
Article Figures & Data
Figures
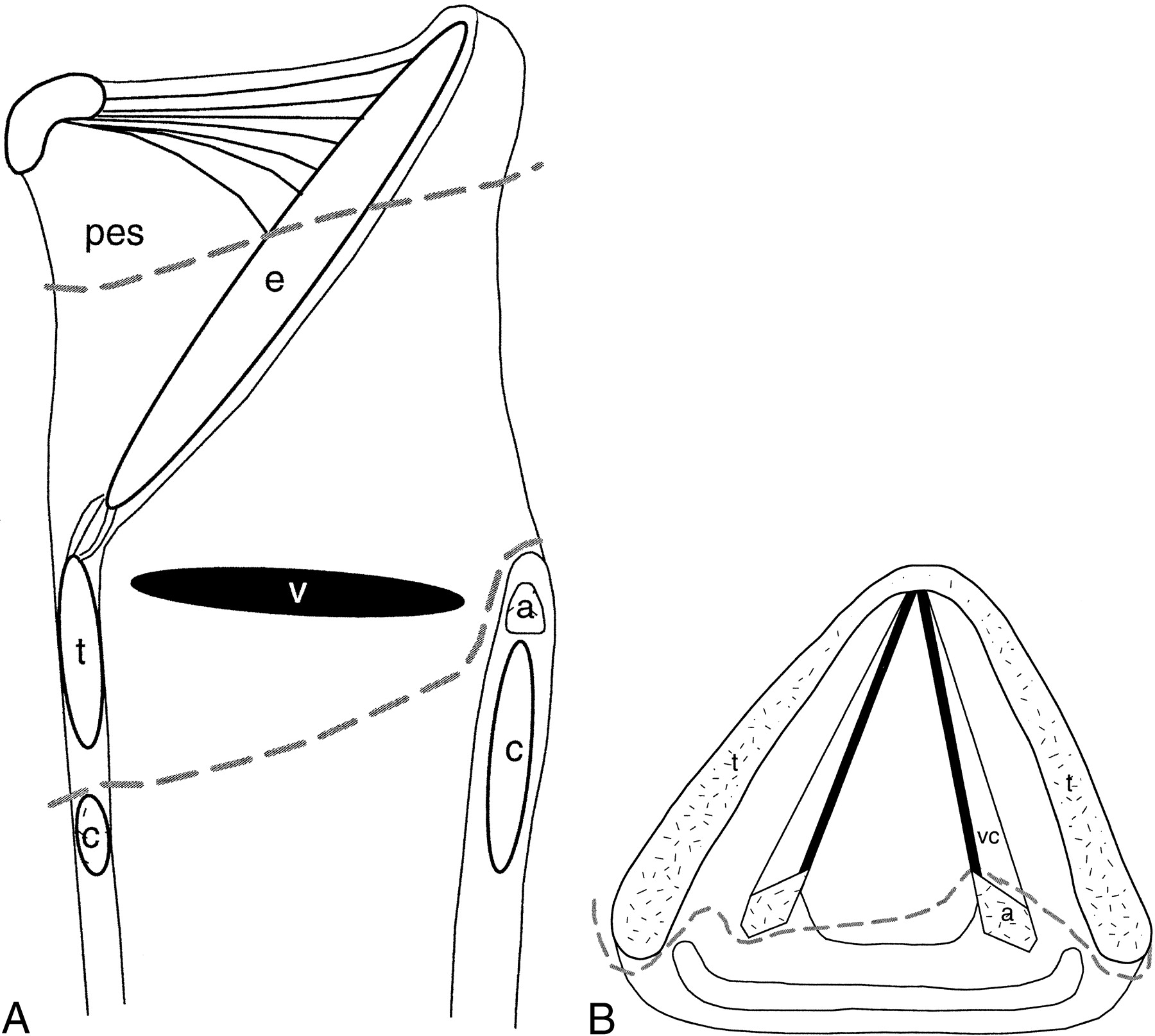
fig. 1. A and B, Sagittal and axial drawings of structures resected during CHP (dashed lines). pes indicates preepiglottic space; e, epiglottis; a, arytenoid; c, cricoid