
Abstract
Summary: Venous sinus thrombosis is a relatively uncommon disorder that frequently is associated with confusing clinical findings and delayed diagnosis. Patients are often screened with unenhanced CT, and CT findings may be subtle and may include hyperattenuation of cerebral veins or venous sinuses secondary to intracranial thrombosis. This hyperattenuation may be mimicked by polycythemia, as shown in this case.
Increased radiographic attenuation of cerebral veins and sinuses is one of the earliest signs of venous sinus thrombosis. We present a case of polycythemia (hematocrit, 69.8) that mimicked this CT sign of venous thrombosis. MR imaging of the brain and MR venography clarified the diagnosis and are necessary to definitively make or exclude the diagnosis of cerebral venous thrombosis. We could not find a direct reference in a search of the radiology literature describing these CT findings in association with polycythemia (1–4)
Case Report
A 27-year-old severely retarded nonverbal Hispanic female with Down syndrome presented with her first generalized tonic-clonic seizure. CT findings were misinterpreted as showing a cerebellar hemorrhage (Fig 1). The patient was transferred to a medical center far from home and without accompanying family members. Limited but significant medical history that was sent with the patient included repaired trilogy of Fallot, chronic cyanosis, pulmonary hypertension, and a history of “stroke” at age 1 year. A neurologic examination documented lethargy but was nonfocal.

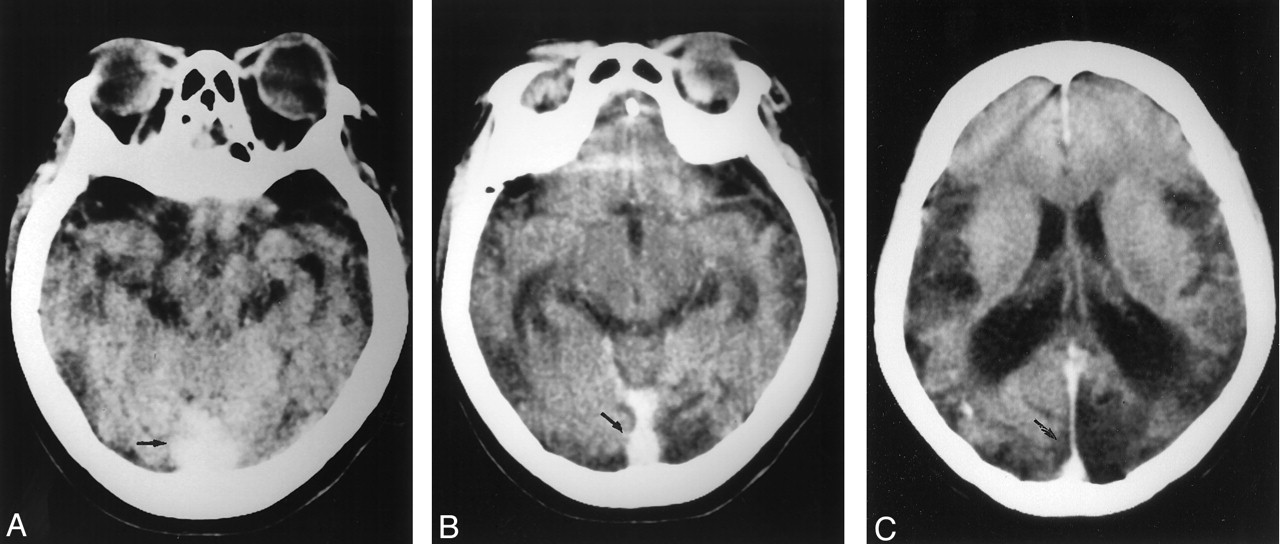
Unenhanced CT scans of the brain.
A, Hyperattenuation in midline of the posterior fossa (arrow) was initially misinterpreted as cerebellar hemorrhage and later misinterpreted as sinus thrombosis.
B and C, Higher sections reveal abnormally increased attenuation of straight sinus and superior sagittal sinus (arrows) caused by polycythemia.
A review of the unenhanced CT scans revealed marked atrophy and old left occipital infarct. The vein of Galen, straight sinus, and superior sagittal sinus were all noted to have abnormal increased attenuation. No Hounsfield units could be obtained, because the CT scans had been obtained at an outside institution. No cerebellar hemorrhage was present. A preliminary diagnosis of sagittal and straight sinus thrombosis was made on the basis of the CT findings. However, MR imaging and time-of-flight MR venography, which were ordered to confirm this diagnosis and to better evaluate the brain, revealed normal patency of these veins and sinuses (Fig 2). The patient’s hematocrit was noted to be 69.8, the hemoglobin was 20.8, and the partial pressure of oxygen was 76%. The increased signal intensity in the venous sinuses mimicking sinus thrombosis was caused by the increased radiographic attenuation of the excess hemoglobin protein in this patient, which was due to cyanotic congenital heart disease with severe polycythemia.

