
Article Figures & Data
Figures
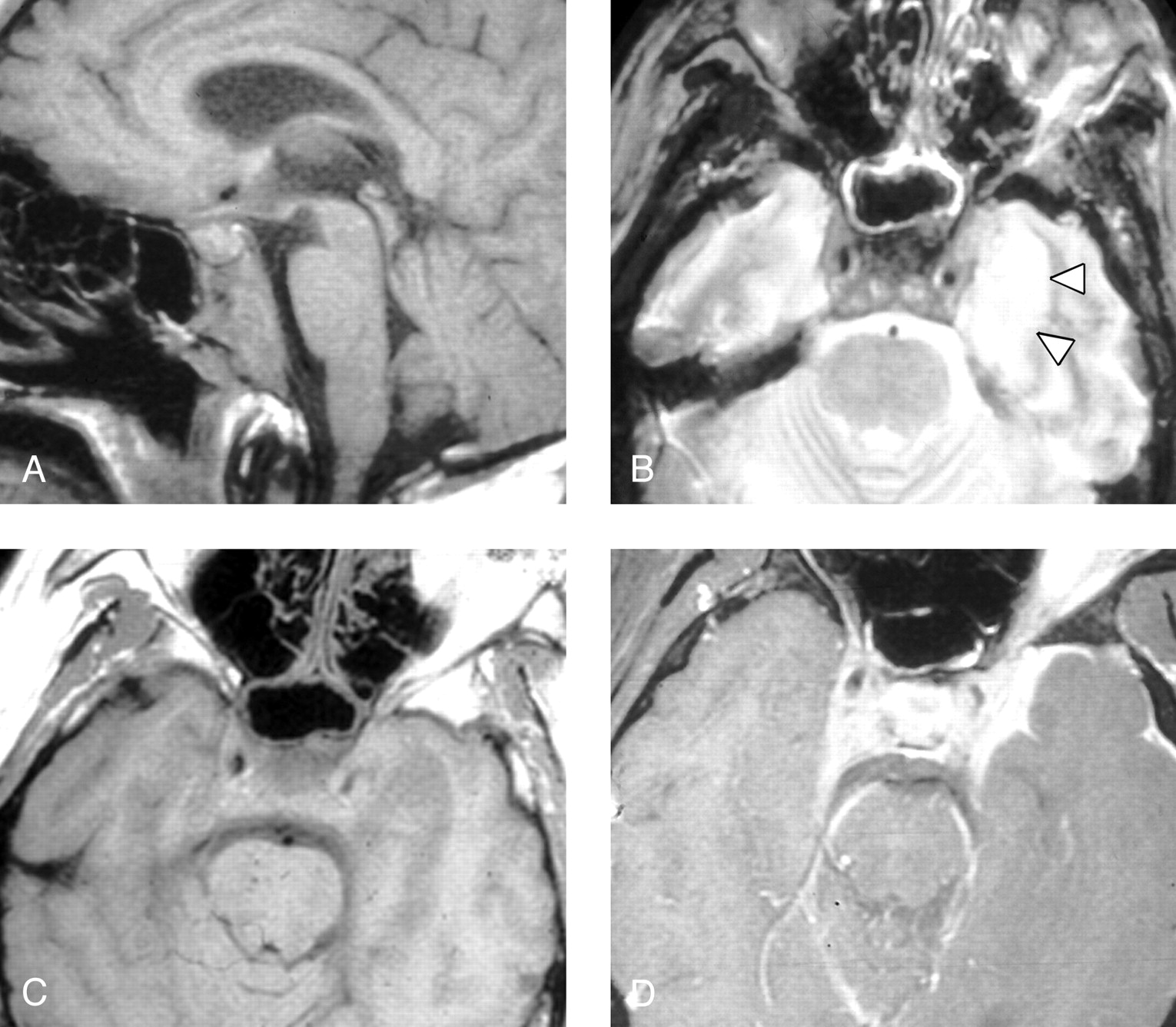
- Fig 1.