cartilage; v, ventricle; t, thyroid cartilage; vc, vocal cords
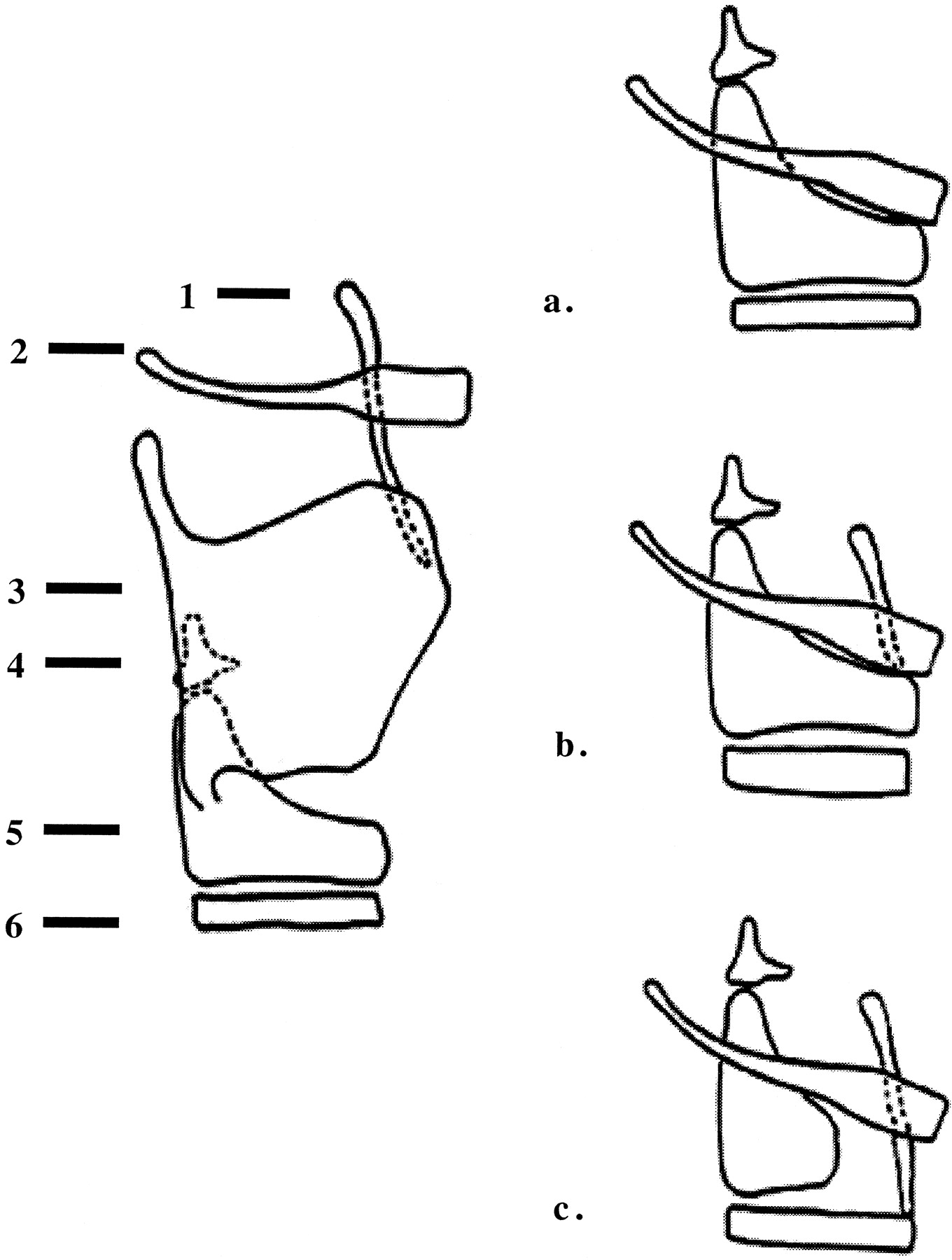
fig. 2. Types of reconstruction with SCPL. 1 indicates epiglottis; 2, hyoid bone; 3, thyroid cartilage; 4, arytenoid cartilage; 5, cricoid cartilage; 6, tracheal ring.
