
Abstract
Summary: We present a case of Guglielmi detachable coil extraction into a microcatheter after coil detachment during embolization of a superior hypophyseal artery aneurysm; extraction was a result of the suction generated during pusher-wire withdrawal. Experimental simulations using many coil and microcatheter combinations were used to identify factors that contribute to the likelihood of this phenomenon.
Endovascular treatment of intracranial aneurysms with Guglielmi detachable coils (GDCs) is associated with lower procedure-related morbidity and superior clinical outcomes compared with those of surgery (1, 2). Avoidance of technical complications is mandatory if coil embolization is to gain universal acceptance as the standard of care for treatment of these lesions.
We report an instance of GDC displacement, after confirmation of coil detachment, into a microcatheter by suction generated during pusher-wire withdrawal. Experimental simulations using various coil designs were conducted to identify microcatheter-coil combinations that require the most judicious wire-removal technique.
Case Report
A 49-year-old woman with a history of sarcoidosis underwent MR imaging and MR angiography; imaging findings revealed left carotid ring and cavernous internal carotid aneurysms. Conventional angiography confirmed the presence of an 8-mm superomedially directed left superior hypophyseal artery aneurysm, a 12-mm aneurysm of the horizontal cavernous segment, and a 2-mm carotid-ophthalmic aneurysm.
Coil embolization of the superior hypophyseal aneurysm was undertaken with the patient under general anesthesia. The balloon remodeling technique was used by positioning a Sentry-10 balloon (Target Therapeutics, Fremont, CA) across the aneurysm neck. A Prowler-Plus microcatheter (Cordis, Miami Lakes, FL) was used to catheterize the aneurysm, and a GDC-10 2D 8 mm × 30 mm coil (Target Therapeutics) was delivered into the aneurysm. A predetachment angiogram showed satisfactory coil position. The microcatheter tip was noted to be displaced from the confines of the coil ball (Fig 1A) and was subsequently repositioned before coil detachment by using a GDC Synergy (Target Therapeutics) power supply. The pusher wire was withdrawn slowly under fluoroscopic observation for the first 10 cm to confirm detachment and then withdrawn more rapidly from the microcatheter and discarded. Fluoroscopy revealed a segment of coil within the distal 2 cm of the microcatheter (Fig 1B). A Trupush (Cordis) coil pusher was used to redeliver the remainder of the coil into the aneurysm. Four additional coils were used, and total occlusion of the aneurysm was achieved. The patient remained neurologically intact and was discharged from hospital uneventfully on the second postoperative day.

A, Unsubtracted right anterior-oblique projection before detachment of the first coil. The microcatheter tip is displaced outside the coil mass, but the entire coil has been delivered into the aneurysm (black arrow). The pusher-wire marker overlays the proximal marker of the microcatheter (arrowhead). Note balloon catheter in situ for balloon-remodeling technique (white arrow).
