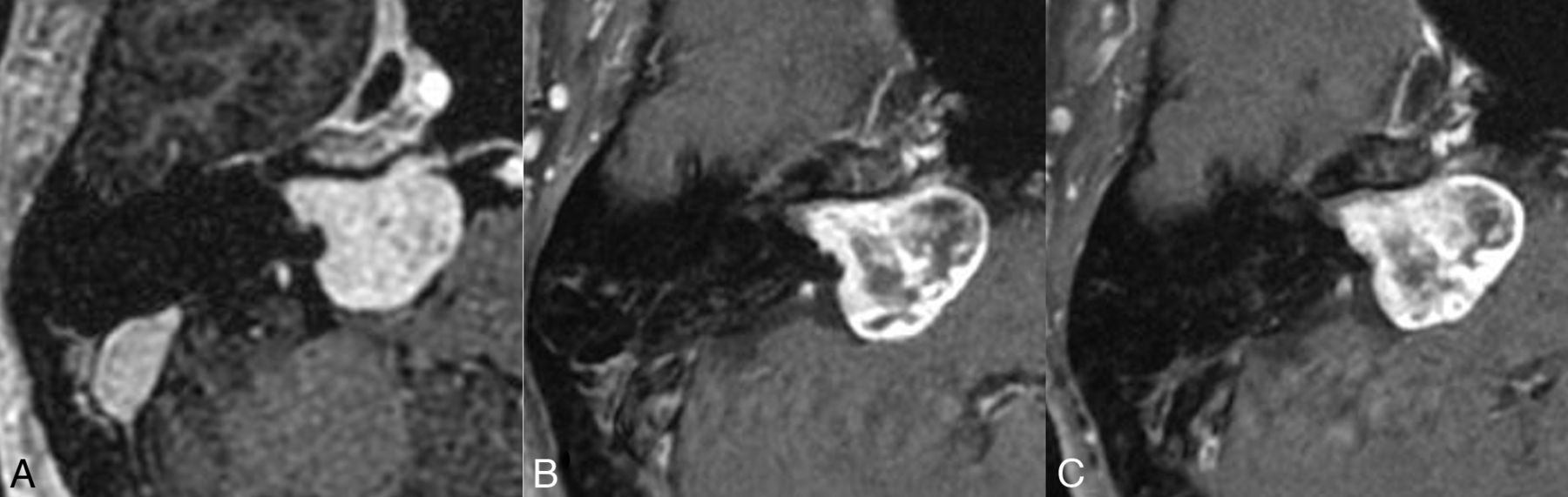
Tumor control post-SRS. Axial postcontrast images obtained pre-SRS (A) and at 1 (B) and 3 years (C) post-SRS show stable tumor size, despite considerable loss of central enhancement in the post-SRS period.

Treatment failure post-SRS. Axial postcontrast images obtained pre-SRS (A), and at 1 (B), and 2 (C) years posttherapy show a progressive increase in tumor volume from 1.9 mL at baseline to 3.2 mL at 2 years, accompanied by worsening disequilibrium clinically.
As noted earlier, tumors may also occasionally show a delayed pseudoprogression, and tumor enlargement within the first 3-4 years is generally not used as a sole criterion for salvage therapy.16 Because differentiation between tumor regrowth and delayed pseudoprogression may be challenging on conventional MR imaging, some authors recommend a documented increase in tumor size for 3 consecutive annual scans before adjudicating treatment failure, except in cases with new symptoms or larger tumors.11 Table 1 outlines the various forms of treatment outcomes that may be seen in VS post-SRS.