A, CHP.
B, CHEP.
C, TCHEP.
fig. 3. A and B, Sagittal and axial drawings of structures resected during CHEP (dashed lines).
Note.—pes indicates preepiglottis space; e, epiglottis; a, arytenoid; c, cricoid cartilage; v, ventricle; t, thyroid cartilage; vc, vocal cords.
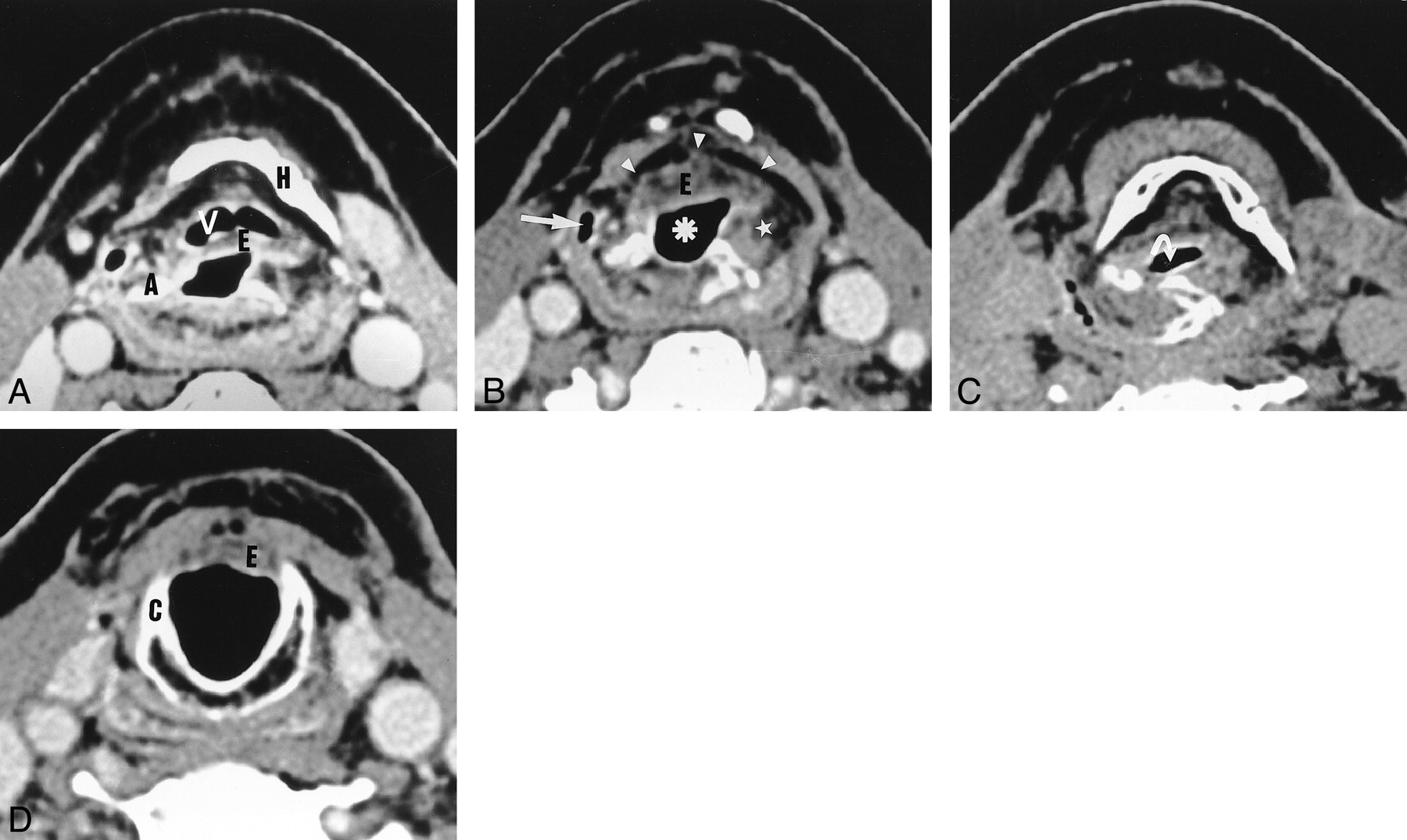
fig. 4. Axial CT scans obtained after SCPL with CHEP.
