
Abstract
BACKGROUND AND PURPOSE: Although spinal root abnormalities are known to occur, spinal MR examination is seldom performed in hereditary motor and sensory neuropathies (HMSN). The following work was undertaken to assess the MR imaging spectrum of lumbosacral spinal nerve root abnormalities and determine whether intradural nerve root involvement could be related to any biopsy feature.
METHODS: Ten consecutive patients (eight male, two female; age range, 28–65 yrs) with Charcot-Marie-Tooth (CMT) (type I = 5, type II = 2) and Déjèrine-Sottas disease (DSD) (n = 3) underwent a contrast-enhanced lumbosacral MR examination. Sural nerve biopsy was perfomed in all patients. Atypical clinical features were present in two patients. The MR scans of each patient were reviewed for possible causes of myeloradiculopathy, spinal nerve root and ganglia dimensions, signal change, and abnormal enhancement.
RESULTS: In the seven patients with CMT, abnormal MR findings were intradural nerve root hypertrophy (n = 2), signal abnormalities (n = 2), and enhancement (n = 3). Two of three patients with DSD had the abnormal MR finding of intradural nerve root enhancement. In both patients with atypical clinical features, MR imaging showed nerve root hypertrophy and enhancement. Both findings were related to an increased number of onion bulbs at sural nerve biopsy. Inflammatory infiltrates were not observed in any patients.
CONCLUSION: In patients with HMSN enhancement of intradural spinal nerve roots, whether or not associated with marked thickening, may be found on lumbosacral MR examinations. Spinal nerve root thickening may be responsible for atypical symptoms, and its visibility on MR images represents a useful adjunct to diagnosis. Lumbosacral spinal nerve root abnormalities were related to an extremely high number of onion bulbs (indicating active demyelination) at sural nerve biopsy. Nerve root enhancement does not seem to be related to inflammatory infiltrates.
Hereditary motor and sensory neuropathies (HMSN) are a heterogeneous group of genetically determined peripheral neuropathies characterized by symmetrical and predominately distal motor and sensory disturbances and a slowly progressive course. Charcot-Marie-Tooth (CMT) type I and Déjèrine-Sottas disease (DSD) are the disorders most characteristically associated with marked thickening of peripheral nerves (hypertrophic neuropathies). Diagnosis is founded on familial history, clinical-laboratory data, electromyography and nerve conduction studies, sural nerve biopsy, and molecular genetic studies. Spinal nerve root abnormalities have been described in patients with HMSN. MR imaging is a noninvasive tool for in vivo study of the cauda equina nerve roots, and although occasional reports on the utility of spinal MR examination have been published (1–4), spinal root involvement in these disorders has not been widely discussed.
We performed lumbosacral MR examinations in a series of patients with HMSN to assess the spectrum of intradural nerve root abnormalities. Correlations between MR findings and sural nerve biopsies were obtained to determine whether intradural nerve root involvement could be related to biopsy features.
Methods
From January 1998 to March 1999, 10 consecutive patients (eight male, two female; age range, 28–65 yrs) with HMSN (type I = 5, type II = 2, and type III = 3; mean follow-up period, 6.3 yrs) underwent plain and contrast-enhanced MR imaging of the lumbosacral spine. All clinical data were obtained from examination of the clinical charts. In all patients, both light (LM) and electron microscopy (EM) were performed on sural nerve specimens. In patients with type I-II HMSN, diagnosis was confirmed with molecular genetic investigations. Two patients with CMT I suffered from progressive urinary bladder dysfunction and severe low back pain. These clinical features are not usually present in HMSN and were considered atypical. Palpable peripheral nerve enlargement was not present in any patient. All patients with clinical and/or laboratory suspicion of a concomitant inflammatory or infectious polyneuroradiculopathy were excluded. Two patients with type III HMSN were in the “classical” or “juvenile” form, and one had the “congenital hypomyelinating” form.