Patient 1, a 50-year-old man presenting with a severe headache, diplopia, and the sensation of a “thick” tongue.
A, Sagittal T1-weighted image (600/11/2 [TR/TE/NEX]) demonstrates abnormally low signal intensity in the inferior clivus.
B, Axial T1-weighted image (600/11/2) demonstrates abnormal soft tissue isointense to muscle infiltrating submucosally within the nasopharyngeal soft tissues, extending posteriorly to abut the carotid arteries (arrowheads), and replacing the normal hyperintense fatty marrow within the lower clivus.
C, Axial T2-weighted fast spin-echo image with fat saturation (4000/102/2) demonstrates mildly increased signal intensity within the infiltrated soft tissue as compared with normal muscle. In addition, there is fluid in the mastoid air cells and middle ear cavities bilaterally, presumably related to Eustachian tube dysfunction or obstruction or both.
D, Contrast-enhanced axial T1-weighted spin-echo image with fat saturation (600/11/2) demonstrates moderately intense enhancement of the infiltrative soft tissue. Some areas of nonenhancement may represent areas of infarcted or necrotic muscle.
E, Axial T1-weighted spin-echo image (600/11/2) from a follow-up MR examination 16 months after the initial study demonstrates normalization of clival signal intensity (white arrows), as well as considerable reduction in bulk of the previously noted abnormal pre- and paraclival soft tissue.
F, Contrast-enhanced axial T1-weighted spin-echo image with fat saturation (600/11/2) from the same follow-up examination demonstrates marked reduction of enhancement, with a normal appearance to the nasopharynx and prevertebral muscles. An ill-defined area of linear enhancement just at and anterior to the hypoglossal canal on the right (arrow) is likely extending along the course of the hypoglossal nerve. Of note, this patient’s hypoglossal palsy has persisted despite resolution of all other symptoms.
- Fig 2.
Patient 6, a 35-year-old man presenting with headache and bilateral deficits of CN III, VI, VII, X, and XII. The patient had been previously treated with steroids and oral antibiotics for paranasal sinus inflammatory disease.
A, Sagittal T1-weighted MR image (600/11/2) shows diffuse low signal intensity in the clivus, with prominence of preclival soft tissue and thickening of the retroclival dura.
B, Axial T2-weighted spin-echo image (2500/80/0.75) demonstrates mild circumferential mucosal thickening in the sphenoid sinus. Abnormal low signal intensity soft tissue is present within the cavernous sinuses bilaterally, and there is mild narrowing of the left cavernous carotid flow void. High signal intensity in the left temporal lobe (arrowheads) is present, presumably due to either focal cerebritis or localized venous ischemia/infarction.
C, Axial T1-weighted spin-echo image (600/11/2) demonstrates abnormal soft tissue in the cavernous sinuses bilaterally and swelling of the left temporal lobe with poor definition of adjacent cerebral sulci. The left internal carotid artery appears patent but narrowed. Fat within the orbits and sphenotemporal buttresses is unremarkable.
D, Contrast-enhanced axial T1-weighted image (600/11/2) with fat saturation demonstrates dural and leptomeningeal enhancement along the anterior left temporal lobe, as well as expansion of the cavernous sinuses bilaterally and extension of abnormal enhancement along the tentorium. Apparent enhancement of the left orbital fat is secondary to a failure of fat saturation in the inferior orbit of this somewhat rotated patient. Note that the orbital fat is seen to be normal in panel C.