B, Unsubtracted projection after coil detachment and withdrawal of pusher-wire shows 1–2 cm of coil retraction into the microcatheter (arrows)
Experimental Simulation
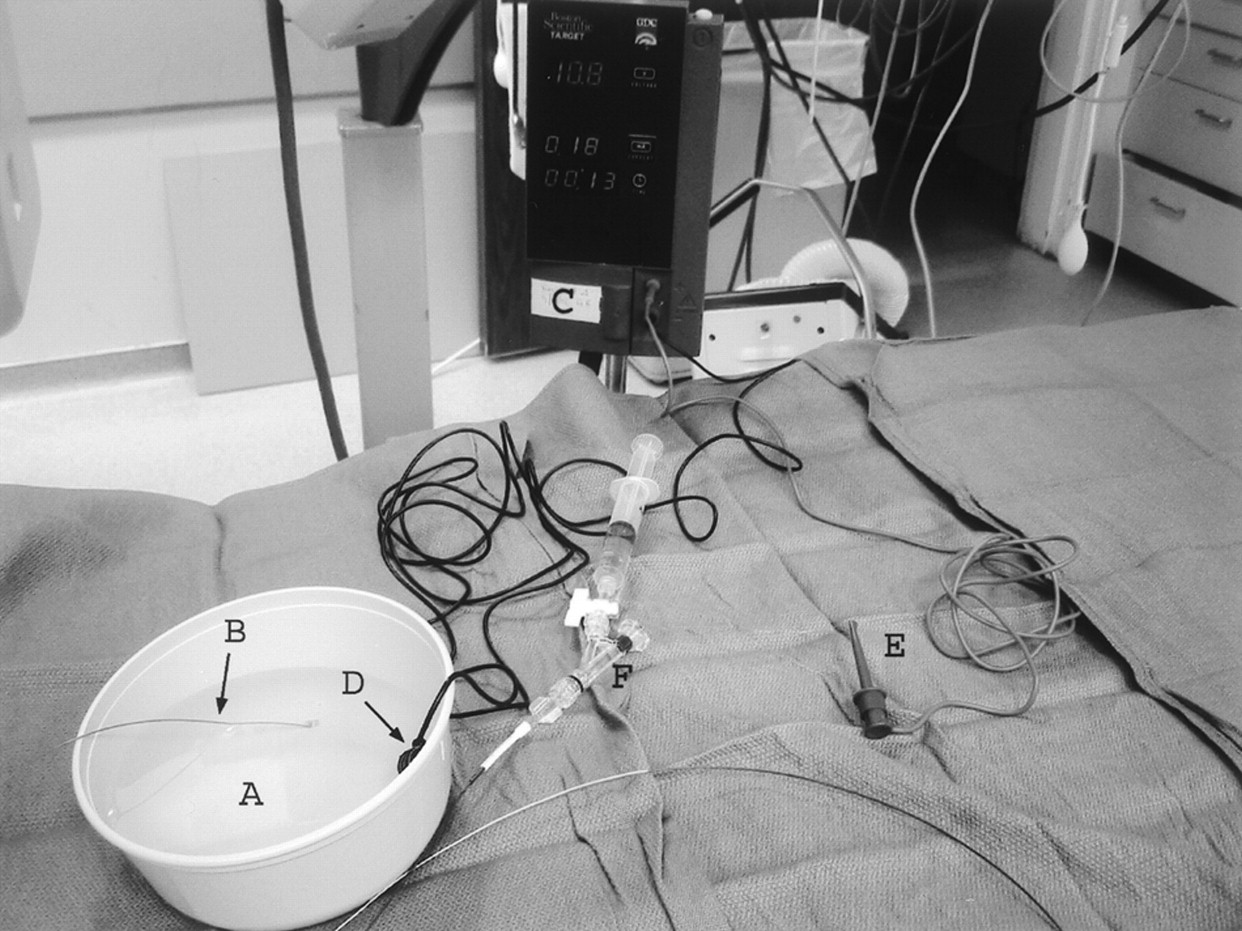
Five varieties of GDC were advanced through Prowler-Plus (Cordis) and Excel-14 (Target Therapeutics) microcatheters into a plastic bowl containing 0.9% NaCl solution. Each coil was advanced under fluoroscopic observation until the detachment zone was just within the tip of the microcatheter. The grounding cable was placed into the saline bowl, and the positive lead was connected to the end of the pusher wire. Each coil was detached by using a Synergy (Target Therapeutics) power supply (Fig 2).

Experimental simulation components.
A, Bowl containing normal saline.
B, Microcatheter containing coil.
C, Power supply.
D, Grounding electrode.
E, Positive electrode attached to pusher wire.
F, Perfusion sidearm.
If the coil end had displaced relative to the microcatheter tip after detachment, the pusher wire was removed and the coil was siphoned into the microcatheter tip by applying suction with a 10-mL syringe. The pusher wire was subsequently reinserted into the microcatheter and advanced under fluoroscopic observation until it was within 5 cm of the catheter tip.
If the coil end remained within the microcatheter tip after detachment, the pusher wire was then slowly withdrawn under fluoroscopic observation to confirm detachment and then readvanced to within 5 cm of the catheter tip.