MR examination of the lumbosacral spine was performed on a superconducting 1.5-T unit with a linear surface coil. All patients underwent the same study protocol: sagittal spin-echo (SE) T1-weighted 500/15/2 (TR/TE/excitations), then sagittal and axial fast spin-echo (FSE) T2-weighted 4000/120/4 acquisitions with an echo train length of 16, followed by postcontrast sagittal, axial, and coronal SE T1-weighted 500/15/2–4 acquisitions. IV injection of paramagnetic contrast medium was performed at a 0.1 mM/kg dose. Section thickness was 3–4 mm for sagittal and coronal scans and 5–6 mm for axial scans. Field of view was 30–35 cm for sagittal and coronal acquisitions and 20–25 cm for axial scans. The acquisition matrix was 256 × 192 pixels. A fat saturation technique (spectral presaturation with inversion recovery [SPIR]) was performed during at least one of the postcontrast SE T1-weighted imaging sessions.
Hard copies of MR examinations were reviewed in a non-blinded fashion by two observers for the following findings: possible causes of myeloradiculopathy, intra- and extradural spinal root and ganglia dimensions, and signal change and enhancement. MR imaging findings of the lumbosacral spine in five healthy subjects were available for comparison. Histologic specimens from sural nerve biopsy were evaluated by a neurophatologist (GM) for the following findings: reduction of myelinated fibers, amount of onion bulbs, collagen tissue, and cellular infiltrates. Each abnormality was classified as slight (+), moderate (++), severe (+++), and marked (++++).
Results
An overall schematic representation of microscopic and MR findings is reported in the Table.
Correlations between pathologic features from sural nerve biopsy and lumbosacral MR examination
MR Imaging Findings
Type I HMSN
In two patients (case 1 and 5), plain and contrast-enhanced MR examinations were negative. In two patients (case 3 and 4), the plain sagittal scans revealed a large soft-tissue mass with polylobulated margins, showing low-to-medium signal intensity on SE T1-weighted and medium-to-high signal intensity on FSE T2-weighted images in the region of the cauda equina (Fig 1A). Thickened intradural nerve roots showing medium-to-high signal intensity were confirmed on the axial FSE T2-weighted images. The roots of the cauda equina were packed together, mimicking a subarachnoid block at the L2–L3 level (Fig 1B). Nerve root enlargement extended to the spinal ganglia and the lumbosacral plexus. Marked enhancement of intra- and extradural nerve roots occurred in both patients on postcontrast SE T1-weighted images (Fig 1C–E). Intradural nerve root enhancement was also seen in one patient (case 2) in the absence of hypertrophic changes.

A–E, MR images of the lumbosacral spine in a patient with CMT I and atypical clinical features (case 3).
Marked thickening of spinal nerve roots, completely filling the spinal canal, is seen on the sagittal (A) and axial (B) FSE T2-weighted (4000/120 [TR/TE]) images. Enhancement of hypertrophic spinal nerve roots and ganglia (arrows) is depicted in the postcontrast SE T1-weighted (TR/TE) sagittal (C) and axial (D) images. A coronal SPIR (E) postcontrast SE T1-weighted scan better depicts spinal ganglia hypertrophy and enhancement by supppressing signal from the paravertebral and foraminal fat.
Type II HMSN
In both patients (case 6 and 7), the MR examination was negative.
Type III HMSN
In one patient with the classical form of HMSN (case 9), the contrast-enhanced MR examination was negative. In the other two patients (one with the classical form, one with the congenital hypomyelinating form), a slight but definite and homogeneous enhancement of intradural nerve roots was seen on postcontrast SE T1-weighted images (Fig 2A–D), in the absence of hypertrophic changes or signal abnormalities.

A–D, MR images of the lumbosacral spine in a patient with the congenital hypomyelinating form of DSD (case 8).