A, The vallecula (V) and epiglottis (E) are depicted at the level of the hyoid bone (H).
B, Below the level of the hyoid bone, the neovestibule (asterisk) is limited anteriorly by the epiglottis (E) and laterally by the NAFs (star). The lateral recess of the hypopharynx (arrow) and the preepiglottic space (arrowheads) are depicted.
C, During phonation, the neoglottis is oval and transversally oriented (arrow).
D, At the level of the cricoid cartilage (C), the subglottic lumen is empty and outlined by a thin mucosa. The inferior border of the epiglottis (E) cannot be distinguished.
fig. 5. Axial CT scans obtained after SCPL with CHEP.
A, Hyoid bone (H), epiglottis (E), and neoaryepiglottic fold (star).
B, Slightly lower image shows that the left arytenoid has been resected and replaced by an exessive soft tissue (star). The right arytenoid (A) is depicted.
C, At the level of the cricoid cartilage, the excessive soft tissue is visible in the subglottic lumen (arrow). A slightly thickened aspect of the mucosa covering the cricoid cartilage is depicted (arrowhead).
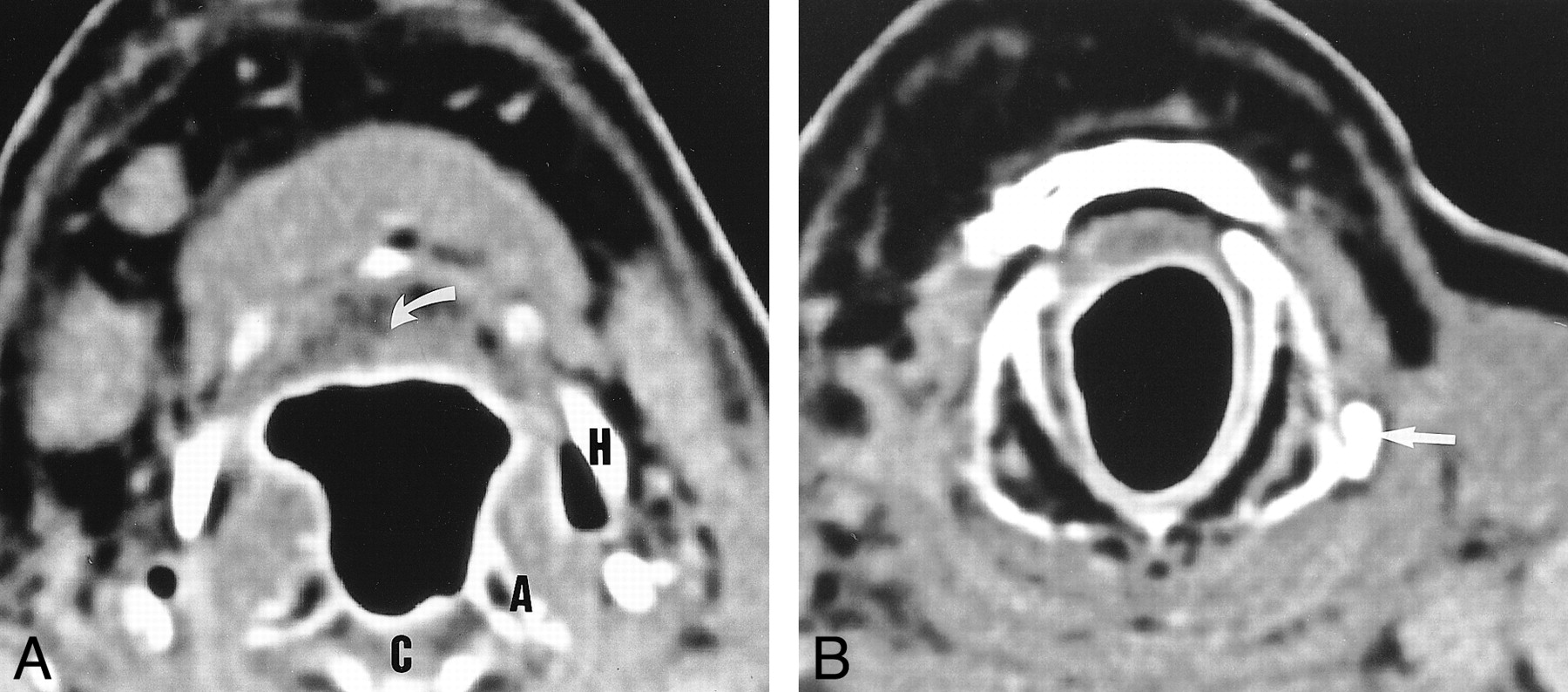
fig. 6. Axial CT scans obtained after SCPL with CHEP below the level of the hyoid.
A, The lateral recess of the hypopharynx is virtual (arrow).
B, During the Valsalva maneuver, the recess unfolds completely. Its medial limit is the neoaryepiglottic fold, which is thickened and slightly heterogeneous.
fig. 7. Axial CT scans obtained after SCPL with CHP.
A, Soft tissue (arrow) corresponding to the base of the tongue is depicted behind the hyoid bone (H) instead of the epiglottis and valleculae. The pexis projects the arytenoids (A), upper border of the cricoid cartilage (C), and hyoid bone (H) to the same level.
B, At the level of the cricoid cartilage, the mucosa is thin and regular. The left inferior horn of the thyroid cartilage has been spared (arrow). The right horn is not visible.
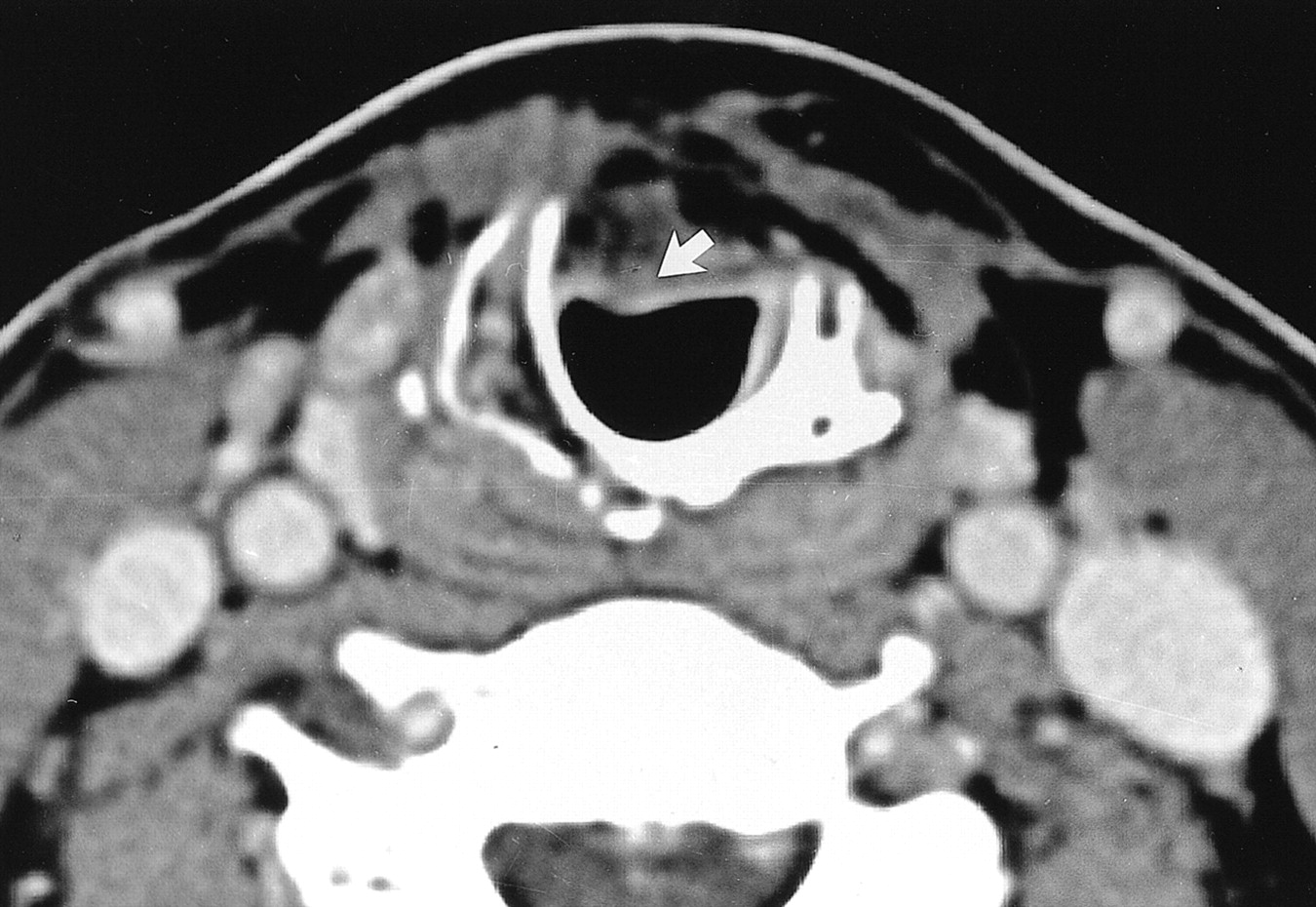
fig. 8. Axial CT scan obtained after SCPL with TCHEP. The anterior arch of the cricoid cartilage has been resected. Therefore, the remaining epiglottis (arrow) is anchored to the first two tracheal rings
fig. 9. Axial CT scans of recurrrent disease in a patient who underwent SCPL with CHEP 2 y before.
A, Image depicts strong enhancement (star) of the right NAF compared with that of the left. This finding is very suggestive of recurrence.
B, The enhancement follows the lateral wall of the neovestibule (arrowheads). C, The enhancement proceeds down to the cricoid cartilage mucosa, which is thicker than usual (straight arrow), with the extralaryngeal spread of tumor (curved arrow).
fig. 10. Axial CT scans of recurrence 3 y after SCPL with CHP.
A, Enhancement of the right lateral wall of the neovestibule (arrows).
B, Enhancement spreading downward to the submucosa of the cricoid cartilage (arrow). C, Enhancement extending upward to the right side of the base of the tongue (arrow).
fig. 11. Axial CT scans in a patient who underwent SCPL with CHEP 5 y before. At nasofibroscopy, the patient had an anterior cervical cutaneous fistula with an arytenoid that was only slightly thickened.
A, Massive extralaryngeal recurrence around the cricohyoidopexy (arrows).
B, Recurrence spreading downward to the pretracheal tissue (stars).
