
Abstract
Summary: A 62-year-old woman had sudden-onset headache and posterior neck pain, and a subarachnoid hemorrhage was revealed by unenhanced CT. Both multi-detector CT angiography and digital subtraction angiography were performed and revealed a small intracanalicular aneurysm of the left anterior inferior cerebellar artery. The patient underwent successful retrosigmoid craniectomy and trapping of the aneurysm. This case shows the ability of multi-detector CT angiography to indicate bony landmarks that can alter the surgical approach.
Intracanalicular aneurysms of the anterior inferior cerebellar artery are rare. Multi-detector CT angiography offers excellent visualization of the bony anatomy, which is critical in considering treatment options.
Case Report
We report the case of a 62-year-old woman who presented with sudden-onset headache and posterior neck pain. A neurologic examination revealed that cranial nerves II through XII were intact. A motor examination revealed full strength in the left upper and lower extremities and in the right lower extremity. The patient was slightly weak in the right upper extremity, graded 4+/5. Sensation was intact to full touch. The results of a cerebellar examination were normal. The patient’s speech was fluent, and she was alert and oriented to person, place, and time. Unenhanced CT of the brain revealed subarachnoid hemorrhage in the posterior fossa, adjacent to the left side of the pons.
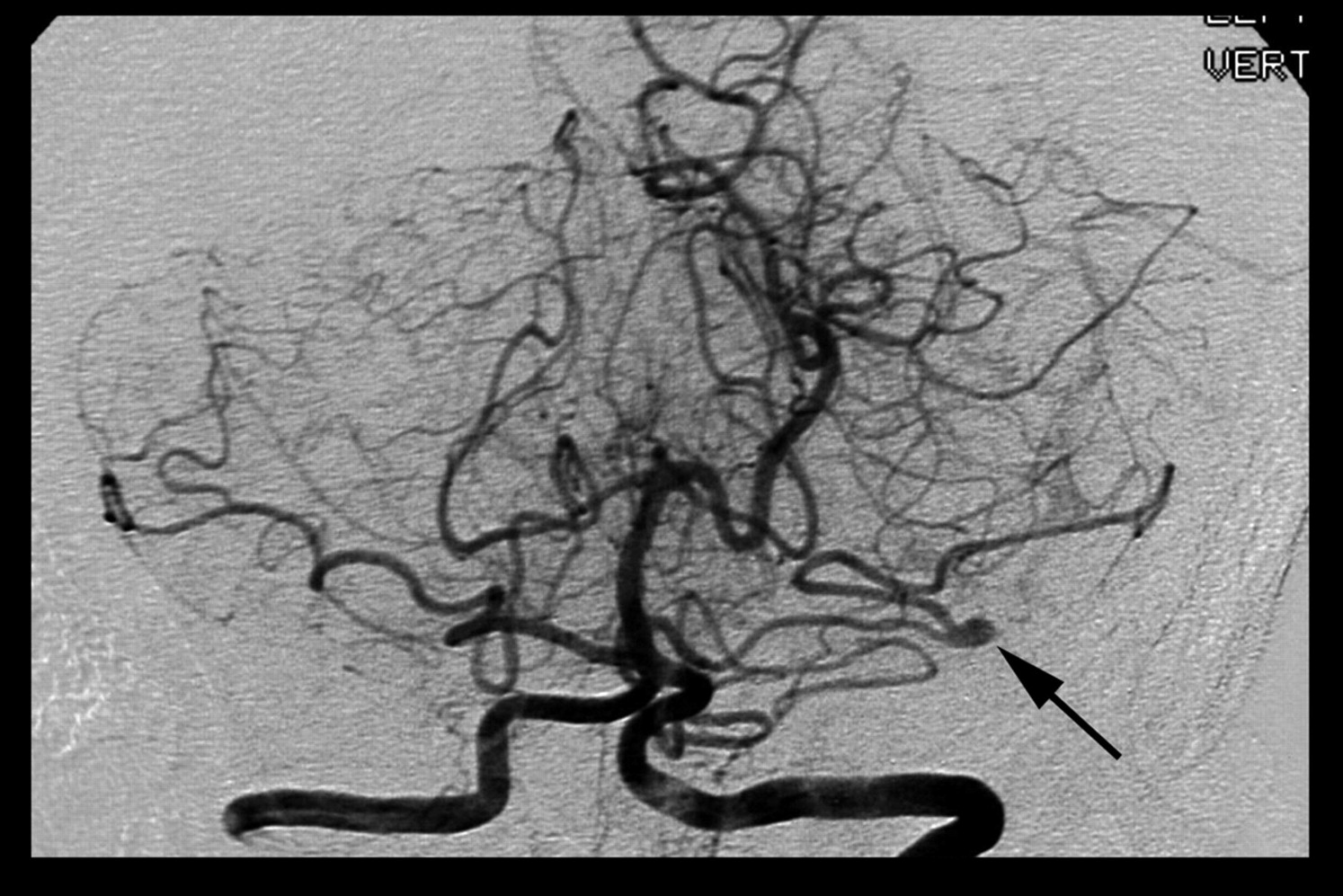
The patient underwent transfemoral intra-arterial digital subtraction angiography performed for further evaluation. The left vertebral artery injection (Fig 1) revealed a small aneurysm of the left anterior inferior cerebellar artery. For further delineation of the relationship of this aneurysm to bony landmarks, the patient underwent multi-detector CT angiography on a GE