
Abstract
Summary: We report MR findings in a case of a giant cell reparative granuloma involving the temporal lobe in a middle-aged man. On MR images, most of the mass was hypointense on T1-weighted images, hypointense on T2-weighted images, and mildly enhanced on postcontrast T1-weighted images. The hypointensity on T2-weighted images corresponded to areas of hemorrhage and hemosiderin deposition on pathologic correlation.
Giant cell reparative granuloma (GCRG) is a rare benign condition of unknown cause occurring most commonly in the mandible. It has also been reported to occur in the long bone, paranasal sinus, orbital region, cranial vault, and temporal bone (1–7). In the English-language medical literature, only a few cases of GCRG of the temporal bone have been described (2, 3, 4–8), and, to our knowledge, MR findings with pathologic correlation of GCRG have not been reported. We report a case of GCRG of the temporal bone and describe the MR findings correlated with the pathologic findings in this rare tumor.
Case Report
A 50-year-old man presented with a 2-year history of hearing disturbance, tinnitus, and a feeling of fullness in his right ear. He was found to have a mass in the right external auditory canal. He denied a history of trauma or surgery to the right ear.
He underwent CT and MR imaging of the head before biopsy and subsequent excision. CT demonstrated a lytic-appearing region in the anterior portion of the right temporal bone with bone destruction of the mastoid air cells adjacent to the mastoid antrum and a soft tissue attenuation in the external auditory canal extending to the scutum (Fig 1A).

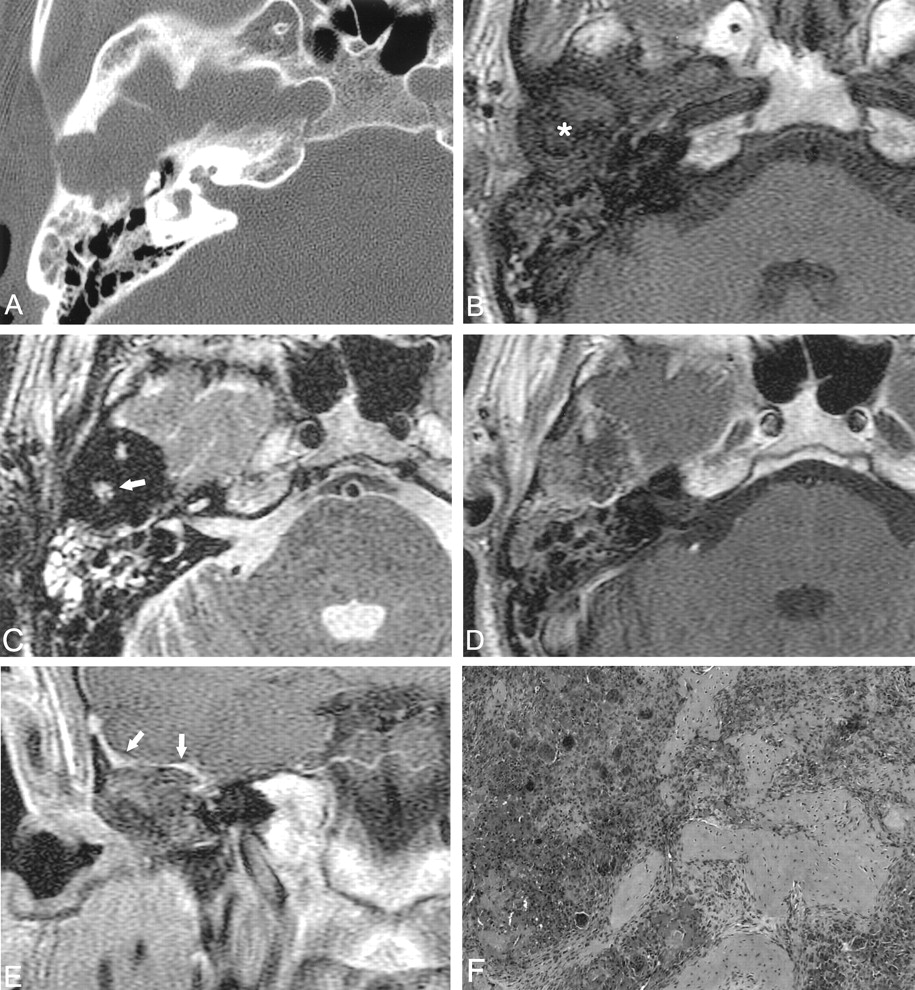
Images of a 50-year-old man with a 2-year history of hearing disturbance, tinnitus, and a feeling of fullness in his right ear.
A, Axial CT image demonstrates bone destruction and soft tissue replacement of the anterior portion of the right temporal bone.
B, Axial T1-weighted MR image (416/9 [TR/TE]) shows a lesion (asterisk [*]) that is hypointense to the muscles in the right temporal area. The lesion occupies the anterior portion of the mastoid and extends to the middle cranial fossa.
C, Axial T2-weighted MR image (4000/126) shows that the lesion has mainly hypointense and several hyperintense foci in its central portion (arrow). The dark appearance of the lesion corresponds to areas of hemorrhage and hemosiderin deposition found at pathologic correlation.
