
Abstract
Summary: We report the case of a 41-year-old man with clinical findings of viral meningitis associated with acute retinal necrosis syndrome in his right eye. MR images showed right optic nerve enlargement and high-intensity signal abnormalities in the region of the left lateral geniculate body and the left occipital lobe.
Acute retinal necrosis (ARN) syndrome usually affects healthy adults. It involves the acute onset of diffuse uveitis, occlusive retinal vasculitis, vitritis, and rapidly progressive retinal necrosis (1). At end-stage, the syndrome often causes retinal detachment, optic atrophy, and severe visual loss. The origin of the syndrome is thought to be intraocular infection caused by varicella zoster virus (VZV) or herpes simplex virus (HSV) (2). We report the case of a 41-year-old man with viral meningitis associated with ARN syndrome and describe the MR findings.
Case Report
A 41-year-old man was admitted to our hospital on July 12, 1999, because of gradual, progressive loss of visual acuity and narrowing of the visual field of the right eye over the previous 3 days. Headache and periocular pain preceded the symptoms by a few days. He had no relevant family history of disease and no significant events in his personal history.
Ophthalmologic examination on admission showed visual acuity of 20/100 in the right eye and 20/20 in the left eye. The right eye showed a ciliary injection, cells and flare in the anterior chamber, and vitreous opacity. Funduscopic examination revealed characteristic scattered yellowish-white retinal exudates, retinal hemorrhage, retinal vasculitis, and edema of the optic disk. These abnormal retinal findings were more severe on the nasal side than on the aural side. The left fundus was uninvolved.