LightSpeed Qx/I unit (General Electric Medical Systems, Milwuakee, WI). Scanning parameters were 1.25-mm collimation, 0.5-mm section interval, pitch of three (high quality mode), 140 kVp, 200 maS, and display field of view of 14.0 cm. The scanning time was 31 s. The scanning volume was from the superior aspect of the ring of the C1 vertebra to above the level of the lateral ventricles. A total of 120 mL of low osmolar contrast medium (300 mg I/mL) was administered by using a power injector at a rate of 4 mL/s via a peripheral 18-gauge IV line. The multi-detector CT angiographic examination confirmed the small aneurysm and also clearly defined the intracanalicular location (Fig 2).

Frontal projection digital subtraction angiogram, left vertebral artery injection, shows a small aneurysm (arrow) arising from a branch of the left anterior inferior cerebellar artery.

Axial CT angiogram again shows the small left-sided aneurysm (arrow). The intracanalicular location is clearly shown.
On hospital day 3, the patient underwent a left retrosigmoid craniectomy. The lateral cerebellum was retracted to expose the VIIth and VIIIth cranial nerve complex and the origin of the internal auditory canal. This aneurysm, which was thought to be a congenital berry type aneurysm, was trapped. Postoperative angiography showed satisfactory aneurysm occlusion (Fig 3). Postoperatively, the patient did well and was discharged initially to a rehabilitation facility. She achieved a full recovery, and only partial left-sided hearing loss remained as a residual deficit.

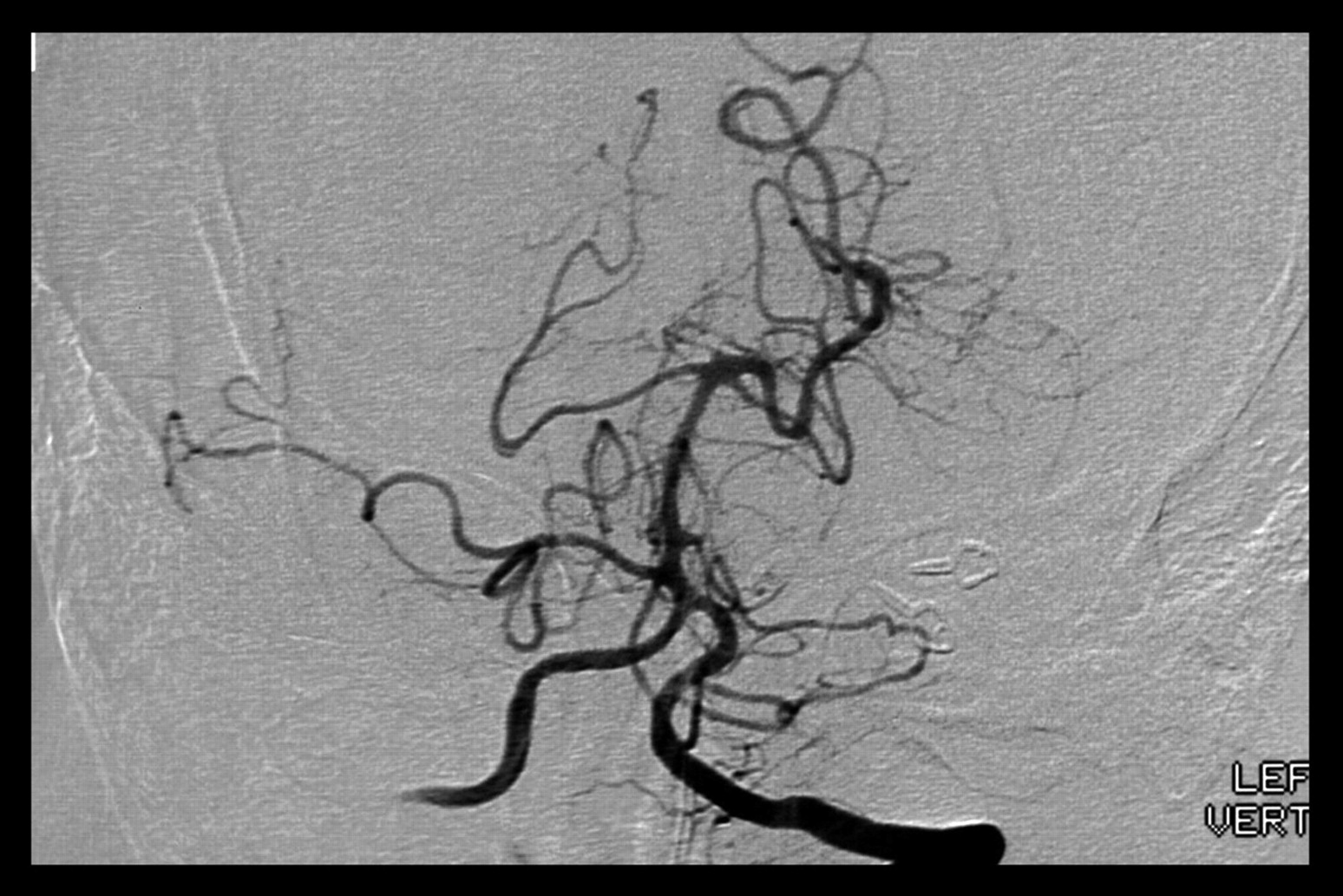
Frontal projection digital subtraction angiogram, left vertebral artery injection, shows no residual filling of the aneurysm after successful surgical trapping.
Discussion
