
Abstract
Summary: The persistent hypoglossal artery is a rare perseverance of an embryonic vessel connecting the anterior and posterior circulations and is generally considered to be an incidental finding. This is a case of a patient with an atherosclerotic narrowing at the origin of the persistent hypoglossal artery seen at 3D CT angiography. The pertinent findings and clinical implications of this anomalous vessel are discussed.
The persistent hypoglossal artery (PHA) is one of four primitive connections between the anterior and posterior circulations that normally regress in utero. Of the four, the persistent trigeminal artery makes up the vast majority, with the PHA a distant second. These vessels have some clinical importance when they are associated with aneurysms or arteriovenous malformations, or when carotid endarterectomy is considered, but are generally incidental findings. There are a few reports of atherosclerotic plaque extending from the distal internal carotid artery (ICA) into the PHA, although this is the first reported case of an isolated PHA stenosis.
Case Report
A 65-year-old woman had a left carotid bruit discovered on routine physical examination when she presented with elevated blood pressure. A carotid duplex study showed calcified plaque without stenosis at the left carotid bifurcation. Elevated velocities were found in the high left ICA, corresponding to a high-grade stenosis, although no stenosis was present in the proximal and mid-portions of the ICA. CT angiography was performed after administration of 120 mL of contrast material at 3 mL/s with an 11-second delay with real-time 3D volumetric reconstructions (1-mm-thick sections) and showed a large PHA entering a slightly enlarged left hypoglossal canal and forming the basilar artery (Fig 1). There was no left vertebral artery and only a very small right vertebral artery that primarily fed the right posterior inferior cerebellar artery. No communicating arteries were present. The PHA had a 60% to 70% stenosis just beyond its origin, corresponding to the elevated velocities seen on duplex scans. Calcified plaques were present in the ICA just proximal to the takeoff of the PHA, but no significant stenosis was present.

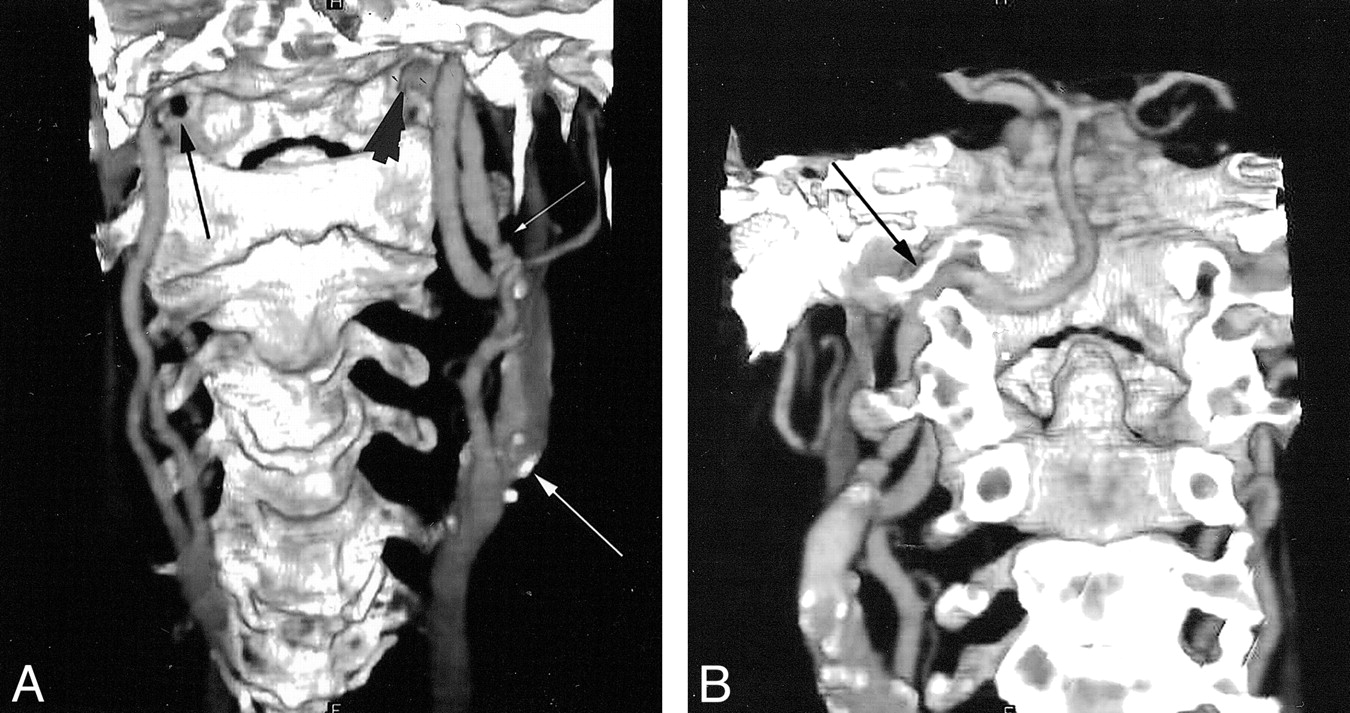
65-year-old woman with left carotid bruit and elevated blood pressure.
