
Abstract
Summary: Cerebral vasculitis presenting with intracranial hemorrhage is a rare but known entity. We discuss here the case of a 61-year-old woman presenting with subarachnoid hemorrhage. Cerebral angiography showed vasculitic changes involving the small and medium-sized vessels. She also had a concomitant herpes zoster rash on her back. A 3-month follow-up angiogram revealed partial resolution of the vasculitic changes.
Varicella-zoster vasculitis presenting with ischemic stroke is a known entity and has been described as one of the rare but important causes of stroke, especially in children (1, 2). Cerebral vasculitis associated with other conditions such as drug abuse, systemic lupus erythematosus, ulcerative colitis, pregnancy or postpartum period, and certain infectious processes such as tuberculosis or fungal infections has been known to cause intracranial hemorrhage (3–8); however, herpes vasculitis presenting with subarachnoid hemorrhage is not well described in the literature. We present here a patient with subarachnoid hemorrhage who also had concurrent dermatomal herpes zoster rash and whose cerebral angiogram showed findings consistent with small and medium-sized vessel arteritis.
Case Report
A 61-year-old woman presented with what she described as the worst headache of her life as well as with nausea and photophobia. She had a history of polio in childhood with resultant bilateral weakness of the lower extremities. At admission, she was awake, alert, well oriented, afebrile, and normotensive. Her mental status and cranial nerve examinations were normal. Motor strength was 5/5 in both upper extremities, 4/5 in the right lower extremity, and 0/5 in the left