Marked diffuse enhancement of the cauda equina nerve roots in the absence of root enlargement is seen on pre- (A) and postcontrast (B) SE T1-weighted (500/15) sagittal images. Fat-suppressed (SPIR) coronal postcontrast T1-weighted image (C) enables better contrast between enhanced spinal ganglia (arrow) and surrounding fat-suppressed fat tissue signal compared with corresponding non-SPIR image (D).
Biopsy Findings
Type I HMSN
On LM, the extent of fibrotic abnormalities and number and size of onion bulbs varied considerably among patients. Reduction in the number of myelinated fibers correlated with disease duration and severity and was more marked in cases 3 and 4 (<2303/mm2), in which almost all fibers showed onion bulbs. Few residual fibers showed a thin myelin sheath, indicating remyelination. Axons appeared either normal or hypotrophic. Nerve fascicles showed variable hypertrophic changes, depending on the amount of onion bulbs, increase in endoneural collagen tissue, and amorphous protein precipitate resembling mucus on specific histochemical stains. An increase of fibroblasts and mastocytes was seen in the endonevrium in patients 2, 3, and 4 (Fig 3). On EM, onion bulbs showed the typical two-to-five concentric layered structure of overlapping, intertwined Schwann cells encircling thinly myelinated and demyelinated axons. In some onion bulbs, the axon was not visible (denervated onion bulb).

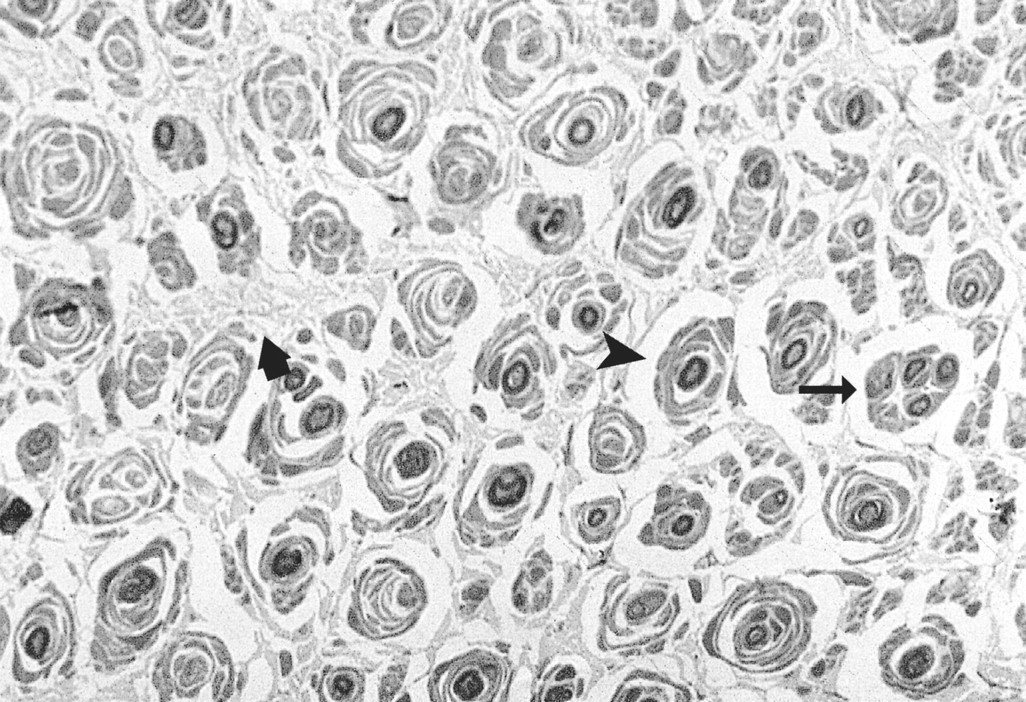
Light microscopy of the sural nerve specimen (Toluidin blue stain, semi-thin section) in a patient with CMT I and atypical clinical symptoms (case 3).
Almost all fibers show “onion bulbs” (black arrowhead), with an absence of myelinated fibers, indicating active demyelination. Clusters of regenerating fibers are indicated by thin black arrow and collagen hypertrophy by large black arrow.