Treatment outcomes in VS post-SRS
Surrounding Parenchymal Changes
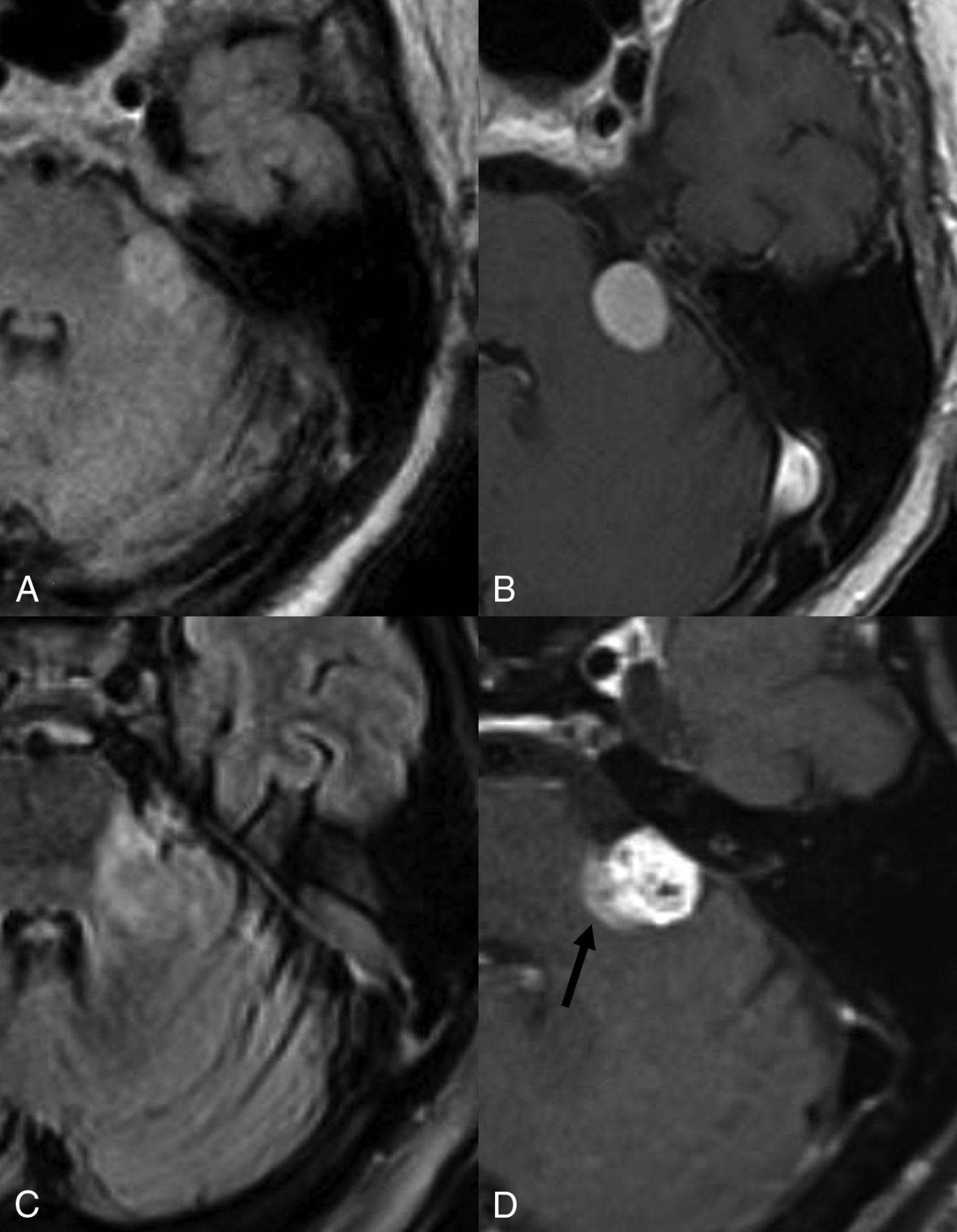
Development of peritumoral edema postradiosurgery is well-recognized with meningiomas and has been reported in 28%–50% of cases.21 Similar changes may also be observed along the pons and cerebellar peduncles in patients with VSs treated with SRS and have been reported in about 24% of patients, developing at a median of 6 months postradiosurgery (range, 4–24 months).9 These may be associated with contrast enhancement and generally resolve on follow-up imaging (Fig 6). The exact etiology is unclear but is presumably related to radiation effects, given the temporal association with SRS. Hayhurst et al9 noted that the development of edema was significantly associated with nonauditory complications such as hydrocephalus (6%), ataxia (12.5%), trigeminal (21%) or facial nerve dysfunction (3.75%) (P = .001, OR = 7.27; range, 2.33–22.66). Overall, there is scarce literature on these findings, which may not always be clinically symptomatic but can, nevertheless, be mistaken for inflammation and/or tumor extension into the inner ear structures.

Parenchymal edema and enhancement post-SRS. Axial FLAIR (A) and postcontrast (B) images show a left-sided vestibular schwannoma abutting the left brachium pontis without edema. Post-SRS, axial FLAIR (C), and postcontrast T1WI (D) reveal parenchymal edema (C) and enhancement (arrow, D).