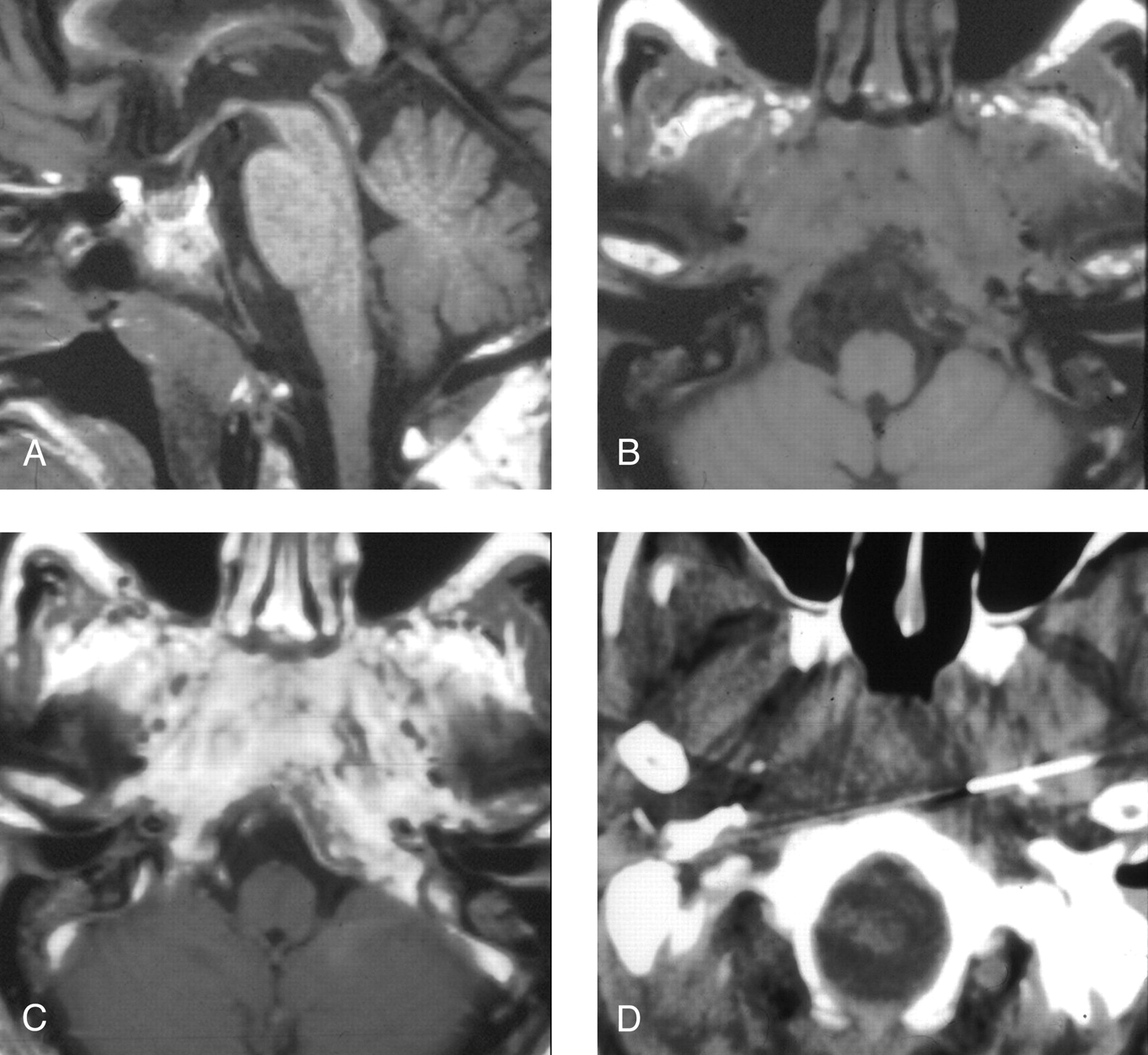
- Fig 3.
Patient 4, a 72-year-old man presenting with headache, dysphagia, and progressive hoarseness.
A, Sagittal T1-weighted image (600/11/2) demonstrates abnormally hypointense signal in the lower clivus.
B, Axial T1-weighted image (600/11/2) demonstrates abnormal soft tissue isointense to muscle infiltrating submucosally into the nasopharyngeal tissues, around the carotid arteries, and back to abut the abnormal clivus.
C, Contrast-enhanced axial T1-weighted image (600/11/2) demonstrates marked enhancement within the infiltrated tissue.
D, CT-guided FNA of the preclival soft tissues shows the needle tips anterior to the lower clivus.