Type II HMSN
Abnormalities were confined to a small proportion of fibers. On LM, only a slight reduction in the number of myelinated fibers was seen. Onion bulbs were rare. Several fibers showed a thin myelin sheath. EM demonstrated a certain amount of nonspecific axonal degeneration in both myelinated and unmyelinated fibers. Well-formed onion bulbs were absent.
Type III HMSN
In both patients with the “classical” form of type III HMSN, LM showed a significant reduction of myelinated fibers, irrespective of their diameter. The major part of the fibers showed either complete demyelination or thinning of the myelin sheath. Onion bulbs were numerous, and in patient 10, almost every myelinated fiber was surrounded by an onion bulb. On EM, typical onion bulbs were seen. Fibroblasts and mastocytes were present in the endoneural collagen in both patients. In the patient with the congenital hypomyelinating form of HMSN (case 8), an almost complete disappearance of myelinated fibers, with rare basal lamina onion bulbs, was observed on both LM (Fig 4A) and EM (Fig 4B), in the absence of cellular infiltrates.

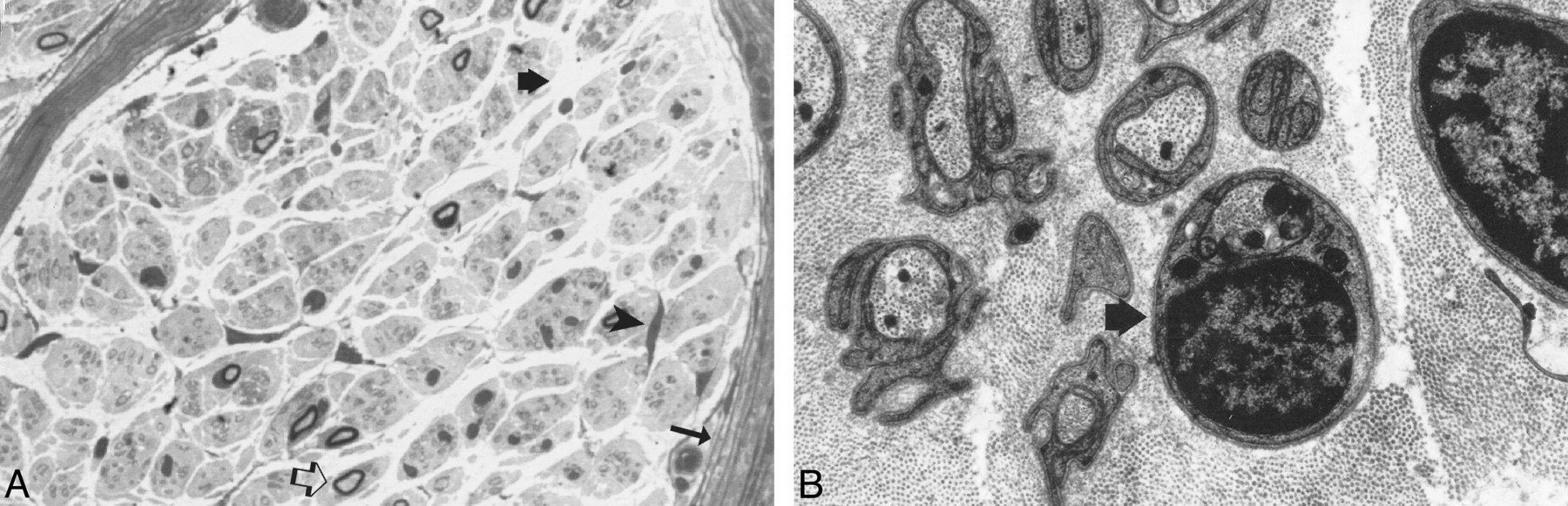
A and B, LM and EM of the sural nerve specimen (Toluidin blue stain, semi-thin section) in a patient with the congenital hypomyelinating form of DSD (case 8).
