
Abstract
Summary: A 49-year-old woman with a direct posttraumatic carotid cavernous fistula (CCF) was treated with detachable balloons via a transcarotid route. After the procedure, her intracranial bruit, conjunctival injection, and orbital congestion were cured, but the preexistent sixth nerve palsy deteriorated.
CT showed one balloon positioned in the posterior portion of the right cavernous sinus and was regarded to be responsible for nerve compression. After surgical exposure by use of a transnasal-transsphenoidal approach under 3D navigation control, this balloon was deflated by puncture with a 22-gauge needle.
The previously described symptoms resolved after balloon deflation. This report presents a rare complication of endovascular treatment of direct CCF and a new microsurgical approach to a balloon in a case of nerve compression.
Direct carotid cavernous fistulas (CCFs) (Barrow Type A) are high-flow shunts between the cavernous portion of the internal carotid artery (ICA) and the cavernous sinus (CS) and are usually caused by traumatic laceration of the ICA (80%) or rupture of a preexisting aneurysm of the ICA (1). The clinical symptoms are visual blur, diplopia, headache, ocular pain, and bruit designation. The clinical signs can develop weeks after injury.
Transarterial balloon embolization with or without preservation of the carotid artery or by a transvenous approach is the treatment of choice and is associated with limited morbidity and the least damage of cranial nerves (2). A strayed, overinflated, or dislodged balloon can cause neurologic deterioration attributable to a reopened fistula or local compression of cranial nerves (3, 4).
We describe a new technique for clearing a sixth nerve palsy after ballooning of an arteriovenous fistula. To our knowledge, a computer-navigated puncture of a balloon by use of a transnasal-transsphenoidal approach has not been previously reported.
