
Article Figures & Data
Figures
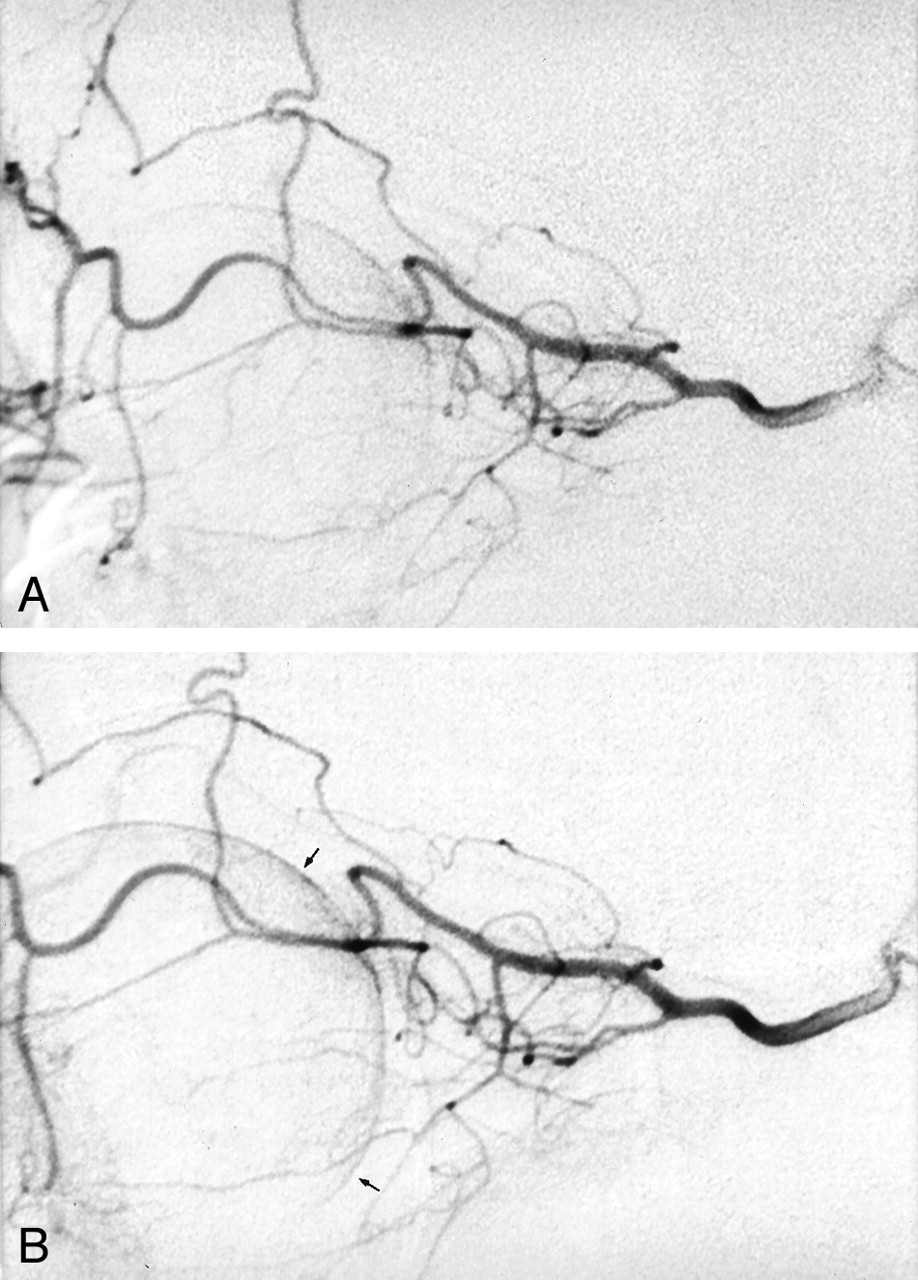
- Fig 1.
Superselective angiography of the ophthalmic artery in a patient with acute blindness due to CRAO.
A, Before the administration of LIF.
B, After the administration of LIF, no significant changes were noted, except for slightly better choroidal-retinal perfusion (arrows).

