
Abstract
Summary: Intracranial true mycotic aneurysms are rare and generally lethal. We report a case of a near-drowned child with brain abscesses due to Pseudallescheria boydii, a saprophytic fungus, who died after subarachnoid hemorrhage occurred. CT showed contrast-enhancing lesions indicative of aneurysms of basilar and right posterior cerebral arteries that could not be appreciated 2 days before. P. boydii is often resistant to commonly used antimycotic drugs. Because CNS infection is frequently associated with near-drowning, early diagnosis and specific therapy are strongly recommended for these patients.
Pseudallescheria boydii (previously named Petriellidium boydii) and its asexual form, Scedosporium apiospermum, are ubiquitous saprophytic fungi that cause chronic subcutaneous infection (ie, true fungal mycetoma, “maduromycosis”) and, less frequently, other localized or even disseminated infections that tend to have a chronic-progressive course despite treatment (1, 2). CNS invasion that may manifest as brain abscess (approximately 77% of the cases), meningitis, encephalitis, ventriculitis, or vascular involvement resulting in sinus thrombosis and cerebral infarction has been reported as occurring in approximately 40 patients (1–11); because of frequent resistance to antimycotic drugs, the prognosis is poor. Approximately 76% of the cases result in death (8). Intracranial aneurysms caused by this challenging CNS pathogen have been rarely reported (12, 13). True mycotic aneurysms are also rare in general, and they are associated with a very high mortality rate (13, 14). We report a case of a near-drowned child with P. boydii brain abscesses who died after subarachnoid hemorrhage was caused by aneurysms of the basilar and posterior cerebral arteries. CT scans provided the diagnosis and showed their extremely rapid growth.
Case Report
A previously healthy 3-year-old girl was admitted to our pediatric intensive care unit in a coma, with hypoxemia, metabolic acidosis, and unstable vital signs, after near-drowning in polluted water. After a few days, she became feverish. Laboratory tests showed infection, but cultures failed to grow any organisms; the chest radiograph showed pulmonary edema, but no focal lesions. Broad-spectrum antibiotic therapy was administered. Approximately 4 weeks later, a neurologic examination revealed right hemiparesis and CT showed right frontal and left frontotemporal lesions, consistent with abscesses. The left frontotemporal lesions were associated with more conspicuous edema and exerted marked mass effect on the ventricular system and midline structures (Fig. 1). The left-sided lesion was surgically drained and excised, and resolution of the mass effect was achieved. A culture of the whitish dense material obtained at drainage yielded S. apiospermum, and IV administered itraconazole was started. Despite this, CT performed during the ensuing days showed progression of the infection, with new micronodular abscesses. On postoperative day 8, the patient experienced sudden neurologic deterioration. CT showed extensive subarachnoid and intraventricular hemorrhage, with associated hydrocephalus. Inside the interpeduncular cistern, near the subarachnoid hemorrhage, CT revealed new, irregularly roundish lesions surrounded by the hyperattenuated blood. Contrast-enhanced CT confirmed these lesions to be highly consistent with aneurysms of the basilar and right posterior cerebral arteries (Fig 2A and B). The child’s condition rapidly deteriorated to the point of clinical brain death. The family denied autopsy. CT scans obtained 2 days before the fatal hemorrhage were retrospectively reviewed. They showed only a dilated perimesencephalic portion of the right posterior cerebral artery, providing evidence of the rapid extension of vascular compromise and tumultuous aneurysm evolution.