Case Report
A 49-year-old woman presented with conjunctival injection of both eyes; mild, right sixth nerve palsy; and decreased visual acuity of the right eye. There was a history of head trauma with amaurosis on the left eye 4 months prior. Initial CT scanning showed a skull base fracture and multiple cerebral contusions. Doppler sonography showed an increased blood flow through the right ICA (4.5/3.0 kHz right side versus 2.5/1.2 kHz left side).
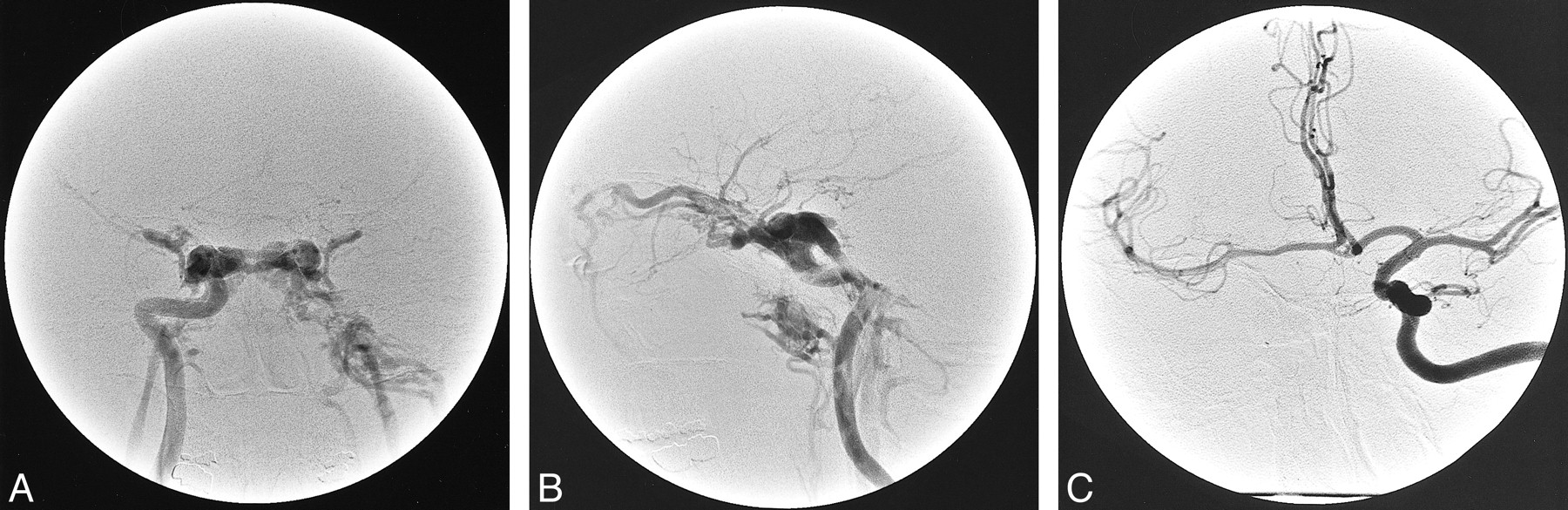
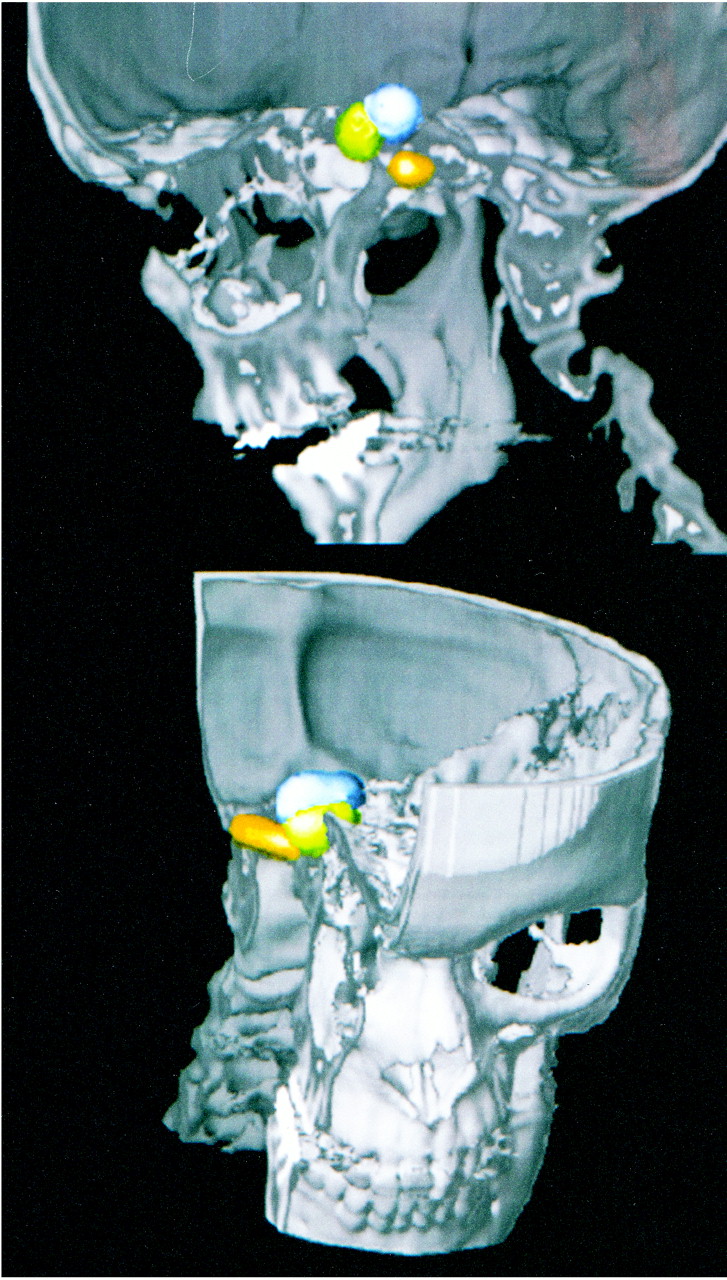
Cerebral angiography revealed a right-sided direct CCF draining mainly by the superior ophthalmic vein, the petrous sinus, cortical veins, and predominately the contralateral CS (Fig 1). A definitive closure of the fistula without occlusion of the ipsilateral ICA was impossible. Therefore, the three detachable silicone balloons occluded the fistula and the ipsilateral ICA. Two balloons were located within the extremely dilated CS, and one was in the ICA below the fistula (Fig 2). After the intervention, the bruit heard behind the right ear, the conjunctival injection, and orbital congestion were cured, but the preexistent, incomplete sixth nerve paresis had progressed to a complete state. On cranial CT scans, the balloons were located in the anterior and posterior portion of the right CS, and we assumed that the posterior balloon was overinflated.

A, Angiogram of right ICA before embolization (anteroposterior view, early arterial phase) shows huge CCF and no opacification of intracranial vessels.
B, Lateral angiogram of the right ICA shows CCF drainage by the right superior ophthalmic vein, both CS, the inferior petrosal sinus, and pterygoid sinus.
C, Left ICA angiogram before embolization (anteroposterior view, early arterial phase) shows cross flow via the anterior communicating artery.