Tables
Authors No. of Patients Medical Treatment Final Results Karjalainen, 1971 (19) (Patients with arteritis were included) 91 No comment 58%blind, 21%good or reduced visual acuity Neubauer et al., 2000 (20) 65 Acetazolamide, acetylsalicylic acid, massage of the globe, Pentoxifyllin, beta-blocker, paracentesis 15%showed distinct improvement (at least three visual acuity gradations) Schmidt et al., 1992 (18) (Control group of conservative treatment in comparison with small number of patients with LIF treatment) 41 Ocular massage, Pentoxifyllin, and anterior chamber paracentesis Virtually no visual improvement; visual acuity improved to 20/50 in only one patient Atebara et al., 1995 (8) 40 Paracentesis and Carbogen treatment Nine (22.5%) patients, visual improvement Augsburger and Magargal, 1980 (21) 34 Paracentesis, ocular massage, inhalational therapy (95%oxygen and 5%carbon dioxide), acetazolamide, and aspirin Helpful in 12 (35%) patients (visual acuity ≥20/100) Duker et al., 1991 (9) 33 Carbogen (95%oxygen and 5%carbon dioxide), ocular massage, anterior chamber paracentesis, topical timolol maleate, acetazolamide 29 patients, low vision (ie, counting fingers or hand movements); one patient, vision deteriorated from 20/40 to hand motions; two patients, final visual acuity of 20/40; one patient, 20/50; one patient, 20/20 Wolf et al., 1989 (10) 20 Hypervolemic or isovolemic hemodilution 10 patients, central vision improved Magargal and Goldberg, 1977 (22) 20 Paracentesis Five patients, significant improvement; five patients, moderate improvement Lorentzen 1969 (23) 12 No comment In no case was there any improvement, rather deterioration (10-year follow-up) Rumelt et al., 1999 (14) 11 Ocular massage, sublingual isosorbide dinitrate, acetazolamide, mannitol or glycerol, paracentesis, methylprednisolone, streptokinase, and retrobulbar tolazoline Eight patients, improvement Gombos, 1970 (24) 7 Dextran (Rheomacrodex) with papaverine hydrochloride Two patients, complete recovery; three patients, marked improvement Perkins et al., 1987 (13) 5 Acetazolamide, inhalation of 5%carbon dioxide and 95%oxygen, aspirin Three patients, spontaneous improvement to 20/50 or better; two patients, 20/80 or better after treatment Beiran et al., 1993 (11) 4 Hyperbaric oxygenation combined with ocular massage, nifedipine, and glycerol Three patients, treatment began <100 min, considerable improvement in vision; one patient, treatment began at 6 hr, no improvement - TABLE 2:
Conservative treatment of 29 patients with incomplete central retinal artery occlusion
Pentoxifyllin Hemodilution Aspirin Acetacolamid (Diamox) Heparin 2* (7.89%) 25† (86.2%) 4 (13.79%) 3 (10.34%) 10 (34.48%) Additional treatment or single treatment Pentoxifyllin + additional treatment in one patient* Hemodilution + additional treatment in 12 patients† 9 Heparin + 1 Marcumar) Pentoxifyllin only in one (3.45%) patient Hemodilution only in 11 (39.93%) patients Aspirin only in one (3.45%) patient Diamox only in one (3.45%) patient Heparin only in one (3.45%) patient Note.—In all patients, an immediate massage of the globe and treatment of high blood pressure were performed.
* Pentoxifyllin + hemodilution + aspirin, one (3.45%) patient.
† Hemodilution + heparin, nine (31.03%) patients; hemodilution + aspirin, two (6.89%) patients; hemodilution + Diamox, two (6.89%) patients.