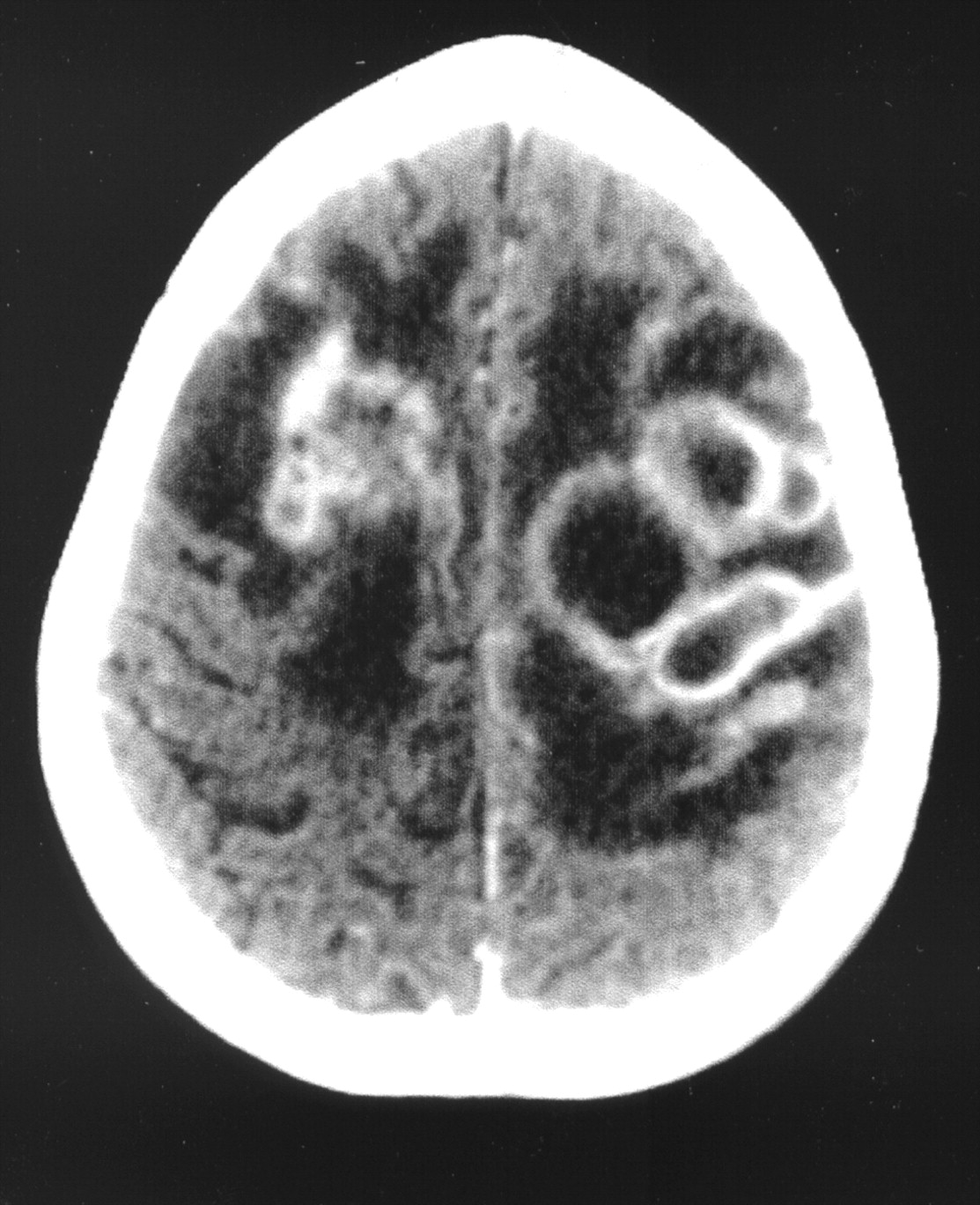
CT scan of the brain obtained on day 29, after the IV administration of contrast medium, shows multiple enhancing ring-shaped lesions, consistent with abscesses in both hemispheres, with marked peripheral hypoattenuation, consistent with edema.

CT scans of the brain obtained on postoperative day 8.
A, CT scan shows subarachnoid and intraventricular hemorrhage, associated with hydrocephalus. New, irregularly roundish lesions surrounded by the hyperattenuated blood can be seen inside the interpeduncular cistern.
B, Contrast-enhanced CT scans show intense enhancement of these lesions, confirming the hypothesis of aneurysms of the basilar and right posterior cerebral arteries.