On LM (A), a decreased number of myelinated fibers with peri- and epineural connective tissue hypertrophy is noted (arrow). Very few residual thinly myelinated fibers (open black arrow) are observed. Note the absence of onion bulbs and connective tissue hypertrophy (thick black arrows) with fibroblasts (black arrowhead). On EM (B), complete absence of myelin sheaths around axons is seen. A Schwann cell nucleus is indicated by the arrow.
Discussion
Few reports describe the MR appearance of intradural nerve roots in HMSN, because MR imaging is considered to have no diagnostic role in these disorders. However, spinal nerve root abnormalities on MR images have been occasionally reported, and spinal cord impingement from enlarged intradural roots has been described in patients with CMT I and DSD (2, 4–5). In our series, we have encountered two situations in which MR imaging was deemed valuable. The first was characterized by patients with atypical symptoms in which lumbosacral MR imaging showed marked enlargement, signal change, and enhancement of intradural nerve roots. Because lumbosacral MR imaging showed neither disk nor degenerative disease and diabetes mellitus, chronic inflammatory demyelinating polyneuropathy, amyloidosis, acromegaly, and Refsum's disease were excluded, we suggested that spinal root abnormalities or cord compression secondary to marked nerve root enlargement may be responsible for the low back pain and bladder dysfunction. In these patients, MR imaging was a useful diagnostic test for revealing the possible cause of atypical symptoms and excluding other causes of nerve root or spinal cord compression.
The second situation was characterized by patients with the classical clinical syndrome and normal or diffusely enhancing intradural spinal nerve roots on MR images. In these patients, lumbosacral MR examination was performed to see if intradural nerve root abnormalities could also occur in the absence of atypical symptoms. Further studies of a larger group of patients are needed to determine whether a substantial proportion of patients with CMT and DSD have nerve root thickening and impingement or if this is just an unusual association.
HMSN have been classified by Dyck (6) into seven types (I–VII). Type I and II correspond clinically to CMT and type III to DSD disease. Peripheral nerve hypertrophy (noticeable sometimes by palpation) and “onion-bulb” changes in nerve fibers on microscopic examination are typical findings of type I HMSN. Differentiation between type I and type II HMSN is based on reduction of mean conduction velocity in the median or ulnar nerve: very marked (less than 38 mm/s) in type I and normal or slightly reduced in type II. The clinical manifestations in type III HMSN (recently classified also as “congenital dysmyelinating neuropathies”) begin usually earlier than do types I–II, and its course is more severe. Moreover, type III HMSN is usually associated with extremely high protein content in the CSF. Based on morphologic characteristics of the peripheral nerve, three subtypes of HMSN III are recognized: HMSN type III with amyelination (“congenital hypomyelinating neuropathy”), with basal lamina onion bulbs (“infantile form”), and with classical onion bulbs (the “classical” or “juvenile” form of DSD). HMSN type IV (Refsum's desease) is an autonomal recessive syndrome currently recognized to be caused by a defect in phytanic acid alpha oxidation. HMSN types V–VII are distinguished by the presence of spastic paraplegia, optic atrophy, and retinitis pigmentosa, in addition to HMSN features.
Although an exact correlation between MR imaging of the cauda equina and sural nerve biopsy specimens is difficult, it may be supposed that the pathologic process in these disorders extends diffusely to all peripheral nerves, including the lumbosacral intradural nerve roots. MR imaging may be considered an in vivo method for studying gross pathologic abnormalities. In patients with a history of hereditary polyneuropathy, macroscopic enlargement of peripheral nerves is present only in one of four patients with CMT I, which usually represents a late clinical finding. Interestingly, palpable peripheral nerves were not observed in any of our patients, and intradural nerve root thickening seen on MR examinations correlated with the amount of onion bulbs, increase in endoneural collagen tissue, and amorphous protein precipitate, causing a marked enlargement of nerve fascicles.
