
Abstract
BACKGROUND AND PURPOSE: The aim of this study was to assess the effect of zero-filled interpolation (ZIP) on measurements of the cervical arteries because its benefits on the accuracy and precision of measurements in medium-sized arteries remains unknown.
METHODS: Three observers measured 36 computer-simulated vessels (2–6.8 mm) and 130 normal cervical vessels (assessed with two-dimensional time-of-flight MR angiography) from 512–, 256–, and 256–ZIP matrix source images. The accuracy and precision of measurement was assessed for each matrix by using the Student t test and F test of variance, respectively. The effect of vessel size and matrix placement on measurement error was determined by means of linear regression and the Student t test, respectively.
RESULTS: No significant difference was observed between simulated measurements obtained on the 512 matrix and their true value. The 256 matrix caused overestimation of vessel diameter compared with 512 matrix (mean bias, 0.3 mm for computer-simulated vessels and 0.1 mm for normal vessels). This effect was reduced with ZIP, by a mean of 0.1 mm for both groups (P < .03). Precision was not affected by the matrix size or ZIP, and vessel size and matrix placement did not alter the measurement error.
CONCLUSION: Vessel diameter is overestimated on 256-matrix MR angiographic source images. ZIP reduces this overestimation; however, the effect is small and unlikely to be clinically important.
MR angiography (MRA) offers a safe, noninvasive assessment of the cervical vasculature. One of its challenges, however, is that it fails to meet the high spatial resolution necessary for accurate arterial measurement without excessively long imaging times. Zero-filled interpolation (ZIP) offers a means of reducing pixel size without increasing the imaging time. However, its benefits on the accuracy and precision of measurements in medium-sized arteries remain unknown. The aim of this study was to examine the effect of ZIP on both computer-simulated vessels and images of the cervical arteries obtained with two-dimensional (2D) time-of-flight (TOF) MRA.