Discussion
Fungal (ie, true mycotic) aneurysms of the intracranial circulation are rare and differ from the more common bacterial “mycotic” aneurysms. These tend to be distal and small and to have an acceptable prognosis with medical and surgical treatment (13), whereas fungal aneurysms usually affect the circle of Willis and proximal arterial tree, tend to enlarge and extend involving long segments of the vascular wall, and are friable and poorly defined as shown by pathologic studies. Therefore, their endovascular or surgical treatment is extremely difficult if not impossible and they are associated with a very high (nearly 100%) mortality rate (12–14). Recent pathologic studies have thrown light on the pathogenetic mechanism of aneurysm formation in cases of CNS aspergillosis, the mycosis that most commonly causes intracranial aneurysms, documenting a massive destruction of the elastic lamina of the arterial wall (14). Although it has been pointed out that P. boydii, like Aspergillus species, shows a high affinity for blood vessels (2, 5), and although hemorrhagic features were found in some cases of CNS pseudallescheriasis (5, 10, 11), cerebral aneurysms caused by this organism are much rarer. In our review of the literature, we were able to find only two descriptions of these lesions (12, 13); the involved vessels were the right internal carotid (segments C1 to C4) and the basilar arteries, respectively. Both cases were unsuccessfully treated. The former patient (an immunocompromised near-drowned woman with associated thrombotic occlusion of the right sylvian artery and brain abscesses) died 71 days after the event, after experiencing progressive severe deterioration due to her overall brain disease (12). The latter (an immunocompetent woman who had undergone surgical drainage of sinusitis 5 and 4 months before admission and presented with subarachnoid hemorrhage) died after approximately 12 days, during which her fusiform aneurysm enlarged rapidly despite aggressive treatment (13). In both cases, the diagnosis was made with intracranial arteriography, and neither case underwent pathologic study. Our report lacks pathologic and arteriographic evidence, because autopsy was refused. Cerebral arteriography was not performed because of the rapidly progressive neurologic deterioration and death of the girl. Nevertheless, the findings shown by the last CT scans were highly suggestive for a diagnosis of mycotic aneurysms, and retrospective evaluation of those obtained 2 days earlier showed rapid progression to rupture, providing a striking imaging confirmation of the characteristic aggressivity of fungal vascular lesions, as shown by pathologic study (14).
Fungal aneurysms do represent a treatment challenge, and in cases of fungal CNS infection, aggressive treatment should be started as early as possible. It should be emphasized that distinguishing P. boydii from Aspergillus species, morphologically related but differentiated by culture and antigen studies, may be extremely important from a therapeutic point of view because of its particular susceptibility characteristics (see below). P. boydii CNS invasion may follow extension from a source near the brain (eg, paranasal sinuses, eye, ear), direct inoculation (eg, with trauma or surgery), or hematogenous spread from the lung in cases of massive aspiration, that typically takes place with near-drowning in polluted water (8). There is increasing evidence that aspiration of polluted water is an important factor predisposing to CNS pseudallescheriasis, even in immunologically intact patients. In 1996, Wilichowski et al (6) reviewed eight uniformly fatal cases of near-drowned patients with brain abscesses caused by this organism, none of whom was immunocompromised. Invasive pneumonitis and then hematogenous spread is likely to be the main means of P. boydii CNS entry, with some role possibly played by intensive care corticosteroid therapy in enhancing its pathogenicity. Early diagnosis of the infection may be difficult (2, 6), and the onset of neurologic symptoms revealing P. boydii CNS invasion may be late (several weeks, and even months) (6, 9). Therefore, a high index of suspicion should be maintained in near-drowned patients to ensure early diagnosis of mycotic infection and detection of CNS dissemination. However, more effective treatment of P. boydii CNS infection is still needed. Surgery and complementary specific medical therapy have been proved to provide the best chances; however, successful management of such cases has been rarely accomplished (8). This partly depends on the frequent resistance of this organism to antimycotic drugs and scarce availability of potentially effective antimycotic drugs in brain compartment. P. boydii has often proved resistant to a variety of commonly used antimycotic agents, primarily amphotericin B (2, 5, 6, 8, 10, 11, 13), whereas drugs in the azole family have been more successfully used (8). It has been suggested that Voriconazole might be the agent with the best combination of anti-pseudallescherial activity and CNS penetration (8, 9).
References
- Received January 8, 2002.
- Accepted after revision June 6, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}