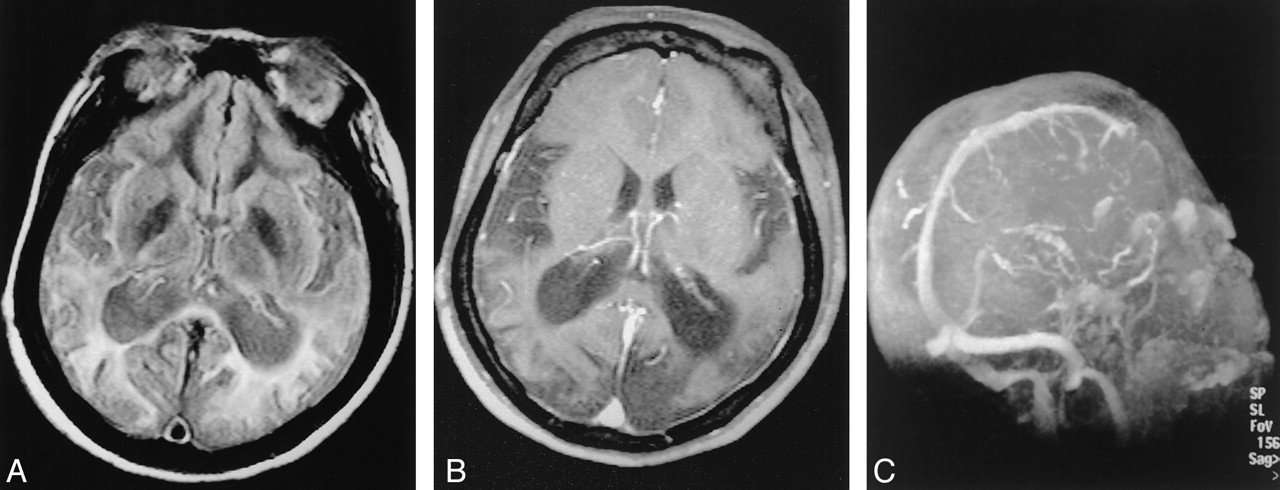
MR images and time-of-flight MR venogram of the brain.
A, Axial proton density-weighted (6200/105/1 [TR/TE/NEX]) MR image reveals normal flow voids in the straight sinus and sagittal sinus.
B, Contrast-enhanced T1-weighted (414/17/1) image reveals normal flow in the venous sinuses.
C, Time-of-flight MR venogram (30/6) shows normal flow in the straight sinus and superior sagittal sinus.
Discussion
Infants and children are among the most susceptible to venous sinus thrombosis. Unfortunately, the clinical diagnosis and treatment of this disease entity are frequently delayed. CT often reveals subtly increased radiographic attenuation in thrombosed veins or sinuses. Owing to the rarity of cerebral venous thrombosis, this abnormally increased attenuation in venous sinuses may initially be overlooked. Often the vascular abnormality is not recognized until subsequent infarction or hemorrhage occurs. Because of the limitations of CT, MR imaging with MR venography is the preferred and indicated diagnostic technique when cerebral venous thrombosis is suspected. However, most patients in this category initially, and often only, undergo non-contrast-enhanced CT. CT or catheter venography can substitute for MR venography, but MR imaging is more sensitive than is CT in detecting early parenchymal infarction.
New et al (1) noted increased attenuation of cerebral blood vessels in patients with polycythemia. This finding has also been recognized anecdotally among pediatric radiologists (2). Nonetheless, polycythemia occurs much less frequently than previously, because early correction of congenital conditions causing right to left shunts has become widespread. Our search of the radiology literature did not yield a specific description of the CT findings of polycythemia. Furthermore, venous thrombosis is a complication of polycythemia (3), and these two diagnoses may occur together and can be differentiated only by MR, CT, or catheter venography (4).
New et al (1) discovered a linear relationship between CT attenuation values and the hematocrit of whole blood preparations. The CT attenuation of hemoglobin was found to be largely due to its protein content. The iron in blood contributed only about 7% of its total attenuation. New showed that the attenuation of retracted clot was approximately 90%, twice the attenuation of normal intravascular blood (hematocrit level of 43). Reference to New’s work reveals that the attenuation of a hematocrit level of 70, as seen in our patient, is approximately 63% greater than the normal intravascular hematocrit level of 42. These findings were confirmed by Norman et al (4). Norman et al also demonstrated that the increased radiographic absorption seen in hematomas is primarily a reflection of hemoconcentration and the attenuation of hemoglobin protein. Calcium does not contribute to x-ray absorption, and iron makes only a minimal contribution to it.
Conclusion
CT visualization of intraarterial thrombus has been well described and has become especially useful in the early CT diagnosis of middle cerebral artery stroke (5, 6). It is important to remember that similarly increased attenuation of the cerebral venous sinuses may represent either polycythemia or venous thrombosis and to differentiate the two by reference to the patient’s hematocrit level. MR, CT, or catheter venography will still be necessary, because poycytemia is one of the conditions predisposing patients to cerebral venous sinus thrombosis.
Footnotes
Presented at the annual meeting of the Western Neuroradiology Society, Monterrey, CA, October 7, 2001.
- Received October 26, 2001.
- Accepted after revision January 24, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Meningeal vein and subarachnoid FLAIR hyperintensities in polycythaemia vera
- When a plain CT brain looks like contrast-enhanced- never forget polycythemia
- Current endovascular strategies for cerebral venous thrombosis: report of the SNIS Standards and Guidelines Committee
- Headache with markedly hypodense cerebral venous sinuses
- CT Density Measurement and H:H Ratio Are Useful in Diagnosing Acute Cerebral Venous Sinus Thrombosis
- Cerebral Venous Sinus Density on Noncontrast CT Correlates with Hematocrit