Methods
Computer Simulation
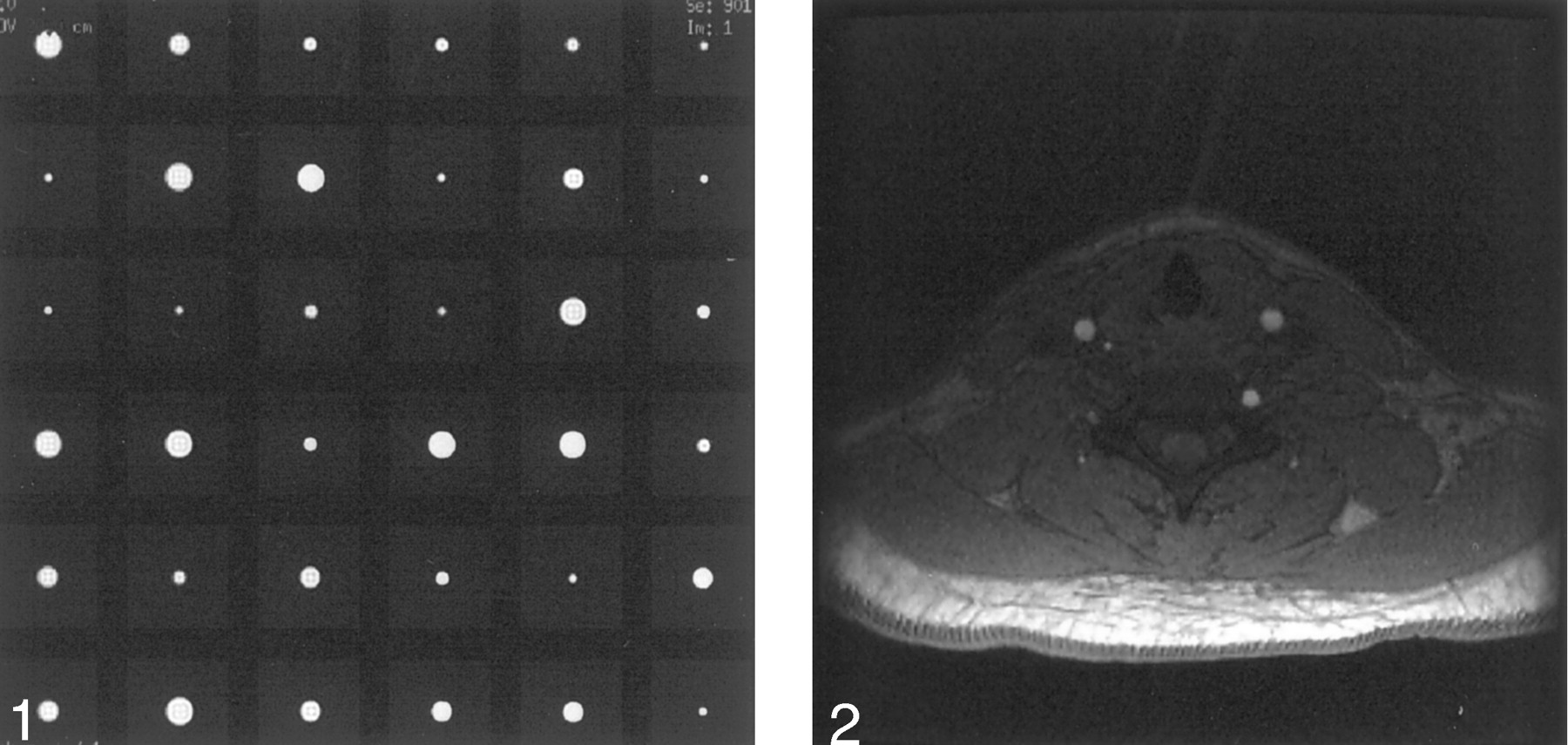
A cross-sectional representation of four vessels (diameters 2, 3.3, 5.1 and 6.8 mm) was generated on a computer workstation (Fig 1). Vessels were placed within a 512 matrix in three locations: 1) centered on the corner of four pixels, 2) moved 1/4 pixel superiorly and to the right, and 3) moved 1/2 pixel superiorly and to the right. The 512 matrix was manipulated to generate a 256 matrix of the vessels (peripheral k-space data discarded, 256 fast Fourier transform [FFT]) and a 256 ZIP matrix (peripheral k-space padded with zeroes, 512 FFT).

Computer-simulated vessels. Image shows computer-simulated vessels of four diameters (2, 3.3, 5.1 and 6.8 mm) displayed in three matrices (512, 256, and 256 ZIP) and in three pixel locations. Vessels are displayed in random order.
Healthy Volunteers
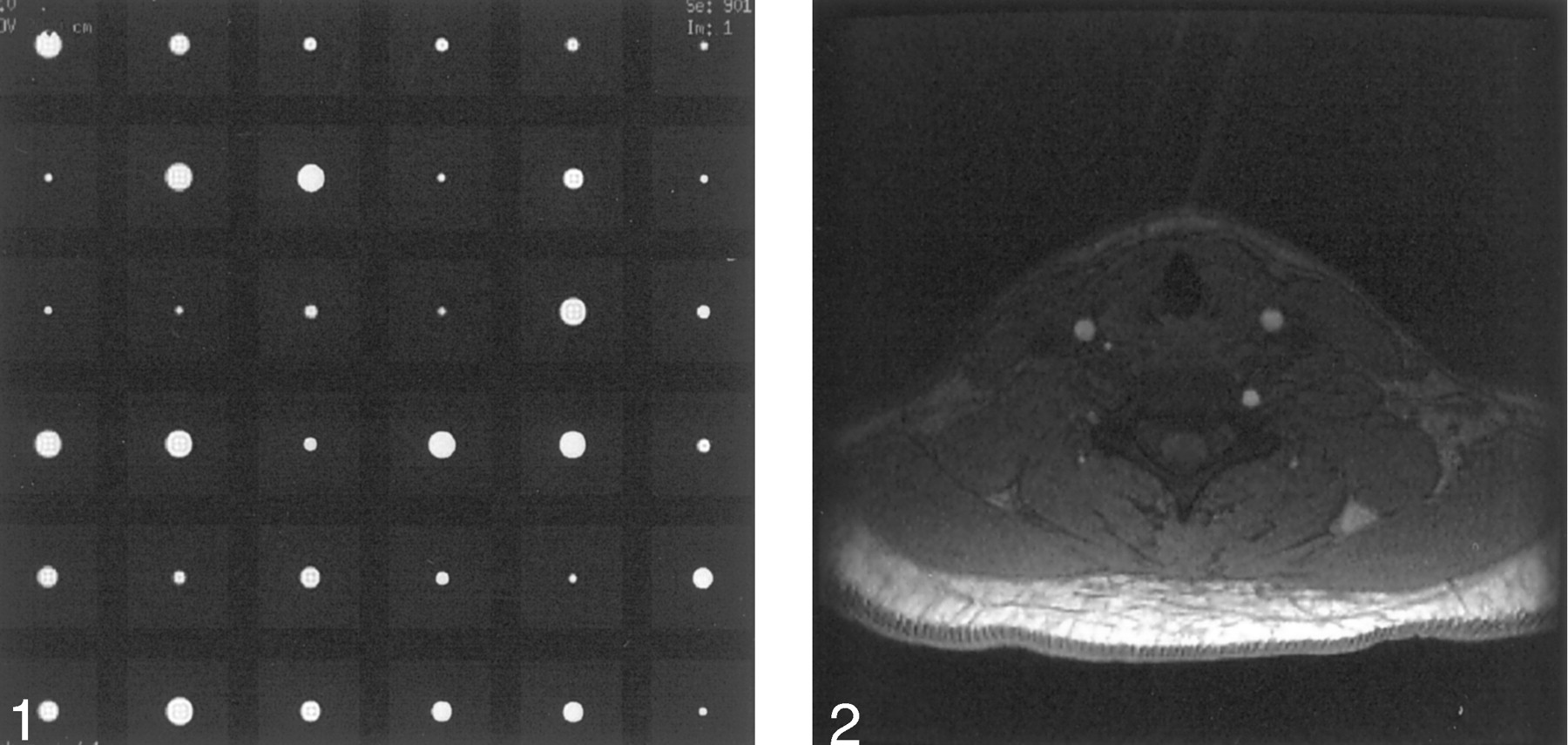
2D TOF MRA (512 × 512 matrix; TR/TE, 45/22; FOV, 20 cm; 1-mm section thickness; 12 seconds per section) of the cervical vessels was performed in five healthy volunteers, none of whom had evidence of vascular stenosis or occlusion on MRA. From each dataset, five widely spaced axial sections were chosen, and arteries coursing perpendicular to the section plane were identified (Fig 2). K-space data were manipulated to generate a 256 matrix and a 256 ZIP matrix, as described previously.

Typical 2D TOF MRA source image obtained in a healthy volunteer. Image shows a source image (512 × 512 matrix) used for vessel measurement.
Vessel Measurement