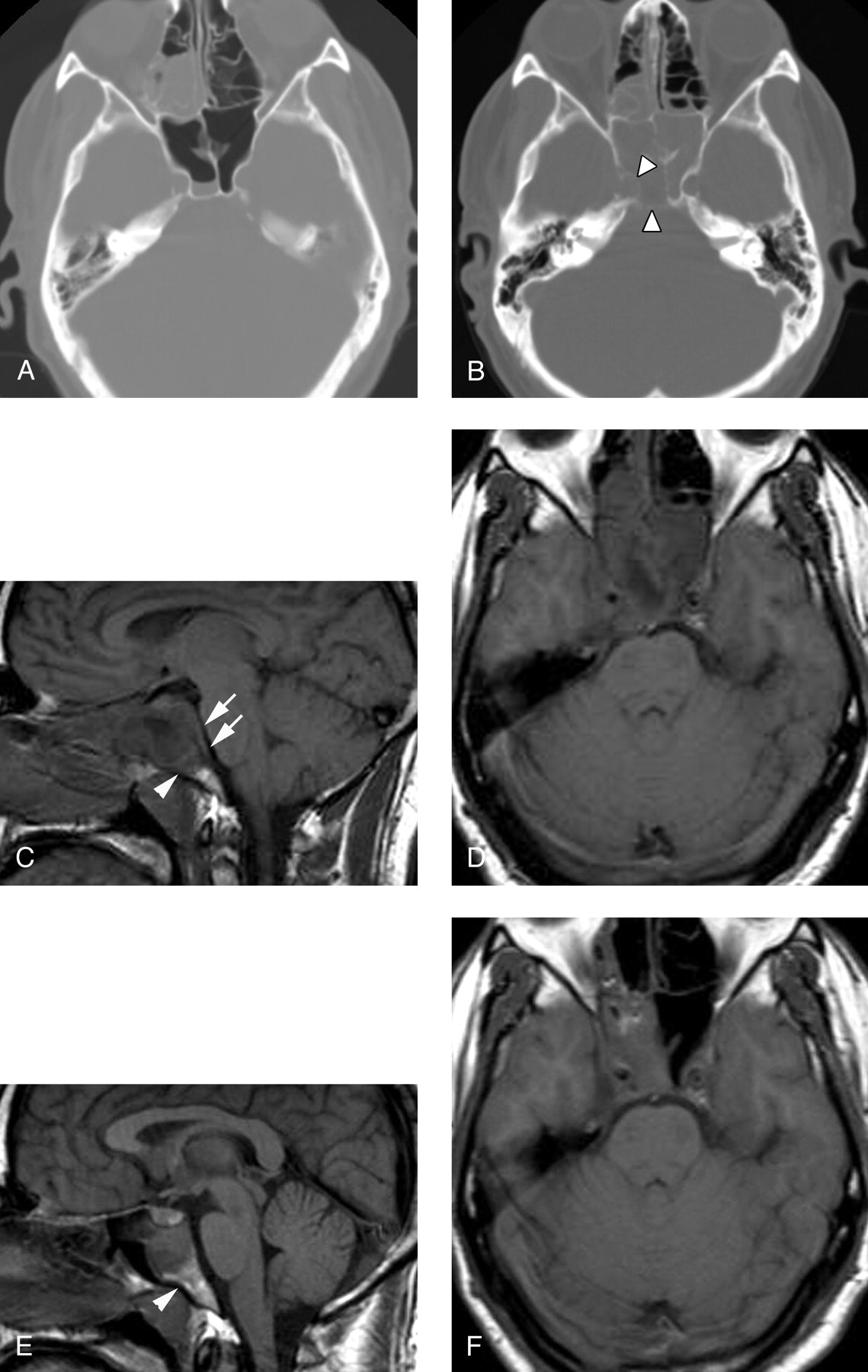
- Fig 4.
Patient 5, a 33-year-old man presenting with severe headache and sinus congestion.