Intracochlear hemorrhage secondary to SRS has been previously reported and is rare, generally presenting with acute onset hearing loss.22 Additionally, an increased dose to the cochlea may be associated with post-SRS hearing loss, and keeping the cochlear radiation dose below 4 Gy when possible is generally recommended.23
Development of Cysts Post-SRS
Intra- or peritumoral cysts may occur de novo, or enlarge post-SRS, with the incidence of delayed cyst formation reported at about 2.3% (Online Supplemental Data).24⇓-26 The thin-walled peritumoral cysts may histopathologically demonstrate arachnoid cells without any tumor cells.26 Enlarging or symptomatic cysts (secondary to mass effect) may require surgical decompression or may spontaneously regress with time.27
Contrast Leakage
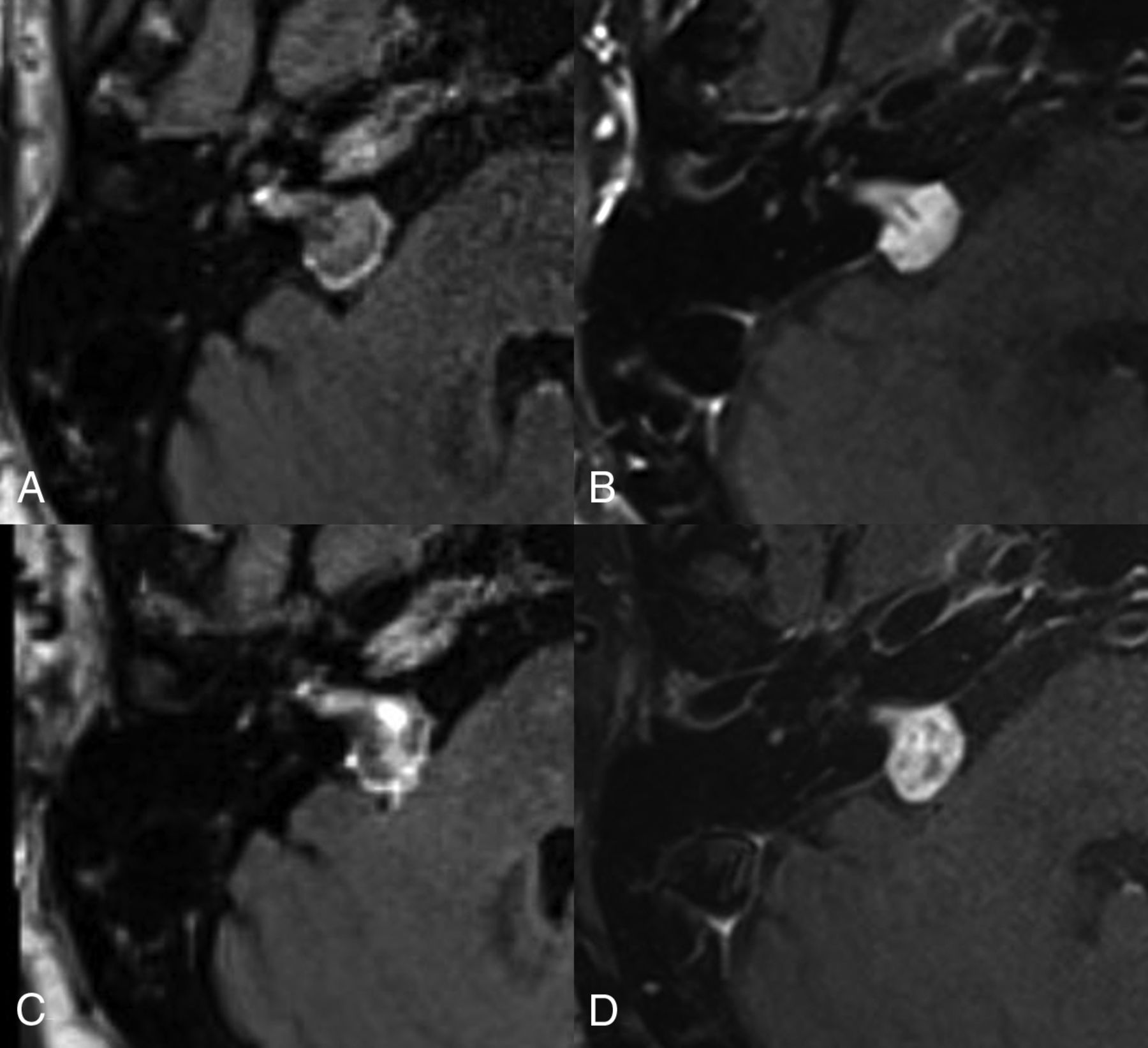
Peripheral contrast leakage, manifesting as a peritumoral halo may be seen in about 90% of patients with treatment-naïve VS. In such cases however, the contrast is only seen along the periphery of the VS.28 In our experience, early or delayed intratumoral contrast leakage in VSs treated with SRS may also be seen in a large percentage of cases (Fig 7). The exact incidence or clinical relevance of the latter remains unclear, but the phenomenon is likely secondary to slow diffusion of the contrast into the necrotic/extracellular spaces. Similar findings have also been described in metastatic brain lesions post-SRS as well as in cardiac imaging.29 On imaging, this may manifest as increased signal within the tumor core on post-contrast FLAIR images as well as increased extracellular, extravascular gadolinium in the internal auditory canal and vicinity of tumor. Whether this intra- or peri-tumoral contrast leakage correlates with elevated CSF protein post-SRS remains unclear.