- TABLE 3:
Conservative treatment of 83 patients with subtotal central retinal artery occlusion
Pentoxifyllin Infusions Hemodilution Aspirin Acetacolamide (Diamox) Rheomacrodex Infusions Heparin Eye Drops for Lowering Eye Pressure Paracentesis 29 (34.9%) 46 (54.21%) 28 + 1 Plavix + 1 Tiklyd: 30 (36.14%) 9 (10.84%) 8 (9.64%) 16 (19.28%) 11 (13.25%) 13 (15.66%) Additional treatment or single treatment Pentoxifyllin + additional treatment*: 21 patients (25.3%) Pentoxifyllin + additional treatment†: 36 (43.37%) Aspirin + additional treatment‡: 25 (30.12%) Acetacolamide + additional treatment§: nine (10.84%) Rheomacrodex + additional treatment§§: eight (9.64%) Heparin + additional treatment: 14 (16.87%) Eye drops + additional treatment: 11 (13.25%) Paracentesis + additional treatment: 11 (13.25%) Pentoxifyllin only: eight patients (9.64%) Hemodilution only: 10 (12.05%) Aspirin only: five (6.02%) Acetacolamide only Rheomacrodex only Heparin only: two (2.41%) Eye drops only Paracentesis only: two (2.41%) Note.—In all patients, immediate massage of the globe and treatment of high blood pressure were performed.
* Pentoxifyllin + aspirin, five (6.02%) patients; Pentoxifyllin + Diamox, one (1.2%) patient; Pentoxifyllin + aspirin + Diamox, one patient; Pentoxifyllin + Rheomacrodex, two (2.41%) patients; Pentoxifyllin + hemodilution, one patient; Pentoxifyllin + Paracentesis, three (3.61%) patients; Pentoxifyllin + hemodilution + aspirin + paracentesis, one patient; Pentoxifyllin + eye drops + paracentesis, two (2.41%) patients; Pentoxifyllin + hemodilution + eye drops + paracentesis, one patient; Pentoxifyllin + hemodilution + aspirin + heparin: one patient; Pentoxifyllin + Diamox + Rheomacrodex + paracentesis, one patient; Pentoxifyllin + hemodilution + eye drops, one patient; Pentoxifyllin + Diamox + paracentesis, one patient.
† Hemodilution + aspirin, 12 (14.45%) patients; hemodilution + eye drops, three (3.61%) patients; hemodilution + heparin, 10 (12.05%) patients; hemodilution + aspirin + heparin, one (1.2%) patient; hemodilution + aspirin + eye drops, one patient; hemodilution + Diamox + Rheomacrodex + paracentesis, one patient; hemodilution + aspirin + Diamox + heparin, one patient; hemodilution + eye drops + Diamox, one (1.2%) patient.
‡ Aspirin + Heparin, one patient; aspirin + Rheomacrodex, one patient.
§ Diamox + Rheomacrodex + eye drops, two patients.
§§ Rheomacrodex + paracentesis, one patient.
- TABLE 3a:
Conservative treatment of four patients with a total central retinal artery occlusion
Pentoxifyllin Infusions Hemodilution Aspirin Acetacolamide (Diamox) Rheomacrodex Infusions Heparin Eye Drops for Lowering Eye Pressure Paracentesis One patient* Two patients One patient One patient Note.—In all patients, immediate massage of the globe and treatment of high blood pressure were performed.
* One patient was treated with Pentoxifyllin infusions + Diamox + paracentesis.
0 Blindness, no light perception I (high degree of visual loss) Perception of light, finger counting, recognition of hand motions II (pronounced degree of visual loss) 1/50–1/15 III (distinct degree of visual loss) 0.1–0.3 IV (minor degree of visual loss) 0.4–1.0 Stage of Occlusion No. of Patients Subtotal 130 (73.0%) Incomplete 39 (21.9%) Total 9 (5.1%) - TABLE 6:
Influence of treatment on 178 patients with central retinal artery occlusion: results of ordinal logistic regression for visual acuity after treatment
Effect No. of Patients Wald’s χ2 P Treatment Conservative 116 (65.17%) LIF 62 (34.3%) 9.38 b 0.0022 Gender Male 125 (70.2%) b Female 54 (30.3%) 0.17 0.6834 e Occlusion Subtotal 130 (73.0%) b Incomplete 39 (21.9%) 26.49 0.0001 Complete 9 (5.1%) 4.53 0.0332 Age 18–89 years 8.71 0.0032 Latency 1–312 hr 3.97 0.0459 Initial visual acuity 0–5 43.31 0.0001 Note.—LIF indicates local intra-arterial fibrinolysis; b, baseline (reference) class; e, removed by backward elimination; (given P values are probability to remove values).