The anatomic location of the detached balloons shown by CT (3D view)
The patient underwent general anesthesia, and a balloon incision was performed by a microscopic endonasal, transseptal, and transsphenoidal computer-navigated approach.
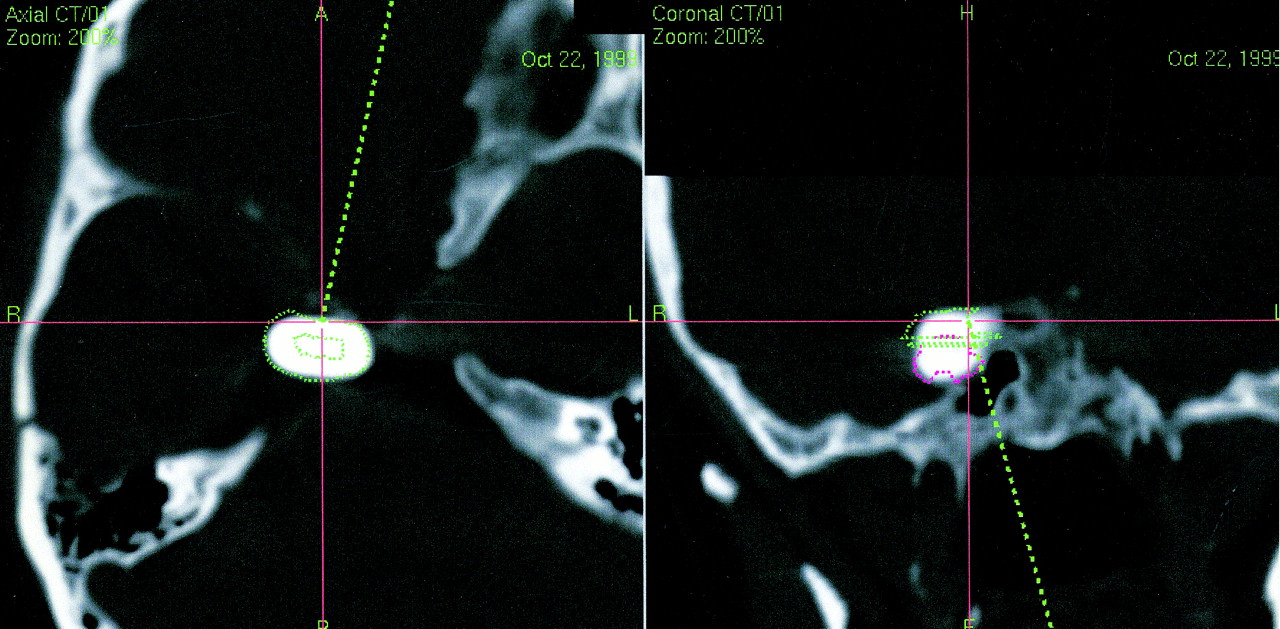
For navigational purposes, spiral CT was performed with a slice thickness of 1 mm, a table feed of 2 mm/tube rotation, and a reconstruction interval of 1 mm at 140 kV and 130 mA (scanner: GE ProSpeed SX Power; GE Medical Systems, Milwaukee, WI). We used a standard reconstruction algorithm at a 360° linear interpolation. The dataset was transmitted to the navigation system (systems: STN Zeiss-Leibinger and Zeiss OPM Neuro Navigation Microscope NC4, Germany), and 3D views were constructed on a workstation (Sun Ultrasparc 2; Sun Microsystems, Santa Clara, CA) with Advantage Windows 3.1 (GE Medical Systems, Buc, France) (Fig 2). The balloon was marked in the navigated CT scan. The patient's head was fixed in a Mayfield clamp to control head motion.