In our series, an abnormal enhancement of intradural nerve roots was also depicted on MR images of patients without atypical symptoms. Immunofluorescent studies of nerves from patients with hereditary and acquired peripheral neuropathies have shown plasma protein leakage, suggesting blood nerve–barrier damage (7, 8). This is also confirmed by the usually high CSF protein content, especially in patients with type III HMSN. Recently MR imaging has been employed to study nerve roots and peripheral nerves in the extremities (1, 2, 9). In particular, it has been reported that plain MR imaging may provide a useful method for detection of demyelinating-remyelinating processes in the sciatic nerve trunk of patients with type III HMSN (3). Experimental studies on rabbit sciatic nerves and rat peripheral nerves after crush injury, neurotomy, and/or nerve grafting seem to support this hypothesis (10). Moreover, it is well known that intradural nerve roots do not usually show any enhancement in healthy subjects because of an intact blood-nerve barrier, unless high doses of contrast medium (0.3 mM/Kg) are injected (11). In our series, diffuse enhancement of lumbosacral spinal roots on MR scans, even in the absence of hypertrophic or signal changes, correlated with the amount of onion bulbs, indicating active myelin breakdown and demyelination. Therefore, it is possible that at least in three patients with CMT I (case 2, 3, and 4) and in one patient with the classic form of DSD (case 10), abnormal intradural nerve root enhancement may be related to blood nerve–barrier damage secondary to active demyelination. Because no inflammatory infiltrates were observed in our series, it is unlikely that nerve root enhancement is caused by inflammatory blood nerve–barrier breakdown. Blood nerve–barrier breakdown is also described in amyloidosis, where it seems to be sustained by the perivascular deposit of amyloid in the absence of inflammatory infiltrates (12). Diffuse enhancement of the cauda equina was also depicted in the patient with the congenital hypomyelinating form of DSD (case 8). In this disease, by definition, a primary defect in myelin formation has been suggested, and demyelination is absent (3), as was supported by a lack of onion bulbs and preservation of axons. It is possible that in our patient a congenital defect of the blood-nerve barrier may also be present, as supported by the usually high CSF protein content in this disorder.
Differential diagnosis of diffuse intradural nerve root enlargement and enhancement include chronic inflammatory demyelinating polyneuropathy, meningeal carcinomatosis or lymphoma, amyloid neuropathy, leprosy, sarcoidosis, and neurofibromatosis. Simultaneous occurrence of neurofibromatosis and CMT disease has been reported in one patient, possibly representing a genetic linkage between these diseases (13). In fact, the gene for neurofibromatosis 1 has been linked to the pericentrometric region of chromosome 17, and the HMSN type I locus is linked to chromosomes 1 and 17. In our patients, however, the cutaneous stigmata of neurofibromatosis were not present, and family history was negative for such disease. Diffuse intradural nerve root enhancement can be also noted in acute and chronic inflammatory demyelinating polyneuropathies, infective polyradiculopathies such as cytomegaloviral AIDS-related polyradiculonevritis (14, 15), postsurgical arachnoiditis (16), and even after radiation therapy. Nerve root compression (eg, spinal stenosis and disk herniation) can disrupt the blood-nerve root barrier, also leading to abnormal enhancement. The latter, however, usually involves only a few nerve roots and in some cases it seems to be reversible, generally resolving in approximately 6 months (17).
Conclusion
Lumbosacral MR imaging of patients with HMSN show either: 1) marked thickening and enhancement of intradural nerve roots, possibly related to atypical clinical features, or 2) diffuse enhancement of the cauda equina nerve roots in the absence of any abnormalities on precontrast MR images. The former lumbosacral MR findings are useful for excluding other causes of nerve root or spinal cord compression. An extremely high number of onion bulbs, indicating active demyelination, correlate with spinal nerve root abnormalities. Nerve root enhancement is not related to inflammatory infiltrates, but rather may be related to blood nerve–barrier disruption from congenital and/or active demyelinating processes.
References
- Received November 1, 1999.
- Accepted after revision May 10, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}