Contrast leakage post-SRS. Axial postcontrast FLAIR (A and C) and T1WI (B and D) obtained pre- (A and B), and 1 year post-SRS (C and D). On the pre-SRS images, there is a thin peritumoral halo on the FLAIR imaging (A) without any contrast leakage centrally. Post-SRS FLAIR (C) shows contrast leakage within the VS more centrally.
Hydrocephalus
Even though hydrocephalus may be seen with untreated VSs in about 3.7%–18% of cases, it may additionally develop post-SRS in 2%–3% of patients (Fig 8).30⇓-32 The precise causal relationship remains controversial, and potential mechanisms include obstruction of the fourth ventricle, protein shedding from the tumor leading to plugging of arachnoid granulations, as well as alterations in CSF flow dynamics in the basal cisterns.30,32,33 Patients may develop communicating hydrocephalus 4–18 months post-SRS and often show elevated CSF protein levels and may have normal opening pressure.30,33 Risk factors include larger tumor size and female sex.34

Hydrocephalus post-SRS. Axial postcontrast images at the level of third ventricle (A–C) and the VS (D–F) obtained at baseline (A and D), at 1 (B and E) and 2 years (C and F) post-SRS show progressive enlargement in ventricular dimensions and disproportionate enlargement of left Sylvian fissure. The underlying VS (D–F) remained stable in size and showed loss of central enhancement. The patient was diagnosed with normal pressure hydrocephalus and underwent ventricular shunting.
Patients may also present with signs of elevated intracranial pressure or gait disturbances and urinary incontinence as seen with normal pressure hydrocephalus.35 Surgical CSF diversion may be required in most patients to alleviate symptoms.31 Table 2 summarizes the various reported post-SRS complications in patients with VS.
Post-SRS complications in patients with VS
Tumors Post-SRS
The risk of a secondary malignant CNS tumor developing post-SRS is considered low, with the overall risk estimated at approximately 0.04% at 15 years.36 However, these can, nevertheless, still occur and should be carefully considered, especially in young patients and those with underlying tumor-predisposition syndromes such as neurofibromatosis.37
Tumors reported post-SRS include malignant gliomas (including astrocytoma, glioblastoma, and ependymomas), sarcomas, meningiomas, as well as dedifferentiation of primary VS into malignant nerve sheath tumor. In the context of VS, malignant nerve sheath tumor and glioblastoma appear to be overall more common (Figs 9 and 10).36,37

Glioblastoma post-SRS. Axial postcontrast, pretreatment images reveal a left VS (A). The post-SRS left temporal lobe at 2 years (B) is without any lesions. The patient subsequently presented with seizures 3 years post-SRS with a new left temporal intra-axial mass on imaging (C), which was subsequently resected and diagnosed as a glioblastoma.

Malignant transformation of a VS post-SRS. Pre-SRS (A) contrast-enhanced image shows a left-sided VS. Post-SRS image after 5 years (B) shows a mild overall increase in tumor size. However, the tumor showed increased growth at 7 years post-SRS (C). A subtotal resection was performed (D), and pathology revealed a malignant peripheral nerve sheath tumor. Follow-up imaging after 4 months (E) shows considerable recurrent tumor burden with involvement of adjacent structures.
The mean latency period for stereotactic radiosurgery–induced neoplasms is about 7.9 years and is generally shorter for malignant neoplasms (7.1 years) compared with benign secondary neoplasms (14.25 years). Secondary neoplasms may occur either inside or outside the original lesion, as well as in regions receiving high- or low-dose radiation. The size of the original tumor often tends to be >2 cm.36,37
CONCLUSIONS
Post-SRS VSs can present with a variable appearances, besides the rare occasional complications such as secondary tumor and hydrocephalus. Familiarity with the various imaging findings may be helpful to avoid incorrect interpretation and recognize early complications.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 28, 2023.
- Accepted after revision January 3, 2024.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}