A, Anterior projection from a 3D CT angiogram shows an anomalous vessel arising from the distal left ICA and entering the hypoglossal canal (arrowhead), indicating that it is a PHA. The opposite normal hypoglossal canal appears dark (black arrow), as the posterior osseous structures have been removed. Note the high-grade stenosis at the origin of the PHA (small white arrow) and the atherosclerotic plaque at the carotid bifurcation without stenosis (large white arrow).
B, Posterior projection from the same data set with the removal of the posterior skull and cervical spine clearly shows the PHA coursing through the hypoglossal canal (arrow) to form the basilar artery. The proximal stenosis is again seen.
Discussion
The PHA is an uncommonly seen carotid-basilar anastomosis occurring in 0.03% to 0.26% of the population (1). The PHA typically originates from the cervical portion of the ICA at the C1–C2 level and continues medially and posteriorly to enter the skull through the hypoglossal canal. The vertebral arteries are usually absent or severely hypoplastic, and there are no posterior communicating arteries. Arteriovenous malformations and intracranial aneurysms have been associated with a PHA, and there are cases of aneurysms forming from the PHA itself (1–3). While generally an incidental finding, identification of a PHA is important before carotid endarterectomy or skull base surgery. Diagnostic angiograms are also obtained before performing a Wada test to exclude a carotid-vertebral anastomosis.
Because the origin of the PHA from the ICA forms similar flow dynamics as are seen at the carotid bifurcation, it is not surprising that there have been reported cases of atherosclerotic stenosis of the ICA near the PHA takeoff, occasionally with extension into the PHA (4–6). This has been reported as a cause of a false-positive carotid duplex scan; in this case, the duplex scan was initially read as a distal ICA stenosis (7).
Conventional angiography, MR angiography, MR imaging, and CT angiography have all been used in the diagnosis of PHA (1–3, 8, 9). Although conventional angiography has been considered the standard of reference when evaluating vascular structures, CT angiography is a noninvasive alternative that has some advantages. CT angiography affords excellent anatomic localization because of its ability to show the vessel entering the enlarged hypoglossal canal, particularly when using 3D reconstruction techniques.
In this case, there was an isolated high-grade stenosis of the PHA without an associated ICA stenosis, although calcified plaque was evident in the ICA just proximal to the PHA origin. As the patient is currently asymptomatic, she will be treated medically. However, it is likely that she will experience such symptoms as syncope or vertigo in the future if the stenosis progresses. The clinical sequela of reduced blood flow in a PHA can be profound, as there is usually no other blood supply to the brain stem or posterior fossa, making intervention hazardous in such cases. Endarterectomy has been successfully performed in patients with combined ICA-PHA stenosis but has never been described in an isolated PHA stenosis. The surgery is technically difficult owing to the location of the ICA-PHA bifurcation and often requires mandibular subluxation and cranial nerve dissection (5). Even when not stenotic, identification of a PHA before ICA endarterectomy is important, as intraoperative arteriography may be necessary to confirm that the PHA is the shunted vessel (4). Because this patient had an isolated stenosis of the PHA, endovascular treatment, such as percutaneous transluminal angioplasty or stent placement, might be alternatives.
PHAs are uncommon vascular anomalies that can be clinically important because of atherosclerotic disease forming at the takeoff from the ICA. The diagnosis can easily be made with CT angiography, which is also useful as an anatomic reference because of its 3D capabilities.
- Received September 29, 2000.
- Accepted after revision March 20, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.