lower extremity. On examination, she was noted to have an asymptomatic vascular maculopapular rash located on her back that extended anteriorly around her trunk in the T11 dermatomic area. She denied having noticed this until 3 days before admission. She had a history of chicken pox in childhood.
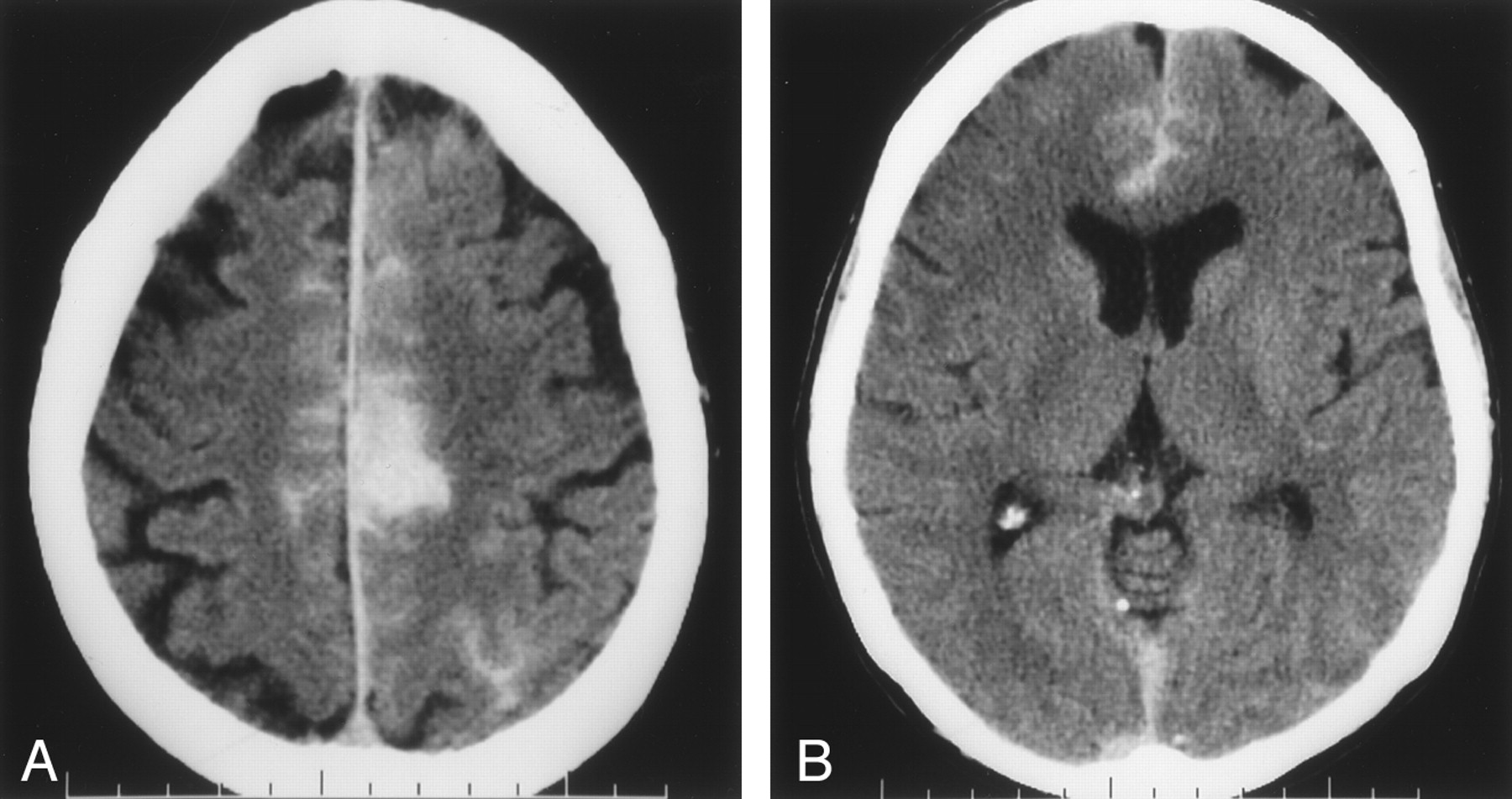
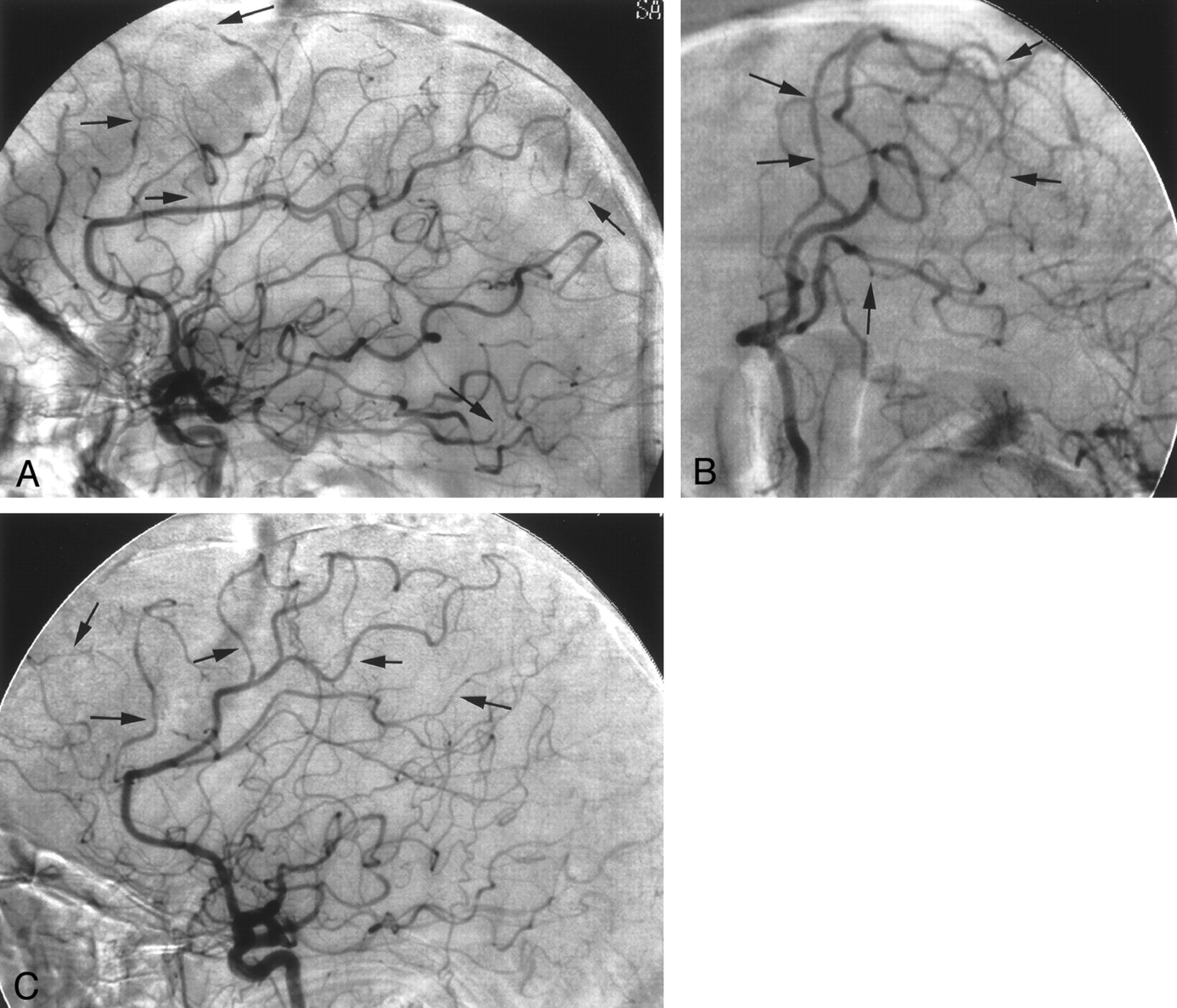
A CT scan of the patient’s head showed Fischer grade III subarachnoid hemorrhage, mainly in the anterior interhemispheric fissure and in left frontal region, with a small para-midline intracerebral hematoma (Fig 1). Cerebral angiography conducted the same day did not reveal an aneurysm or a vascular malformation; however, multiple short segments of narrowing and beading were seen involving the small and medium-sized vessels, suggestive of vasculitis (Fig 2). Vasculitic changes were seen scattered diffusely in anterior, as well as posterior, circulation and even away from the site of subarachnoid hemorrhage. Diffusion-weighted MR imaging did not reveal any cortical or subcortical ischemic lesions.

Axial CT, showing subarachnoid hemorrhage, mainly in the anterior interhemispheric fissure (B) and left para-midline hematoma (A).

Lateral (A) and anteroposterior oblique (B) left internal carotid arteriograms and right internal carotid lateral (C) arteriograms, showing multiple scattered segments (arrows) of irregularity and narrowing involving the small and medium-sized vessels.
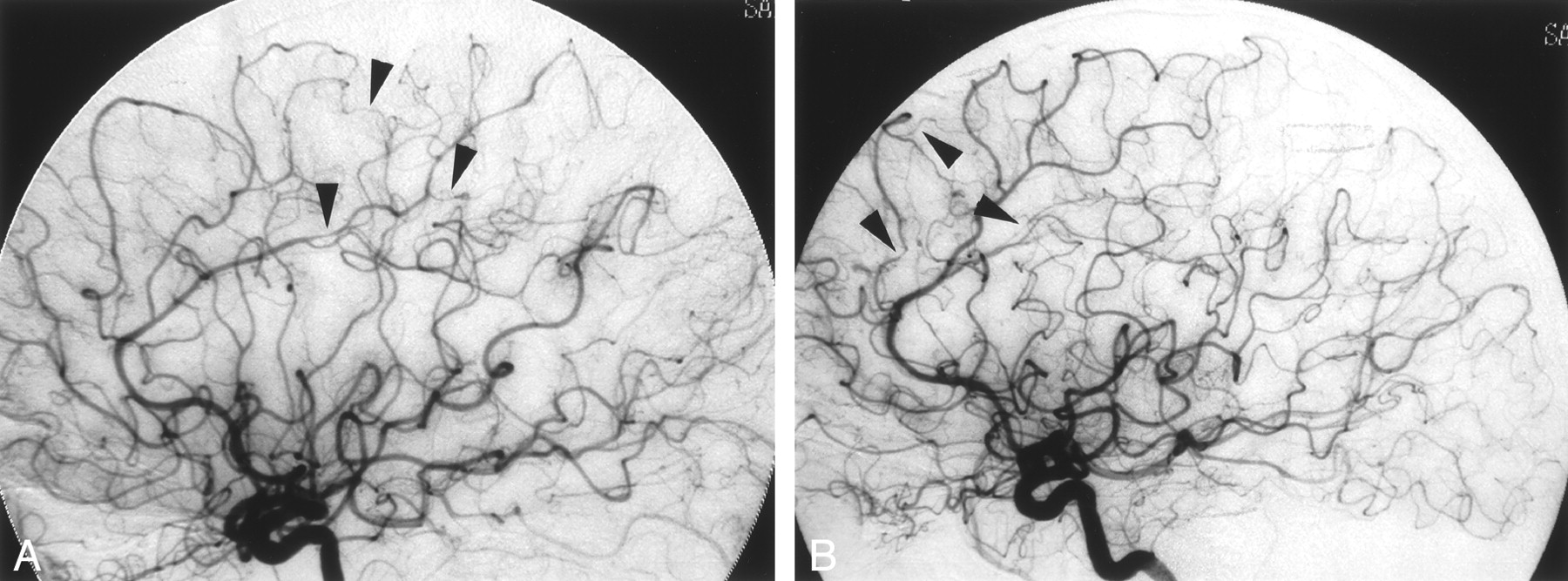