Three observers (K.P.F., J.P.K., J.E.H.) independently measured the transverse lumen of all computer-generated vessels (n = 36) and all normal cervical vessels (n = 130) on an Advantage Windows workstation (GE Medical Systems, Milwaukee, WI). Observers were blinded to type of matrix and the size of the vessel in both the computer-generated group and the normal-vessel group. Computer-generated vessels were displayed in random order. All vessels were magnified by a ratio of 4:1, and observers were allowed to alter the display window and level between the studies for different subjects. These levels, however, were fixed for the dataset for each subject.
Statistical Analysis
Multivariate regression was performed to ensure the independence of the measurements from the healthy volunteers. Accuracy was assessed by comparing the results with those of the chosen criterion standard (512 matrix [patient data] or the true size of the vessel size [simulated vessels]). For this, a paired Student t test was used. Precision was evaluated by comparing individual measurement variance to the mean for all three observers by using an F test. The effect of the size of the vessel on measurement error was assessed by means of linear regression by using the Bland-Altman plot and matrix placement with the Student t test.
Results
Computer Simulation
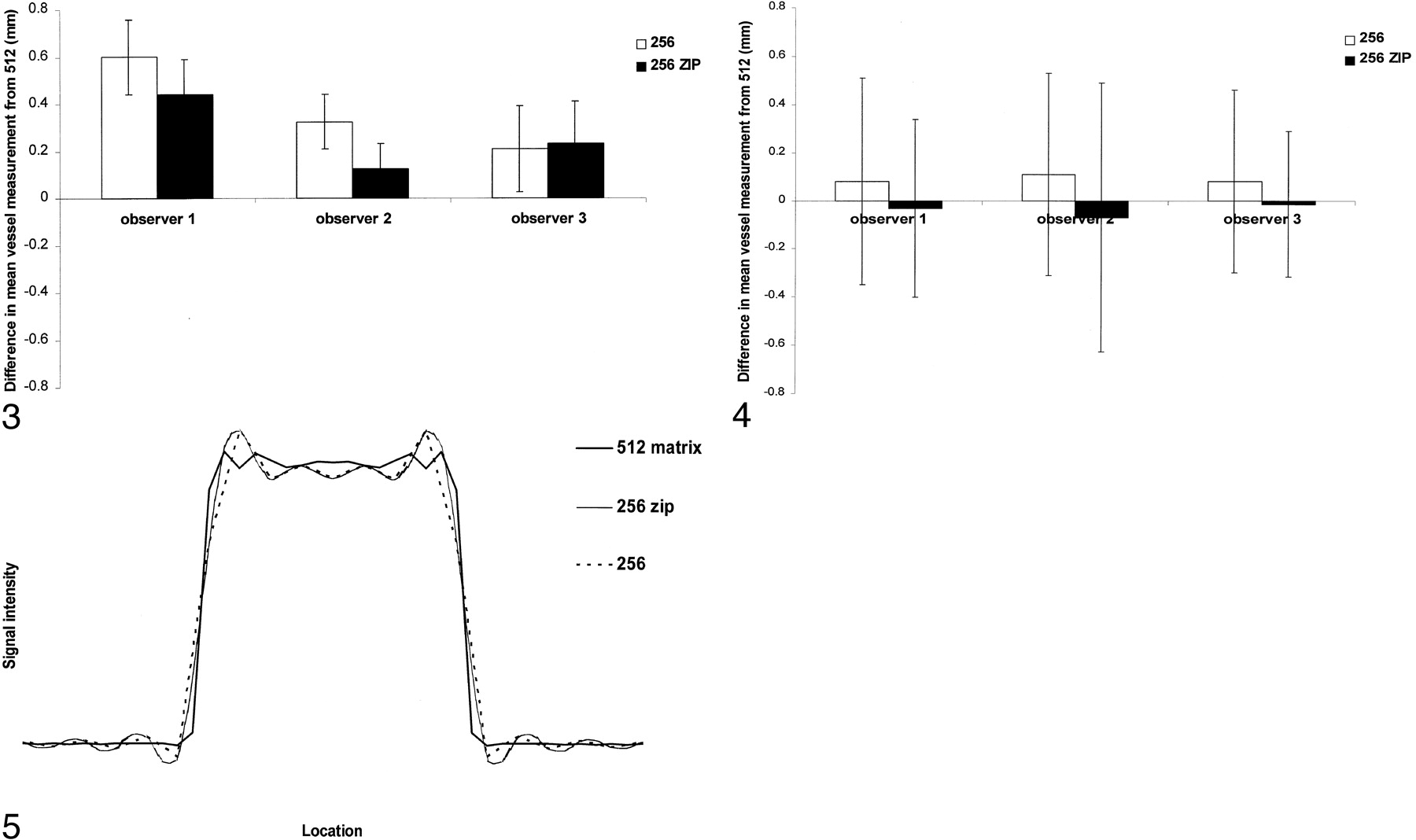
The true size of the vessel and the measurement on the 512 matrix did not significantly differ, both for individual observers and for the mean of all observers (mean true size, 4.3 mm ± 1.9 [SD]); 512-matrix mean, 4.2 mm ±1.8). The diameter of the vessel was overestimated on the 256 matrix, both for the mean of all observers (mean overestimation, 0.3 mm; vessel diameter. 4.6 mm ± 1.9) and for each individual, as shown in Figure 3 (P < .001). ZIP reduced this overestimation by 0.1 mm for the mean of all observers (mean vessel size, 4.5 mm ± 1.9) and for two of three individual observers (P < .03). There was no difference in variance between measurements obtained on any of the matrices or by individual observers. Similarly, there was no significant effect of either vessel size or placement with respect to the matrix on accuracy or precision of results.