True aneurysms of the anterior inferior cerebellar artery are rare. A total of 58 cases have been reported in the literature to date, and these account for 0.1% to 0.5% of all intracranial aneurysms (1–3). Of these, most involve the distal anterior inferior cerebellar artery, often near the cerebellopontine angle. The clinical presentations of anterior inferior cerebellar artery aneurysms are variable, with either symptoms of subarachnoid hemorrhage, including headache, or symptoms related to mass effect, especially when located at the cerebellopontine angle (4), where these lesions can present with symptoms of involvement of the adjacent VIIth and VIIIth cranial nerves, similar to the much more common vestibular schwannoma. Certainly, the much more common vestibular schwannoma would be in the differential of an intracanalicular mass lesion, as would the much rarer intracanalicular meningioma (5). Both of those lesions typically have an extracanalicular component at the cerebellopontine angle. It is interesting to note that anterior inferior cerebellar artery aneurysms have been mistaken for schwannomas in the past (6, 7). In this case, we had the benefit of angiography before CT angiography, which excluded tumor from the differential diagnoses.
Our patient experienced mild residual hearing loss, which was stable at follow-up visits. Spallone et al (4) found that patients with preoperative cranial nerve palsies achieved varied results. In their review of the literature, for patients who had undergone surgical clipping of the aneurysm, location of the lesion close to the internal meatus was a negative predictor for postoperative function. Of the six patients in their review who had undergone trapping of the aneurysm, three had preoperative deficits that persisted and three had new postoperative deficits. The possible explanations for persistent cranial nerve deficits include compromise of the internal auditory artery or direct surgical trauma.