Her systemic vasculitis workup was negative for extractable nuclear and cytoplasmic antibodies, anti-double-stranded DNA, and rheumatoid factor. Erythrocyte sedimentation rate was normal, but C-reactive protein levels were 5.9 mg/dL (normal range 0.0–0.6 mg/dL). Skin culture was positive for the varicella-zoster virus (VZV). The patient was HIV negative and also did not have a history of any systemic illness or neoplasm. Laboratory investigations did not show any bleeding diathesis. A lumbar puncture was not performed because of the location of the herpes rash. While in the hospital, the patient was treated with intravenous acyclovir and pulsed methylprednisolone and was continued on oral acyclovir and prednisone after discharge. Follow-up angiography performed 3 months later showed resolution of some of the segmental narrowing involving the small and medium-sized vessels, although many of the lesions were still present, suggestive of scarring and/or persistent vasculitis (Fig 3). Her C-reactive protein levels were still elevated (3.1 mg/dL). Hence, she has begun immunosuppressive therapy and is doing well clinically on follow-up.

Left (A) and right (B) internal carotid lateral arteriograms (3 months’ follow-up), showing partial resolution of the vasculitic changes and persistence of some of the narrowed segments (arrowheads).
Discussion
Central nervous system complications of VZV include encephalitis, aseptic meningitis, myelitis, acute cerebellar ataxia, Reye syndrome, Ramsay Hunt syndrome, and, rarely, stroke (2, 9). All of these complications are recognized to be due to vasculitis affecting small or large vessels. VZV, an alpha herpesvirus found exclusively in humans, causes chicken pox, usually in childhood. After the acute illness resolves, the virus becomes latent in the neurons of the cranial and spinal ganglia of nearly all patients, with no corresponding