- TABLE 7:
Results for ordinal logistic regression for change of visual acuity under treatment: subpopulation of subtotal occlusions
Effect Classes/Range Wald’s χ2 P Treatment Conservative, 5.70 b 83 (63.8%) b 0.0169 LIF, 47 (36.15%) (36.15%) Gender Male 93 0.01 b (71.5%) 0.9061 e Female, 37 (28.5%) (28.5%) Age 18–89 years 8.85 0.0029 Latency 1–312 hr 3.60 e 0.0579 e Initial visual acuity 1–3 4.28 0.0385 Note.—LIF indicates local intra-arterial fibrinolysis; b, baseline (reference) class; e, removed by backward elimination.
- TABLE 8:
Visual improvement after intra-arterial fibrinolysis: three different stages in 62 patients
Stage of CRAO Group with Distinct Visual Improvement n = 10 patients (16.13%) Group with Partial Visual Improvement n = 26 patients (41.93%) Group without Visual Improvement n = 26 patients (41.93%) Stage I (incomplete) 5 (50%) 3 (30%) 2 (20%) Stage II (subtotal) 5 (10.64%) 19 (40.43%) 23 (48.94%) Stage III (total) (no light perception) 0 4 (80%) 1 (20%) Treatment of 62 patients with intra-arterial fibrinolysis: time interval of treatment after blindness Treatment <6 hr after Visual Loss (n = 10) Treatment ≥6–14 hr after Visual Loss (n = 26) Treatment >14 hr after Visual Loss (n = 26) Distinct improvement 4 (30.77%) 5 (13.16%) 1 (9.09%) Partial improvement 6 (46.15%) 15 (39.47%) 5 (45.45%) No improvement 3 (23.08%) 18 (47.37%) 5 (45.45%) Note.—CRAO indicates central retinal artery occlusion.
- TABLE 9:
Visual improvement after conservative treatment: three different stages in 116 patients
Stage of CRAO Group with Distinct Visual Improvement n = 7 patients (6.5%) Group with Partial Visual Improvement n = 27 patients (23.28%) Group without Visual Improvement or with Deterioration n = 82 patients (70.69%) Stage I (incomplete) 5 (17.24%) 14 (48.28%) 10 (34.48%) Stage II (subtotal) 2 (2.41%) 13 (15.66%) 68 (81.93%) Stage III (total) (no light perception) 0 0 4 (100%) Conservative treatment of 116 patients: time interval of treatment after blindness Treatment <6 hr after Visual Loss n = 31 (26.72%) Treatment: ≥6 to 14 hr after Visual Loss n = 44 (37.93%) Treatment: ≥14 hr after Visual Loss n = 41 (35.34%) Distinct improvement 1 (3.23%) 3 (6.82%) 3 (7.32%) Partial improvement 7 (22.58%) 11 (25.00%) 9 (21.95%) No improvement 23 (74.19%) 30 (68.18%) 29 (70.73%) Note.—CRAO indicates central retinal artery occlusion.
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Intravenous lipo-prostaglandin E1 administration for patients with acute central retinal artery occlusion
- Efficacy and Safety of Intra-Arterial Thrombolysis in Central Retinal Artery Occlusion
- Systemic Prostaglandin E1 to Treat Acute Central Retinal Artery Occlusion
- Efficacy of Intravenous Tissue-Type Plasminogen Activator in Central Retinal Artery Occlusion: Report From a Randomized, Controlled Trial
- Local Intraarterial Fibrinolysis Administered in Aliquots for the Treatment of Central Retinal Artery Occlusion: The Johns Hopkins Hospital Experience
- Intra-arterial thrombolysis for central retinal artery occlusion
- Intra-arterial thrombolysis for central retinal artery occlusion: a systematic review
- Activation of the Mitochondrial Apoptotic Pathway in a Rat Model of Central Retinal Artery Occlusion
- Thrombolysis for central retinal artery occlusion
- Comparison of intra-arterial thrombolysis with conventional treatment in patients with acute central retinal artery occlusion