The patient was alert and well oriented, and neurologic examination revealed neck stiffness and Kernig's sign. Tendon reflexes were normal, and Babinski's sign was absent. Other cranial nerves, the cerebellum, sensation, and the extrapyramidal system were normal. Routine blood tests, urinalysis, electrocardiography, and chest X-ray all were normal. A lumbar puncture performed on July 19 revealed high intracranial pressure (230 mm H2O), 41 leukocytes/mm3 (100% mononuclear cells), a glucose level of 62 mg/dL (3.4 mmol/L), a protein level of 63 mg/dL (0.63 g/L), and negative cultures for bacteria and virus. Antibodies to HSV and VZV were not detectable in the CSF; however, polymerase chain reaction detected HSV DNA in the aqueous humor obtained on July 12.
The patient was diagnosed as having ARN syndrome and began pharmacotherapy of intravenous acyclovir (2250 mg/day), interferon-∝ (3 million IU/day), oral steroids (40 mg/day), and aspirin (80 mg/day). Retinal changes rapidly worsened. Right visual acuity deteriorated to no light perception by July 16, and then gradually improved to hand-motion perception by July 25.
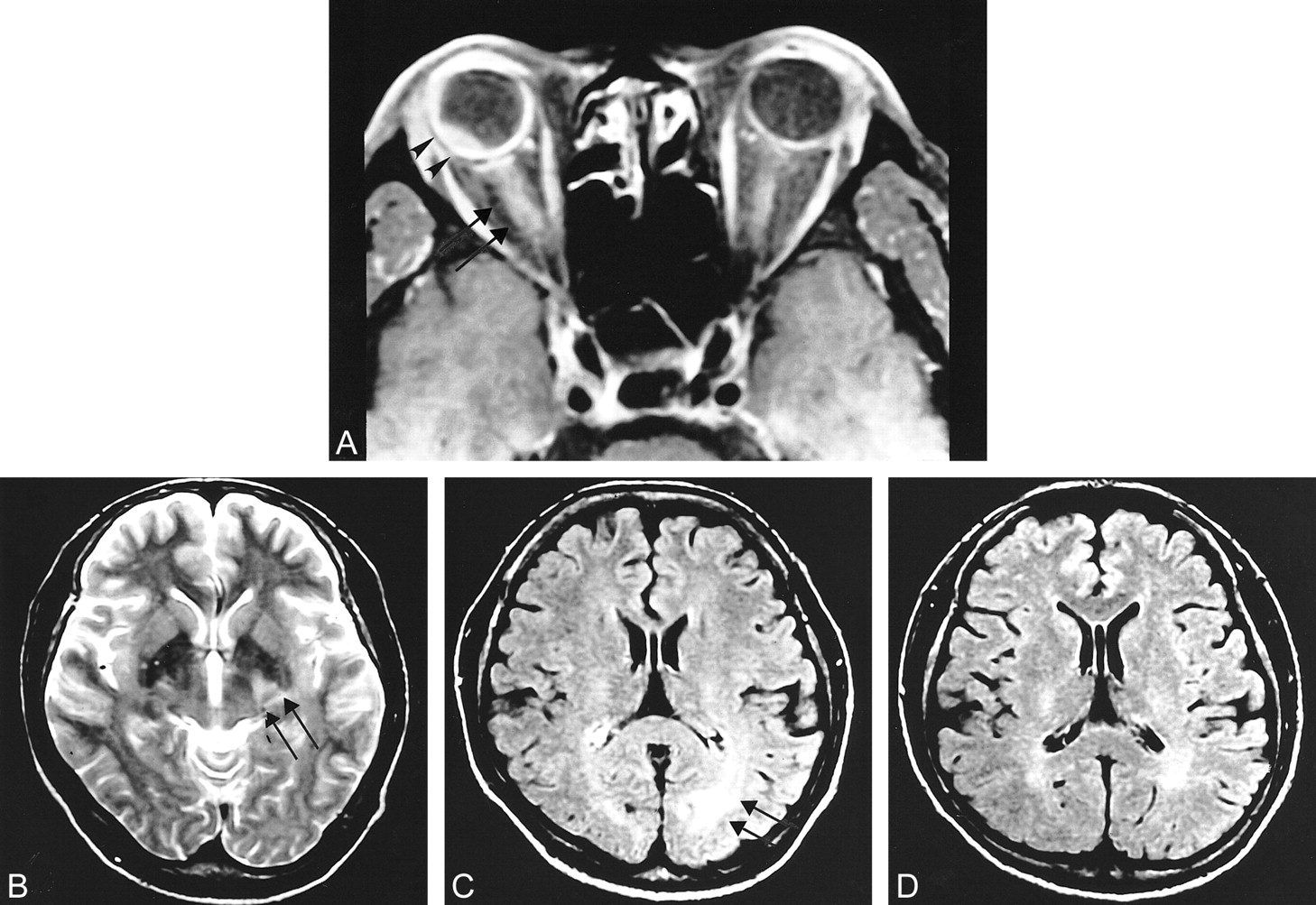
MR studies were performed on July 19 with a 1.5-T system (Magnetom Vision, Siemens-Asahi Medical Technologies, Germany). The MR images of the brain showed right optic-nerve enlargement and a crescent-shaped collection of presumed fluid along the aural side of the right orbit (Fig 1A) on fast short-inversion-time recovery images and high-intensity signal abnormalities in the region of the left lateral geniculate body (Fig 1B) and the left occipital lobe (Fig 1C) on both T2-weighted and fluid-attenuated inversion recovery (FLAIR) images. All signal abnormalities had disappeared by August 2 (Fig 1D).

MR images (A–C obtained on July 19; D, on August 2).
A, Axial fast short-inversion-time recovery image with parameters of 520/20 (TR/TE) shows right optic-nerve enlargement (arrow) and a crescent-shaped collection of presumed fluid along the aural side of the right orbit (arrowhead), although funduscopic examination revealed greater retinal abnormalities on the nasal side.
B, Axial T2-weighted image with parameters of 4000/100 shows high-intensity signal in the region of the left lateral geniculate body (arrow).