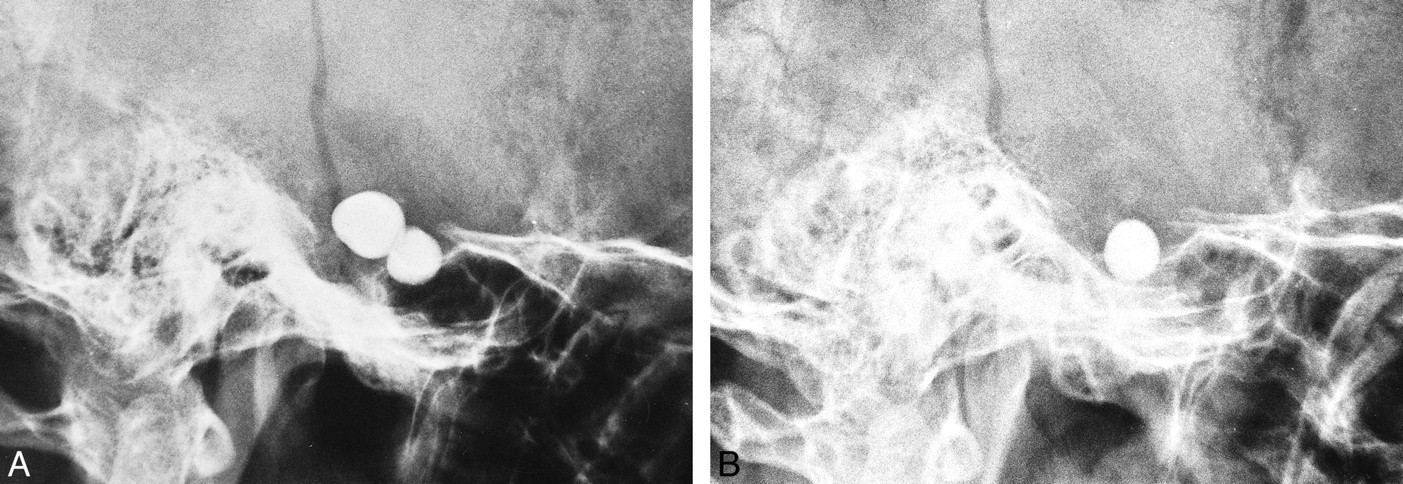
After vasoconstriction, a vertical incision into the mucosa of the nasal septum was performed to prepare for a bilateral mucoperichondrial flap up to the anterior wall of the sphenoid sinus. For a better overview of the sphenoid sinus, the posterior wall of the septum was reduced, and the entrance of the sphenoid sinus was enlarged. The mucosa of the sphenoid sinus was preserved. The pointer of the navigation system showed the area of the posterior wall of sphenoid sinus, where the bone had to be opened (Fig 3). The indicated part of the posterior bony wall of the sphenoid sinus was reduced, and the balloon was localized in the posterior part of the CS. The balloon was punctured with a 22-gauge lumbar puncture cannula, and contrast agent was aspirated and controlled by X-ray to differentiate from CSF. To close the fault of the posterior wall of the sphenoid sinus, a lateral pedunculated mucosal flap of the nasal cavity was prepared. The resected cartilage was reimplanted into the septum, the mucosa incision of the vertical septum was closed by two 4/0 sutures, and a bilateral mucoperichondrial flap was adapted by bilateral packs for 2 days. The procedure was documented by X-ray of the head before, immediately after, and 1 week after deflation of the balloon (Fig 4).

CT navigation for surgery focuses the pointer on the area of the posterior wall of the sphenoid sinus, where the bone was opened

A and B, X-ray documentation of the two balloons located in the CS and ICA at the fistula site (A, before treatment; B, control taken 7 days after balloon puncture). The third balloon in the petrous segment of the ICA is superimposed by skull base structures (see figure 2)
After 8 weeks, the sixth nerve palsy resolved, and follow-up Doppler sonography at 6 weeks showed no clinical signs of CCF recurrence.
Discussion
The structures lying within the CS are surrounded and contained within a membranous structure. The inferior and medial membrane is composed of periosteum and is contiguous to the periosteal layer of dura covering the middle fossa and sella turcica. The superior and lateral portion of the membranes are contiguous to the connective tissue sheaths of cranial nerves II, IV, and V and may indirectly affect the course of cranial nerve VI (crossing the ICA and entering the superior orbital fissure beneath the ophthalmic division of the trigeminal nerve). Thus, increased pressure within the CS (caused by tumor, dural fistula, direct CCF, thrombosis of the CS, or a balloon) may affect some or all of these structures.
The endovascular cure of CCF is possible in up to 77% to 88% of cases (5). True anatomic compartments of the CS, which are rare, may limit options for definitive endovascular therapy (6). Third and sixth nerve palsy after endovascular treatment have been reported previously. In Debrun's experience (2) there was a 30% incidence of transient ophthalmoparesis, which is usually attributable to cranial nerve VI dysfunction (7).