Of the 58 aneurysms reviewed by Mizushima et al (1), only three were intracanalicular. Precise delineation of the relationship of the aneurysm with the bony landmarks of the internal auditory canal is critical in planning therapy for patients with symptomatic lesions. With 2D digital subtraction angiography, the bone is subtracted by using a standard mask technique. As such, the precise location of the internal auditory canal with respect to the aneurysm is difficult to assess. In this case, multi-detector CT angiography not only detected the aneurysm but also clearly showed its intracanalicular nature, which necessitated a retrosigmoid approach to the lesion.
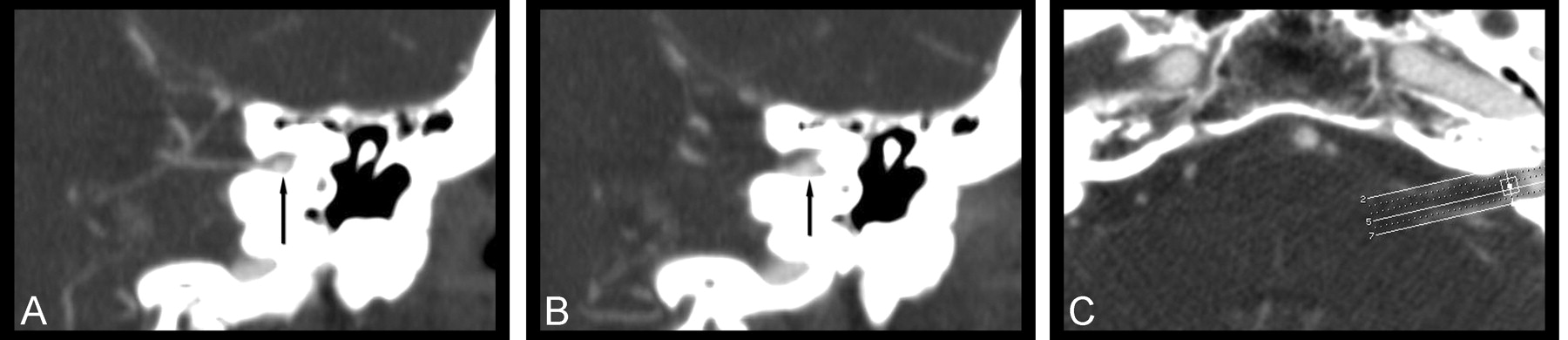
CT angiography has compared well with digital subtraction angiography for detecting cerebral aneurysms (8). Although earlier studies had cited locations near the skull base and other bony structures as potentially difficult areas (9), we think that the high spatial resolution of multi-detector CT angiography is well suited to these lesions. The anatomy of the internal auditory canal renders the use of some reconstruction and reformation techniques difficult. With maximal intensity projection images, the highest attenuation along any one voxel is used for the summated image. Any maximal intensity projection image with a slab thickness greater than the size of the internal auditory canal would include adjacent petrous bone in the volume. As such, the attenuation of the petrous bone is greater than the attenuation of the vessel and would obscure visualization. In addition, the orientation of the internal auditory canal is not in an orthogonal plane, which also makes using standardized maximal intensity projection images difficult. It is possible to generate targeted oblique maximal intensity projection images (Fig 4) that can reveal these lesions. The difficulty with relying on reformatted images again stresses the importance of reviewing source images with any CT angiographic data set.

Maximal intensity projection images.
A and B, Consecutive maximal intensity projection images from multi-detector CT angiography, obtained in an oblique coronal plane, show the anterior inferior cerebellar artery branch entering the internal meatus and the aneurysm (arrows).
C, Note that the plane necessary to produce these images is an oblique coronal plane (as shown) and that the slab thickness is thinner than the internal auditory canal.
Conclusion
Aneurysms of the anterior inferior cerebellar artery are rare and even more so within the internal auditory canal. Multi-detector CT angiography can detect these lesions and characterize their relationship to adjacent bony structures, which can be critical in treatment planning.
References
- Received November 21, 2002.
- Accepted after revision February 7, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.