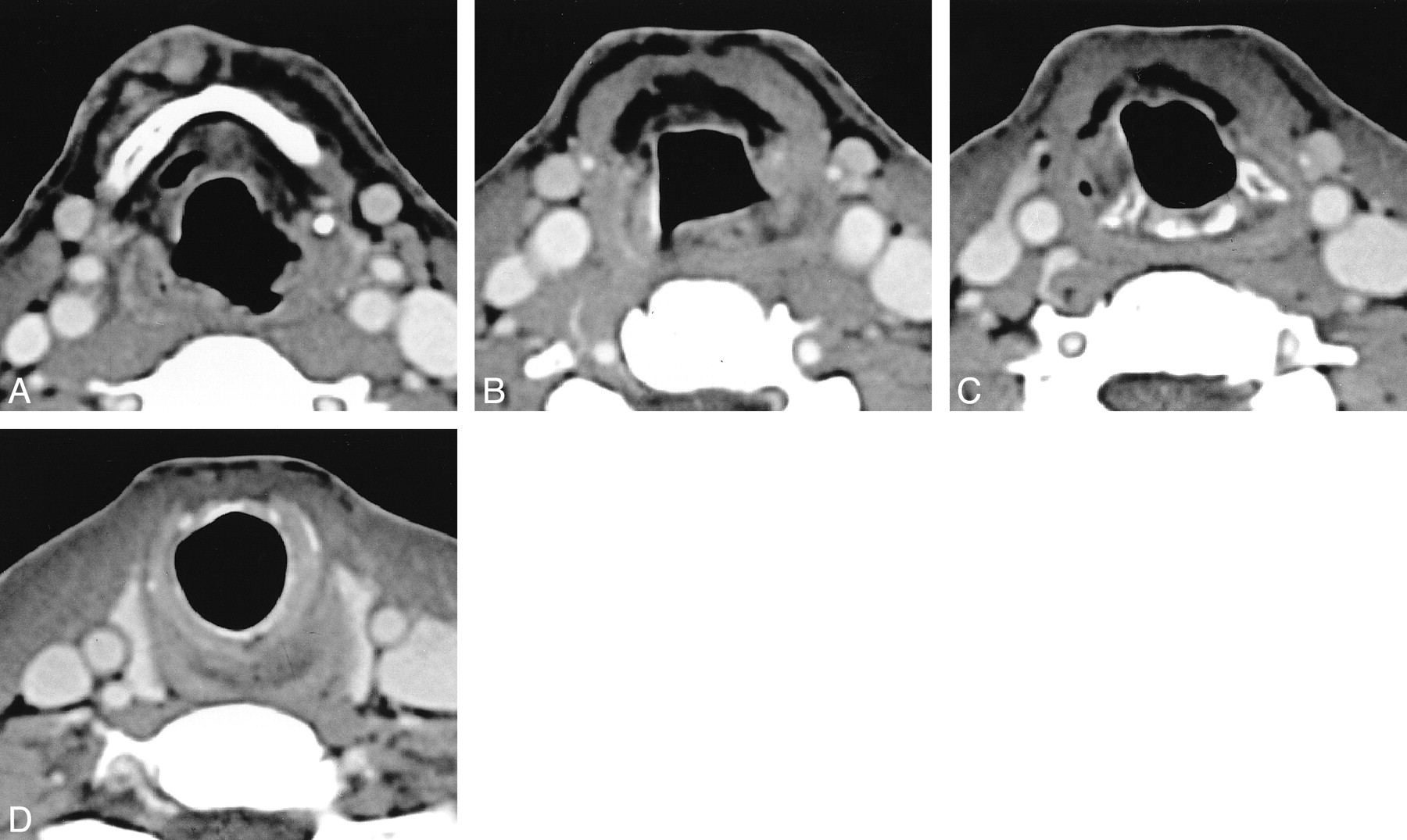
fig. 12. Axial CT scans obtained 6 mo after SCPL with CHEP in a patient with severe swallowing disorders. The distance between the lower limit of the hyoid bone (in A) and the lower limit of the cricoid cartilage (in D) is more than 3.5 cm. This finding implies failure of the pexis, which was confirmed at surgery

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}