C, Axial FLAIR image with parameters of 10000/120/2300 (TR/TE/TI) shows high-intensity signal in the region of the left occipital lobe (arrow).
D, Abnormal signal changes observed in the left occipital lobe are no longer visible on FLAIR image taken August 2.
Discussion
Previous case reports have described the occurrence of ARN syndrome after HSV encephalitis (3, 4). On the basis of electron microscopic analysis of the distribution of HSV antigens in the retina, optic nerve, and brain of patients with herpetic retinitis and encephalitis, the virus is generally assumed to spread by retrograde axonal transport through the optic nerve and to invade retinal tissue directly. In contrast, viral meningitis following ARN syndrome is rare.
Three previous reports of CT or MR findings of ARN syndrome have noted optic-nerve enlargement and abnormal enhancement of the optic nerves and chiasm on postcontrast T1-weighted images, and high-intensity signal abnormalities on T2-weighted images in the region of the optic tract and lateral geniculate body (5–7). In our case, the MR images showed signal abnormalities in the region of the lateral geniculate body and occipital lobe that were greater on the left side even though the main lesion was located on the retina of the right eye. These signal changes along the visual pathway might have been construed to show neuronal degeneration, which has been termed Wallerian or transneuronal degeneration (8).
Anatomically, optic nerves and optic tracts contain the axons of the retinal ganglion cells. Visual information is relayed at the lateral geniculate body and projected onto the visual cortex in the occipital lobe through optic radiation. The optic nerves on the nasal side of the retina cross at the chiasm. The laterality of the MR findings in our case was compatible with the results of funduscopic examination, which revealed greater retinal abnormalities on the nasal side of the right eye, although MR images of the eye did show retinal detachment or subretinal fluid collection on the aural side of the right eye (Fig 1A).
Wallerian degeneration results from injury to the cell body or the proximal segment of the axon, with involution of the distal axon and its myelin sheath. Transneuronal degeneration refers to transsynaptic degeneration of the axons and myelin sheath associated with a lesion in either the afferent or efferent connection to the involved neuron. Observations of these types of degeneration in humans have so far been limited to the visual pathway, corticospinal tract, limbic system (mamillary body or fornix atrophy), dentate-rubro-olivary pathway (hypertrophic olivary degeneration), and crossed cerebellar atrophy (8). Regarding the visual pathway, MR images have revealed changes after anterograde degeneration of optic radiations from lesions involving the lateral geniculate body (9). Retrograde degeneration can cause atrophy of the optic nerves or optic tracts from postgeniculate lesions (eg, arteriovenous malformation and periventricular leukomalacia) (10, 11).
According to clinical observations in humans, MR studies cannot detect changes from Wallerian degeneration until about 4 weeks after injury to the fibers (12). From about 4 to 14 weeks after injury, the degenerated tracts appear as low-intensity signal changes on T2-weighted images, which suggests a transient increase in the lipid-protein ratio. After that, the degeneration causes high-intensity signal changes, which are attributed to glial proliferation and increased water content. The MR findings in our case showed high-intensity signal abnormalities on T2-weighted and FLAIR images obtained 7 days after onset, and these signal changes disappeared within about 3 weeks. These findings are incompatible with ordinary changes due to Wallerian degeneration. Therefore, the signal changes of the lateral geniculate body might have been caused mainly by the transient edema of the fibers along the visual pathway after the spread of inflammation or by direct viral invasion from the retina through the optic nerve. The resolution of the edema within the lateral geniculate body and occipital cortex without any evidence of dysfunction or MR findings of encephalomalacia appears impossible, however, and supports Wallerian degeneration as opposed to the edematous hypothesis.
Footnotes
1 Address reprint requests to Yukiko Tada, Department of Neurology, Yamaguchi University School of Medicine, 1-1-1 Minami-Kogushi, Ube, Yamaguchi 755-8505, Japan.
References
- Received February 23, 2000.
- Accepted after revision January 16, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}