D and E, Axial (D) and coronal (E) contrast-enhanced T1-weighted MR images (416/9) reveal mild heterogeneous enhancement of the lesion and show thickening and enhancement of the adjacent dura (E, arrows).
F, Photomicrograph shows that the tumor is composed mostly of clumps of reactive giant cells around abundant hemorrhagic foci mixed with osteoid formation.
The lesion appeared as a region of decreased signal intensity on T1-weighted images (Fig 1B). On T2-weighted images, the lesion appeared dark(Fig 1C). After contrast material administration (gadopenetate dimeglumine), there was mild enhancement of the soft tissue component of the lesion (Fig 1D and E) in the temporal bone with thickening and enhancement of the adjacent dura (Fig 1E).
Excision of the mass was performed by means of a transmastoid approach. A fragile brown mass occupied the mastoid air cells, external auditory canal, and the epitympanum. There was also erosion of the tegmen tympani and attachment to the adjacent dura. Histopathologic examination showed granulomatous lesions composed of reactive giant cells around abundant hemorrhagic foci and osteoid formation in most parts of the lesion, and a small amount of fibrous stroma was intermingled with these regions. The pathologic diagnosis was GCRG arising from temporal bone.
The patient was grossly free of symptoms for 5 months at the time of this writing.
Discussion
Since Jaffe described the GCRG as a local reparative reaction to intraosseus hemorrhage induced by trauma (1) in 1953, there has been much debate over the pathogenesis of GCRG, including possible infectious (5) and developmental (9) causes, but no single theory has gained wide acceptance. Nonetheless, a general consensus has been reached on differentiating GCRG from giant cell tumor (GCT) on the basis of their clinical and histologic characteristics. Clinically, GCRG has a more benign course than GCT, which reportedly has a higher incidence of recurrence, metastasis, and malignant transformation. In various studies, GCT of the long bones tends to have a high recurrence rate of between 45% and 62%. Lung metastasis occurs in 1–6% of cases (10). On the other hand, GCRG is thought to have a low rate of recurrence, ranging between 10% and 15% (4, 5, 9, 10). There has not been a documented case of metastasis from GCRG. Histologically, GCRG has fewer multinucleated giant cells than GCT, and these cells tend to have fewer nuclei with increased cytoplasm and irregular shapes and to cluster in uneven patches of foci (3, 4–7, 10). By contrast, the giant cells in GCT are more evenly distributed and have a more uniform appearance (4, 5, 7, 10). There is an increased incidence of hemosiderin, hemorrhage, and osteoid in GCRG than in GCT (3, 4–7, 10). Other less frequently mentioned characteristics include increased fibrosis and the absence of necrosis in GCRG and a greater incidence of mitotic figures in GCT (4, 10).
The reported CT findings of GCRG of the temporal bone were those of a nonspecific lytic and expansile lesion, as in this case (4, 5, 7).
Reported MR findings of GCRG of the temporal bone have included hypointensity to the brain parenchyma on T1-weighted images, hypointensity on T2-weighted images, and mild contrast enhancement (7). These findings correspond with our MR findings in this case. In these two cases, the hypointensity on T2-weighted images corresponded well to the areas of hemorrhage and hemosiderin deposition on pathologic correlation.
The pathologic differentiation of GCRG from GCT includes brown tumor associated with hyperparathyroidism, fibrous dysplasia, and aneurysmal bone cyst. The clinical-radiologic correlation can be helpful to the histopathologist in distinguishing the lesions. Brown tumor of hyperparathyroidism can be excluded by measuring the serum calcium and phosphate levels and by performing a parathyroid hormone assay. Fibrous dysplasia can be excluded because of the radiologic features demonstrating a ground-glass appearance on CT scans and low signal intensity on all MR imaging sequences with intense enhancement (11). Aneurysmal bone cysts histologically reveal large pools of blood lined by flat spindle cells separated by a thin, fibrous septa (11) and have characteristic radiologic features demonstrating a multilocular “soap bubble” or “honeycomb” radiolucency. On MR, images the classic findings of aneurysmal bone cyst are those of multiple cysts with fluid-fluid levels (11).
Treatment modalities for GCRG usually consist of curettage, surgical excision, or radiation therapy. Complete surgical excision has been recommended over simple curettage, because of the high incidence of recurrence with incomplete removal. When these tumors are not amenable to surgical resection, radiation therapy has been advocated. The main concern with radiation therapy has been the potential for sarcomatous transformation, although now that megavoltage has supplanted orthovoltage radiation as the standard mode of therapy, not nearly as many instances of sarcomatous transformation have been reported (2).
Conclusion
GCRG is a rare benign condition that may involve the temporal bone. On MR images, it is a well-defined, lobulated, contoured mass. It is hypointense to brain parenchyma on T1-weighted images, hypointense on T2-weighted images, and is associated with mild contrast enhancement. GCRG should be considered in the differential diagnosis of masses involving the temporal bone.
References
- Received September 13, 2002.
- Accepted after revision October 18, 2002.
- Accepted after revision October 18, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.