Computer-simulated vessels: comparison of different matrix measurements. Graph shows differences in mean vessel measurements between the 512 matrix and the 256 and 256 ZIP matrices, with results for each observer shown separately. Error bars indicate the standard deviation of the measurements. Compared with the 512 matrix, both the 256 and 256 ZIP matrices consistently led to overestimation of the size of the vessel. With ZIP, however, a small but significant reduction in luminal diameter was observed for observers 1 and 2.
Healthy Volunteers
Results of multivariate regression confirmed that measurements obtained from the same subject were independent. The diameter of vessels was significantly overestimated on the 256 matrix, for the mean of all observers (256 matrix, mean: 4.5 mm ± 1.6; 512 matrix, 4.4 mm ±1.6) and for each individual, as shown in Figure 4 (P < .05). The 256 ZIP matrix improved accuracy for all observers (P < .001), giving measurements not significantly different from those of the 512 matrix (mean, 4.4 mm ± 1.6; range, 0.7–7.2 mm). There was no difference in variance between measurements obtained with any of the matrices or by individual observers. Similarly, the size of the vessel did not significantly affect either the accuracy or the precision of the results.

Normal vessels: comparison of different matrix measurements. Graph shows differences in mean vessel measurements between the 512 matrix and the 256 and 256 ZIP matrices; the results for each observer are shown separately. Error bars indicate the standard deviation of the measurements. Compared with the 512 matrix, the 256 matrix consistently led to overestimation of the size of the vessel. With ZIP, however, a small but significant reduction in luminal diameter was noted for all observers; these results were not significantly different from those of the 512 matrix.
