
Abstract
Summary: We present an unusual case of a primary lumbar disk-space mass that presumably developed secondary to a chronic hyperextension spinal fracture associated with spinal stenosis. This injury resulted in the appearance of a lumbar intervertebral disk-space mass or pseudotumor. The pseudotumor most likely resulted from a prior spinal fracture, leading to a fused hyperextension deformity in a patient with underlying chronic degenerative spinal disease.
The lumbar-spine intervertebral disk space is rarely involved with primary tumor (1). When seen, involvement is usually a result of contiguous neoplastic invasion, either from vertebral body neoplasia with direct invasion of the disk space or from paraspinal tumor with resultant disk-space involvement. Infectious diseases, such as tuberculosis or those caused by Staphylococcus aureus, frequently involve lumbar intervertebral spaces, but they do not typically result in intervertebral disk-space expansion. We present an unusual case in which a primary lumbar disk-space mass arose secondary to a chronic hyperextension spinal fracture associated with spinal stenosis. This injury resulted in the appearance of a lumbar intervertebral disk-space mass or pseudotumor.
Case Report
An 84-year-old woman with chronic cardiac problems presented with a history of low back pain of several years’ duration. In the 2 months before her hospital admission, she had increasing low back pain to the extent that she could no longer walk. She had minimal pain in the lower extremities. Her bladder and bowel function were maintained, and the patient had no history of weight loss. On examination, power in the lower extremities was 4 on a scale of 5. Knee and ankle reflexes were absent; plantar reflexes were flexor. The patient’s sensation was intact. She required intravenous narcotic medication by means of a patient-controlled anesthesia pump.