A perfusion sidearm was used to maintain a closed system during pusher-wire withdrawal. The system was carefully purged of air by injecting saline into the side port before tightening the hemostatic valve.
Under fluoroscopic observation, the pusher wire was briskly withdrawn by extending the operator’s arm while grasping the end of the pusher wire (Figs 3 and 4). The results with different coil and microcatheter combinations are summarized in Table 1.

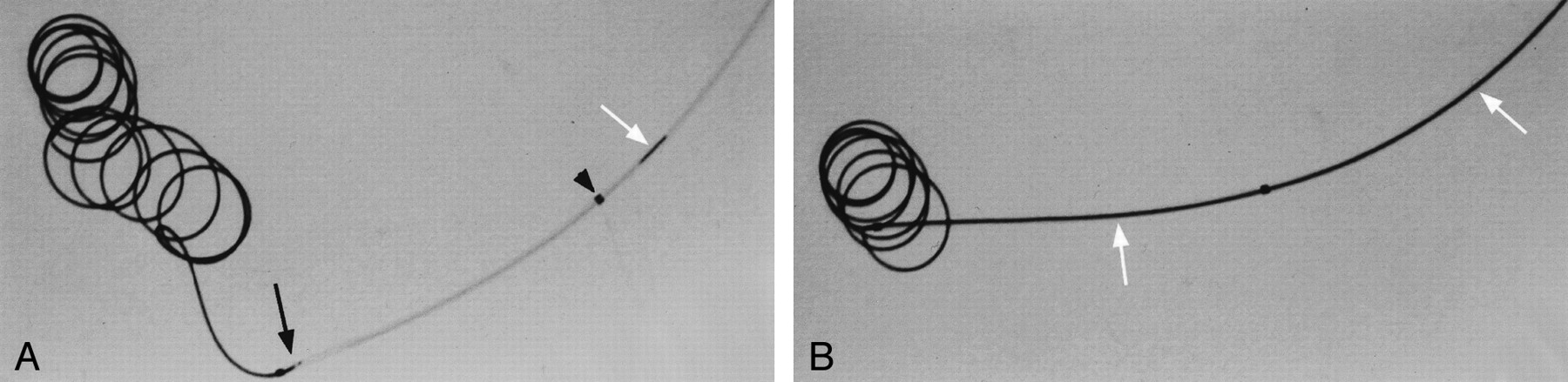
Digital radiographs of experimental simulation achieved by using Excel-14 microcatheter with GDC-10 2D, 8 mm × 30 cm
A, After coil detachment, before removal of pusher-wire. Note position of coil end (black arrow) and pusher-wire marker (white arrow) near proximal marker of microcatheter (arrowhead).
B, After brisk withdrawal of pusher wire. Note substantial coil retraction into microcatheter (white arrows)

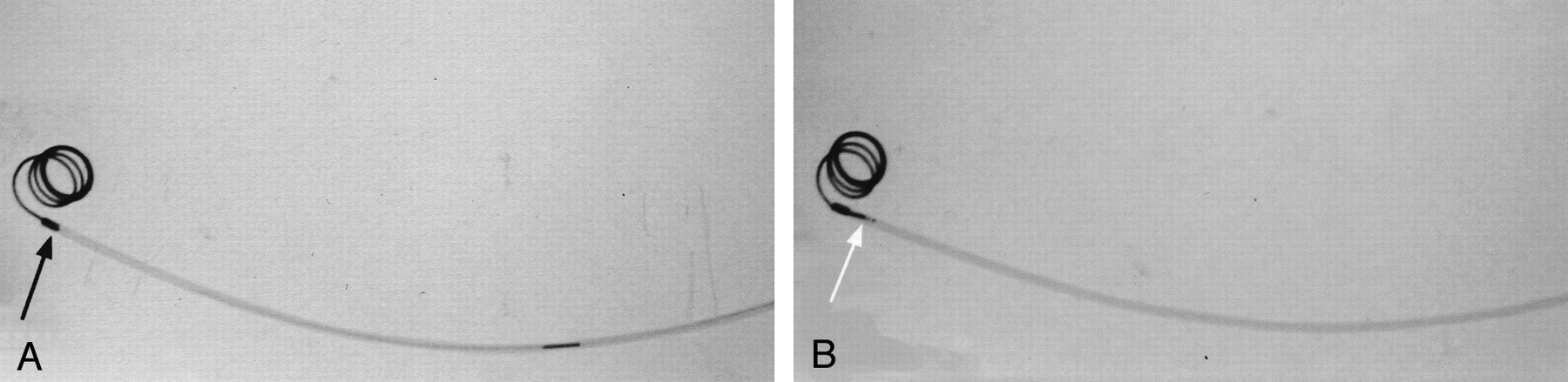
Digital radiographs of experimental simulation by using Prowler-Plus microcatheter with GDC-10 ultrasoft, 4 mm × 6 cm.