signs or symptoms. In immunocompromised or elderly patients, VZV may reactivate to produce a dermatomal rash with radicular pain (shingles), on rare occasions rash without pain (zoster sine herpete), or even severe persistent pain (postherpetic neuralgia). VZV can also spread to intracranial arteries, usually involving the large vessels in immunocompetent patients. In immunocompromised individuals, particularly those with cancer or AIDS, the virus affects small vessels and may lead to a more severe and protracted course causing ventriculitis, meningoencephalitis, or myelitis (9).
VZV is thought to spread directly along the intracranial branches of the trigeminal nerve to the ipsilateral arterial walls in patients with herpes zoster opthalmicus (HZO), presenting with delayed contralateral hemiparesis (10). The latent period between the onset of HZO and neurologic complaints is usually a few days to 6 months. Vasculitis has, however, been observed in patients with dermatomal herpes zoster infection without trigeminal nerve involvement, as seen in the present case. Hematogenous seeding or spreading via the sympathetic nervous system is another mechanism suggested for virus spread to the intracranial vessels (11, 12). In our patient, varicella rash and hemorrhagic stroke occurred almost simultaneously, and angiographic findings of vasculitis were generalized, rather than localized, to one area or one side. This again suggests probable hematogenous seeding or spreading via the sympathetic nervous system rather than the perineural spread pattern of trigeminovascular connections. Herpes vasculitis without any evidence of varicella rash has also been described, though rarely (13).