In our patient, there was a high-flow shunt through a large tear in the posterior wall of the ICA at the C3–C4 segment. The ICA distal to the CCF was obliterated after trauma, and there was no supply from the external carotid artery. The collateralization from the left ICA was sufficient. A definitive closure of the fistula by the venous route or by the arterial route without occlusion of the ICA was impossible, because the high flow through the large tear in the ICA led to an unstable balloon placement in the CS, indicating a high risk of possible fatal balloon migration through the draining veins. Only closure of the CS together with closure of the ICA led to a stable closure of the large tear. Therefore, the fistula and the ipsilateral ICA were occluded by three detachable silicone balloons. Placement of one balloon at the fistula site failed because of the high shunt volume. However, two balloons were placed into the extremely dilated CS (Fig 2): the first one in the posterior part of the CS for stabilization and the second at the fistula site.
After closure of the fistula, the majority of patients with generalized ophthalmoplegia regained complete ocular movements rapidly, whereas patients with an isolated abduction weakness required more time to return to normal (7). Bavinszski et al (8) reported that in one case extended thrombosis of an enormously dilated superior ophthalmic vein occurred after treatment of a giant longstanding fistula, leading to unilateral visual impairment and increased cranial nerve VI palsy.
Balloon dislocation to the venous side has been described as a reason for reopening of the fistula, leading to worsening symptoms (9). A stray balloon is reported in fewer than 2% of cases (8). Sencer et al (10) described a case of balloon migration within the proximal portion of the superior ophthalmic vein and the management of this rare complication by use of a percutaneous CT-guided transorbital puncture. Detection of additional injury to cranial nerves may be difficult, because ophthalmoplegia is associated commonly with traumatic CCF. Although in most instances the worsening of ophthalmoparesis is temporary and requires no specific treatment, in our case, we believed it was necessary to try to deflate one of the balloons. There was an additional amaurosis on the left eye caused by the head trauma that occurred 4 months earlier and after endovascular treatment, there was no decreased right cranial nerve VI palsy over a period of 7 days even though corticosteroids had been administered. In our case, the worsening of cranial nerve VI palsy was presumed to be purely mechanical, caused by overinflation of the balloon located in the posterior part of the CS, because the worsening of the cranial nerve VI palsy started immediately after treatment.
Deflation of the overinflated balloon by a venous route via the inferior petrous sinus was not successful because the guidewire, which we used for puncture, was too soft. Conceptually, surgical approaches to deflate the balloon should be considered when entering different parts of the CS, and should be combined with interventional techniques, if necessary. Various surgical entry points into the CS have been described by different authors and were brought together into a unified geometric construct of the region in 1986 by Fukushima (11). Safe entry into the CS may be achieved via 11 triangularly shaped corridors. Batjer et al (12) described a subtemporal transdural surgical approach to the CS to treat traumatic CCF with detachable balloons. Debrun et al (13) described one case in a series of 95 traumatic CCFs in which surgical exposure and puncture of Parkinson's triangle was necessary to reach the precavernous ascending C5 segment of the ICA.
Minimal invasive surgical approaches should be preferred and combined with neurointerventional techniques, as in our case, to treat the overinflated balloon. Krisht et al (9) used a pretemporal approach via the extradural region of the superior orbital fissure to cannulate the anterior portion of the CS in a case of an aberrant balloon after endovascular treatment of a CCF. Jacobs et al (14) used a percutaneous approach through the foramen ovale to puncture a detached balloon in the CS. We used a microinvasive transnasal-transsphenoidal route to the posterior part of the CS, an alternative route to the invasive neurosurgical approach described by Mullan (anterolateral triangle) and Dolenc as well as Hakuba (medial triangle) (11).
Despite improvement in chemosis, propstosis, and pulsatile tinnitus, some patients undergoing successful endovascular balloon treatment of a direct CCF exhibit the same phenomenon post treatment, and it is not clear whether this is due to nerve irritation, increasing mass effect caused by thrombosis within the CS, or some other etiology. In view of these possible pathophysiological explanations, we assume that in our case lowering the pressure within the CS by deflation of one balloon stopped the compression of cranial nerve VI; after 8 weeks, the cranial nerve VI palsy resolved. Because computed navigation allows exact cannulation of the balloon with avoidance of irritation of the ICA or cranial nerves within the CS, the described surgical approach is easy, fast (duration of procedure, 20 min), and safe. Sonographic controls were done consecutively to exclude recanalization. Six months after treatment, the patient had no signs of fistula recurrence.
Footnotes
↵1 Address reprint requests to Joachim Klisch, Department of Neurosurgery, Section of Neuroradiology, University of Freiburg, Breisacher Str. 64, D-79106 Freiburg, Germany.
References
- Received May 8, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}