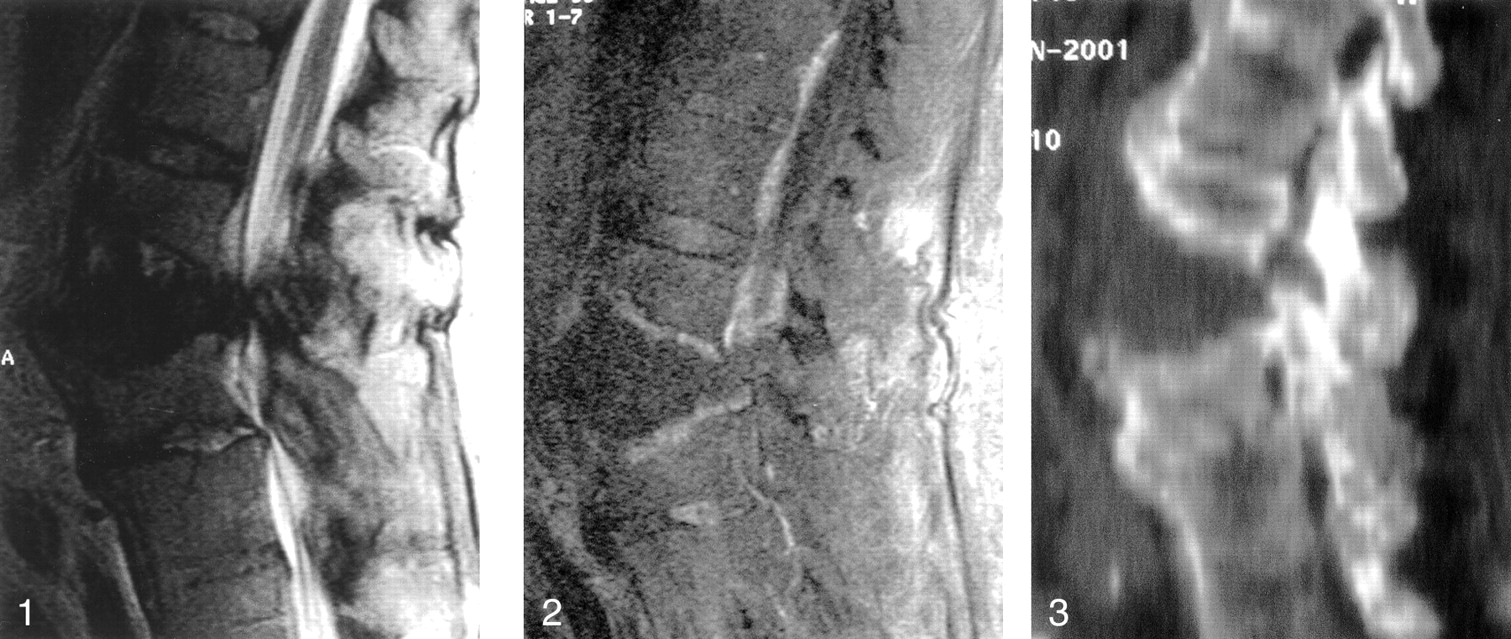
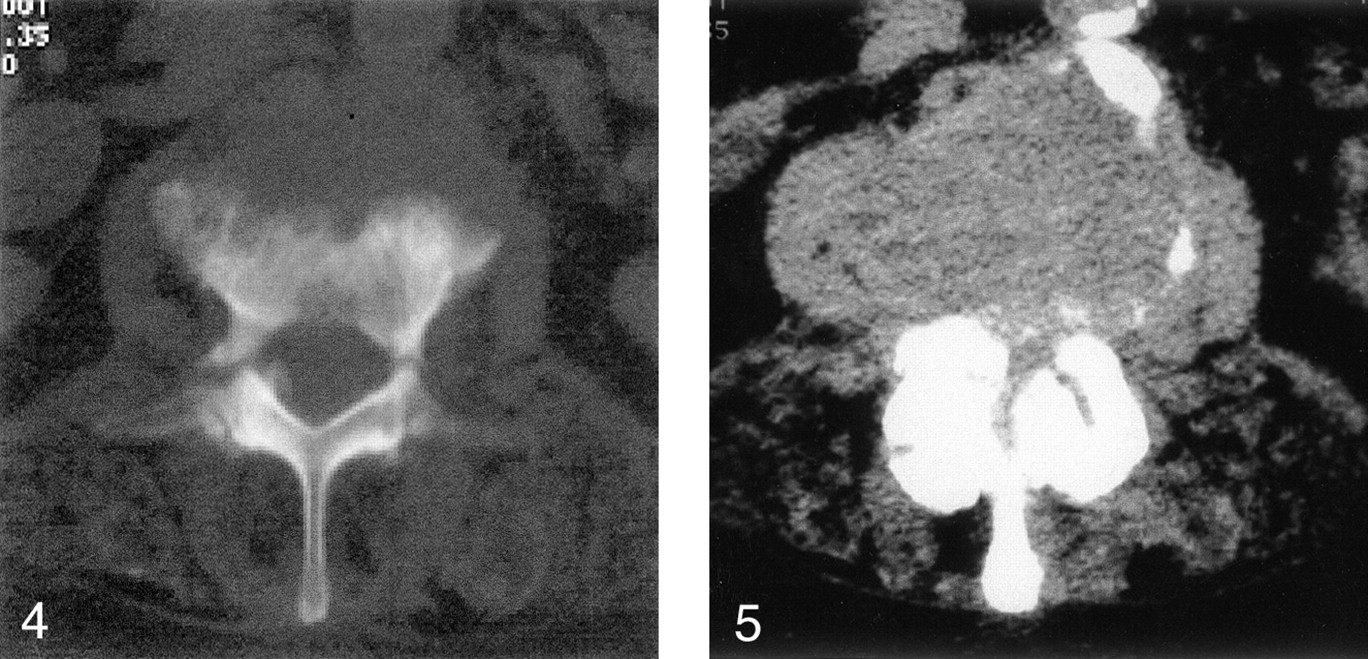
MR imaging demonstrated an expansile mass at the L2-L3 level (Fig 1). The mass demonstrated low signal intensity on T1-weighted images, and remained low in signal intensity on T2-weighted images (Fig 2). Interestingly, the signal intensity in the intervertebral disk was preserved along the lower L2 endplate on T2-weighted images, yet it remained indistinguishable on T1-weighted images. The mass did not enhance with the injection of contrast material, although the vertebral body endplates did. The CSF signal intensity in the central canal was obliterated because of associated central canal stenosis. CT showed that the mass was soft-tissue material that was isoattenuated relative to skeletal muscle (Fig 3). The study further showed bilateral L2 pedicle fractures, with deformed L2 and L3 vertebral-body endplates associated with sclerosis. Central canal stenosis due to a combination of the disk-space mass and posterior-element changes was present. Air attenuation or vacuum phenomenon was not seen within the disk space (Fig 4). Both the L2-L3 and L3-L4 disk levels showed severe degenerative spinal stenosis, as demonstrated on both MR images and CT scans (Fig 5). Further, extensive laminar calcification was present along the margins of the vertebral body; this finding was suggestive of longstanding arthropathy, that is, diffuse idiopathic skeletal hypertrophy.