A, Unenhanced axial CT image (bone window) demonstrates mucosal thickening in the right ethmoid sinus and an air-fluid level in the right sphenoid sinus. The bony walls of the sphenoid sinus are normal. Diagnosis of acute-on-chronic sinusitis was made and Septra and a decongestant were prescribed for the patient.
B, Three weeks later, the patient returned with continued headache and new diplopia on right lateral gaze. Unenhanced axial CT image (bone window) demonstrates segmental erosion of the bony wall of a completely opacified sphenoid sinus (arrowheads).
C, Sagittal T1-weighted spin-echo image (600/11/2) demonstrates abnormal hypointense signal intensity in the upper clivus (arrowhead) and thickening of the retroclival dura (arrows). The sphenoid sinus is filled with fluid and soft tissue.
D, Axial T1-weighted image (600/11/2) demonstrates abnormal soft tissue in the right cavernous sinus, with preservation of the right carotid flow void. Abnormal clival hypointensity is present, as is extensive inflammatory disease of the sphenoid and posterior ethmoid sinuses.
E, Sagittal T1-weighted spin-echo image (600/11/2) after 1 month of intravenous antibiotic therapy demonstrates normalization of signal intensity in the clivus (arrowhead), as well as a reduction in inflammatory sinus disease and resolution of the retroclival dural thickening.
F, Axial T1-weighted spin-echo image (600/11/2) from the same follow-up examination also demonstrates improvement in sinus disease. Abnormal soft tissue persists in the right cavernous sinus but is reduced in volume. The patient’s CN VI palsy had resolved by the time of this follow-up examination.




Tables
- TABLE 1:
Clinical characteristics of patients with atypical central skull base osteomyelitis
Patient (no.) Age (y)/Sex Risk Factors Biopsy Performed Organism Isolated Cranial Neuropathies 1 50/M Diabetes mellitus, chronic sinusitis CT fine needle aspiration Eikenella corrodens VI, IX, X, XII 2 13/M Diabetes mellitus Sphenoidotomy Staph aureus, Serratia marcescens, Aspergillus niger V2, VI, VII, VIII, IX, X, XI, XII 3 38/M HIV positive, replacement steroids Autopsy Aspergillus fumigatus VI, VII 4 72/M Diabetes mellitus CT fine needle aspiration Pseudomonas aeruginosa IX, X 5 33/M Chronic sinusitis Sphenoidotomy Group C Streptococcus VI 6 35/M Diabetes mellitus, steroids Craniotomy Streptococcus milleri III, VI, VII, IX, X, XII Patient (no.) Abnormal SI in Clivus Preclival ST Mass T1 SI in Clivus T2 SI in Clivus Postcontrast Enhancement ST in CS ST in MC IC Extension 1 Y Y Low High Y N N N 2 Y Y Low Heterogeneous Y Y* Y N 3 Y Y Low Heterogeneous Y Y* Y Y 4 Y Y Low High Y N N N 5 Y Y Low High Y Y Y N 6 Y Y Low High Y Y* Y Y Note.—Signal intensity in clivus is compared with that of normal fatty marrow. SI indicates signal intensity; ST, soft tissue; CS, cavernous sinus; MC, Meckel’s cave; IC, intracranial. Intracranial extension implies extension beyond CS or MC, involving dura or brain parenchyma or both.
↵* = associated carotid narrowing or occlusion.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dynamic Contrast-Enhanced MRI Parameters and Normalized ADC Values Could Aid Differentiation of Skull Base Osteomyelitis from Nasopharyngeal Cancer
- Skull Base Osteomyelitis: A Comprehensive Imaging Review
- Extensive skull base osteomyelitis found radiologically after resolution of otitis externa
- Severe destructive nasopharyngeal granulomatosis with polyangiitis with superimposed skull base Pseudomonas aeruginosa osteomyelitis
- A diagnostic dilemma of central skull base osteomyelitis mimicking neoplasia in a diabetic patient
- Diffusion MR Imaging Features of Skull Base Osteomyelitis Compared with Skull Base Malignancy