A, After coil detachment, before removal of pusher-wire. Note position of coil end (black arrow) within microcatheter tip.
B, After brisk withdrawal of pusher wire. Note minimal coil retraction into microcatheter (white arrow).
Experimental simulation results
Discussion
Generation of suction within a microcatheter during guidewire removal is a phenomenon familiar to interventional neuroradiologists. Routine dripping of saline into the hub of the microcatheter during guidewire removal prevents the siphoning of air into the system and reduces the potential for air embolus (3).
We describe an instance of GDC extraction into a microcatheter after coil detachment due to suction generated during withdrawal of the pusher wire. Using an experimental simulation, we identified variables that alter the likelihood of coil displacement by suction.
There are three diameters relevant to coil construction. The core wire diameter is the width of wire that is wound to create the primary coil diameter. The secondary coil diameter is determined by winding the primary coil during the manufacturing process and refers to the diameter of unrestrained coil loops.
Frictional forces increase as primary coil diameter approaches the internal diameter (ID) of the microcatheter; GDC extraction by suction is more likely to occur with large-ID microcatheters. In our simulation, the difference was evidenced by easier aspiration of a coil through a 0.021-inch ID Prowler Plus (Cordis) compared with the 0.017-inch ID Excel-14 (Target Therapeutics) microcatheter.
In vitro studies have shown that decreasing the secondary diameter of the coil increases the frictional force within the microcatheter (4). Coils with smaller secondary diameters should therefore be less susceptible to extraction by suction. This was confirmed in our simulation by the relative ease of extracting an 8 mm × 30 cm coil compared with 4-mm- and 2-mm-diameter coils of the same primary coil diameter (GDC-10 series).
Complex-shaped coils exert far more frictional force than a simple helical coil with an identical secondary coil diameter (4) and should therefore be less susceptible to extraction by suction. Coil length has been shown to be relatively unimportant in determining the frictional force within a microcatheter (4). This accounts for the inability in our simulation to extract a GDC-10 3D-shaped 8 mm × 20 cm coil and the relative ease of extracting a longer GDC-10, 8 mm × 30 cm, helical coil.
Precise positioning of the coil end with respect to the microcatheter tip can be affected by manufacturing tolerances in the microcatheter-detachable coil assembly. Should the intermarker distance of the microcatheter be greater than 3 cm or the length of pusher wire between the coil detachment zone and the marker shorter than nominal, alignment of the pusher-wire marker with the proximal marker of the microcatheter can result in coil detachment within the microcatheter tip, facilitating suction extraction during removal of the pusher wire.
As coils are progressively deposited into an aneurysm, their strands intermingle, reducing the propensity for dislodgement. We theorize, therefore, that the first coil will have the highest likelihood for extraction because of the suction phenomenon.
Conclusion
Under some circumstances, rapid removal of the pusher wire can result in aspiration of a portion of a detached coil into a microcatheter. Pusher wires should therefore be withdrawn slowly and under fluoroscopic observation.
- Received June 3, 2002.
- Accepted after revision October 3, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}