Various histopathologic studies of patients with varicella vasculitis have demonstrated the virus in the vessel wall, which may induce a noncytolytic infection of the smooth muscle cells in the media and functional damage to the vascular endothelium. This may result in thrombosis and promote subendothelial proliferation of smooth muscle cells, fibroblasts, and collagen, leading to areas of stenosis and occlusion (14); however, pathologic findings may differ during acute and chronic disease and are influenced by the host-immune response (15, 16). In immunocompetent individuals, a spectrum of vascular involvement exists, ranging from necrotizing arteritis to moderate, chronic vascular inflammation, thrombosis without inflammation, remote vascular occlusion resembling atherosclerosis of the small vessels of the nervous system, and stenosis or thrombotic occlusion of large vessels in the circle of Willis. VZV penetrates to a greater extent in immunocompromised patients, resulting in small vessel angiopathy (multifocal leukoencephalopathy) or ependymitis (ventriculitis) (9). Autopsy studies in these cases have shown frank invasion by the virus, sometimes with more extensive necrosis and inflammation than that seen in immunocompetent patients (17). Primary (granulomatous) angitis of the central nervous system has been reported to be associated with herpes zoster infection, but whether these are causally related remains uncertain (18).
In the present study, the patient was not immunocompromised but had generalized small and medium-sized vessel vasculopathy rather than the commonly seen localized large vessel involvement in immunocompetent individuals. The virus probably had more extensive and aggressive tissue penetration causing necrotizing angitis and intracranial hemorrhage, despite the presence of any other risk factor for bleeding. Fibrinoid necrosis of large vessels has been shown to cause intracranial hemorrhage in vasculitis associated with methamphetamine abuse (3). True central nervous system vasculitis associated with systemic lupus erythematosus occurs in less than 10% of patients (5) and may cause ischemia or hemorrhage (6).
Polymerase chain reaction (PCR) analysis of CSF is a sensitive and specific test for VZV DNA. Detection of VZV antibody in the CSF, even in the absence of PCR-amplifiable VZV DNA, further supports the diagnosis in cases of suspicious varicella-zoster infection of the nervous system (9). In the present case, however, CSF examination could not be performed, because the lumbar puncture was relatively contraindicated by the presence of the herpes rash on the patient’s back. Cerebral angiography showed typical small and medium-sized vessel vasculitic changes, in addition to the presence of VZV cultured from the skin vesicles, which led to the diagnosis of varicella-zoster vasculitis, and the patient was started on antiviral therapy. A 3-month follow-up angiogram revealed partial resolution of some of the segmental narrowing. Initially, narrowing results from reversible inflammation and vasospasm. Serial angiography may show improvement in cerebral vasculitis patients with a clinical response to therapy (19), as seen in the present case. Persistent irreversible angiographic features appear secondary to scarring (19).
Conclusion
MR imaging may be useful in localizing ischemic lesions associated with cerebral vasculitis; however, MR imaging is a poor indicator of the presence or absence of vasculitis (20). Normal MR findings in a patient with angiographic evidence of vasculitis may ultimately require brain biopsy for a definitive diagnosis (20). MR angiography can be used as a noninvasive technique and may substitute conventional angiography in cases with typical vascular changes (21). Conventional angiography also has a poor sensitivity and specificity to diagnose cerebral vasculitis (22). Thus, cerebral vasculitis is a rare cause of intracranial hemorrhage and must be suspected in a patient with a history of recent varicella-zoster infection even if the angiogram does not show vasculitic changes. An accurate diagnosis, however, should not rely on any single method and is possible only with careful clinical, radiographic, and pathologic correlation.
References
- Received July 25, 2002.
- Accepted after revision September 6, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}