Discussion
ZIP has been shown to improve the contrast and continuity of small vessels examined with intracranial MRA (1). In this study, we examined whether ZIP is also beneficial for MRA of medium-sized vessels, specifically addressing whether it reduces luminal measurement error. Our findings, both in computer-generated vessels and normal vessels suggest that ZIP leads to a very small improvement in the accuracy of luminal measurement.
Accurate measurement of carotid stenosis is key for determining whether endarterectomy is likely to be beneficial (2, 3). Conventional angiography is the current criterion standard for carotid measurement; however, it poses inherent risks, most notably a 1% risk of stroke (4). For this reason, interest in minimally or noninvasive imaging techniques, such as MRA, is great. One challenge of such techniques is to achieve an accuracy comparable to that of conventional angiography.
Traditionally, source images have been thought to offer the most accurate data source for MRA luminal measurements. Our findings, however, suggest that radiologists uniformly overestimate vessel diameters on 256-matrix source images. To help illustrate this clinical observation, the signal-intensity profile of one of the computer-simulated vessels is shown in Figure 5. These data are in keeping with the findings of Hoogeveen et al (5), who observed that the optimal threshold value for detection of a boundary of a vessel on TOF MRA was a signal intensity of 50% (ie, full width at half maximum). To overestimate the diameter of a vessel, its edge must be judged as having a signal intensity less than 50%, where its diameter appears wider. The relatively great interobserver variability likely reflects individual differences in judgment regarding the location of the edge of the vessel; window and level settings of the image are also likely to play a role. The measurement error observed with MRA source images is the opposite of that observed with maximum intensity projection data, with which the lumen of the vessel tends to be underestimated (6–8).

Signal-intensity profile of a computer-simulated vessel. Plot reveals that the 512, 256, and 256 ZIP matrices show the same vessel size at a signal intensity of approximately 50%. At signal intensities lower than this, the 256 matrix shows the largest vessel diameter, the 256 ZIP matrix a slightly smaller diameter, and 512 shows the smallest diameter.
Overestimation of vascular size on the 256 matrix was more marked in the computer-generated group than the normal group. This observation may reflect differences in signal intensity at the periphery of the vessel between the two groups. In normal vessels showing laminar flow, the signal intensity was maximal in the center of the vessels. In the computer-simulated vessels, however, signal intensity was uniform throughout their entire diameter. This artificial setting would likely alter the profile of the vessels and make them appear wider than they actually are. Furthermore, measurement of the lumen of the vessel in subjects may be complicated by edge blurring due to vessel-wall pulsation, which may result in the overestimation of the diameter of the vessel.
Our results have confirmed that 512-matrix MRA offers a small improvement in the accuracy of measurements in the cervical arteries. The reason for this change can be appreciated by referring to Figure 5: With signal intensities less than 50%, the vessel is narrower on the 512 matrix than on the 256 matrices. The use of this matrix offers a true improvement in resolution compared with the 256 matrix; however, this approach has the expense of extra imaging time as well a reduction in the signal-to-noise ratio (9, 10)
We observed a statistically significant improvement in the accuracy of 256-matrix MRA with the addition of ZIP. Although this technique reduces the pixel size to that of a 512 matrix by zero-padding of the periphery of k-space, it does so without a true alteration in resolution. However, the improvement in accuracy with ZIP was small, on the order of 0.1 mm. The importance of this effect depends on the size of the vessel: ZIP improves measurement accuracy by 10% for a 1-mm vessel, but the improvement is only 1% for a 10-mm vessel. For an internal carotid artery of 5 mm with a 50% stenosis, ZIP would improve the measurement accuracy by 1%; this rate increases to 1.4% in an artery with a 70% stenosis. This change would not significantly alter the grading of a carotid stenosis, and therefore, ZIP is unlikely to be a clinically important addition to MRA of the cervical vessels.
Measurement precision did not change with the matrix, the addition of ZIP, or between observers. However, vessel measurements in the computer-simulated vessels were more precise than those in healthy volunteers. Again, this finding likely represents the uniform signal intensity of the vessels rather than the variable signal intensity reduction seen at the edge of the normal vessels, which is due to laminar flow. We did not find any significant effect of vessel size or pixel placement on measurement error. This observation likely reflects the fact that our vessels were large enough to span multiple pixels (11).
Conclusion
We observed that luminal measurements performed on 256-matrix MRA source images commonly led to an overestimation of vessel size. This effect was reduced with ZIP, but the effect was small and therefore unlikely to be important in clinical imaging. By comparison, the 512 matrix offered significantly more accurate vessel measurements; however, this prolonged imaging time.
References
- Received January 21, 2002.
- Accepted after revision September 9, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.