MR sagittal T2-weighted image shows an expansile mass at the L2-L3 disk level that represents the pseudotumor. The disk attached to the inferior L2 endplate has increased signal intensity. Spinal stenosis is present at the L2-L3 and L3-L4 levels.

Gadolinium-enhanced T1-weighted sagittal MR image shows endplate enhancement at the L2-L3 level.

Sagittal CT reconstruction of the lumbar spine shows a disk-space mass with an extension deformity. Note the laminar calcification along the anterior vertebral margins disrupted by the disk-space mass and the facet malalignment.

Axial CT scan (bone window) at the L2 level shows bilateral pedicle fractures. Note the moth-eaten appearance of the L2 endplate simulating an underlying destructive mass.

Axial soft tissue–window CT scan (soft tissue window) at the level of the L2-L3 disk space demonstrates severe central-canal stenosis. This finding was also apparent at the L3-L4 level (not shown).
Clinically, in view of the expansile lesion at the L2-L3 level, a neoplasm was suspected. Results of a metastatic workup were negative. The patient’s pain was thought to be largely related to the severe lumbar central-canal and foraminal stenosis. A decompressive laminectomy was performed from L2 to L5, with the finding of severe central canal stenosis, particularly at L2 and L3. The L2-L3 disk space consisted of a large, empty cavity. No tumor was seen, but some fragments of blood clot and whitish-yellow fragments of tissue were noted. At pathologic analysis, these tissue fragments were reported as fibrous exudate with reactive granulation (Figs 6 and 7). Cultures of the tissue in the depths of the L2-L3 disk proved to be sterile. The patient tolerated the procedure well, with considerable relief of her pain at rest, but she continued to have moderate pain during trunk movement. She died 2 months later in a rehabilitation facility. Autopsy was not performed.

Low-power photomicrograph shows reparative granulation tissue (solid arrows) and a proliferation of capillaries. Bone (open arrow on the left) and cartilage (open arrows on the right) are adjacent to the granulation tissue.

Medium-power photomicrograph shows extensive fibrin stroma (pink) with scattered fibroblasts (elongated cells) and inflammatory cells (lymphocytes and polymorphonuclear cells).
Discussion
Vertebral pseudotumors may be classified into those of vertebral origin and those of disk-space origin. Those of vertebral origin, as cited in the literature, include those related to spinal tuberculosis; cystic masses such as a hydatid cyst; synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome; eosinophilic granuloma; Langerhans cell histiocytosis; fibrous dysplasia; and osteoporotic vertebral collapse (2). Tuberculous pseudotumors can present as destructive vertebral masses that may not radiographically appear to be of infectious origin. Cystic bone lesions, such as hydatid cysts, can occupy a significant bulk of any given vertebral element to mimic a more aggressive lesion (3).
The SAPHO syndrome may mimic vertebral tumors (eg, sclerotic bone tumors) because of the erosive changes with adjacent sclerosis and the hyperostosis that can appear similar to blastic vertebral metastasis (2). In cases of SAPHO, additional lesions can be identified with conventional radiography, bone scintigraphy, CT, or MR imaging. Again, the findings may be suggestive of metastatic disease when this disease process is actually benign. Eosinophilic granuloma, which is a localized form of Langerhans cell histiocytosis, may appear as a pseudotumoral vertebral lesion and is most commonly found in children younger than 10 years (2). These lesions frequently appear with vertebral collapse or vertebra plana (4). Such cases can also be seen in young adults, predominantly in male patients (2, 5). Space-occupying masses are seen in fibrous dysplasia. In such cases, T1-weighted MR images may show decreased signal intensity, and T2-weighted images may show variable signal intensity, depending on the degree of lesion ossification. Chordoma, a mass that arises from a remnant of the notochord, can also appear as a disk-space mass. These tumors occur chiefly in the occipital-cervical and sacrococcygeal regions, and they less frequently appear in the lumbar, cervical, and thoracic regions (7).
The detection of gas within a vertebral disk, especially in the lumbar region, is often consistent with the vacuum phenomenon (8–11). This finding represents an accumulation of gas between the vertebral bodies that is typically more than 90% nitrogen (12). In the presence of a vacuum phenomenon, one can almost exclude the possibility of neoplastic growth because the presence of gas in the disk space may represent a gas-producing infection (13, 14). Importantly, the presence of gas is only rarely associated with infectious spondylitis, but it has been reported in cases of infection with Clostridium species, Brucella organisms, Mycobacteria tuberculosis, Peptococcus species, Streptococcus viridans, Escherichia coli, and Staphylococcus epidermidis (13).
This case involved an expansile soft-tissue mass within the disk space that suggested the possibility of a tumor. Our general experience has been that the height of the intervertebral disk space concomitantly and minimally increases in proportion to the adjacent vertebral compression fractures. However, in this case, the extension fracture deformity widely expanded the space, tearing the inferior attachment of the intervertebral disk. We postulate that the widened space then became occupied with chronic fibrotic tissue, resulting in soft-tissue attenuation at CT. The MR signal intensity mimicked changes seen in processes such as epidermoid or chronic mucocele (that displaying isointensity on T1-weighted images and hypointensity on T2-weighted images).
Conclusion
We believe that this pseudotumor arose secondary to an extension spinal fracture deformity in a patient with degenerative spinal rigidity with spinal stenosis. Interestingly, an air or vacuum phenomenon was not present within the pathologic disk space on any imaging study despite the presence of degenerative disk disease.
Acknowledgments
The authors gratefully acknowledge the histopathologic contribution by Dr Lorenzo Galindo, Department of Pathology, Drexel University College of Medicine.
References
- Received February 20, 2002.
- Accepted after revision July 9, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.