
Abstract
Summary: Cases of sellar involvement of neurocysticercosis (NCC) are rare. Little is known about the mechanisms by which the parasite can compromise the pituitary gland. Although NCC damages sellar structures with direct compression by large cysts, extension through the basal cisterns and third ventricle with focal arachnoiditis can result as an inflammatory response. Evaluation for hypophyseal lesions in patients with NCC may allow for the diagnosis of unexplained loss of visual acuity and hormonal disturbances.
Reports of sellar neurocysticercosis (NCC) are rare (1–4). Little is known about the mechanisms by which the parasite can compromise the pituitary gland and the optic nerves (1, 2), although they probably do not differ from mechanisms previously described in the pathogenesis of NCC in other areas of the central nervous system (5–11). The goal of the present report is to describe seven cases of intrasellar NCC with different mechanisms of involvement as shown by conventional imaging studies.
Case Reports
In a series of 145 patients with NCC confirmed by imaging and enzyme-linked immunosorbent assay (ELISA) CSF findings, we found seven patients with hemianopsia and endocrinologic disturbances, five of whom presented with hydrocephalus as the initial manifestation. CT, MR imaging, and ELISA tests for NCC in CSF were performed for all patients. After placement of a ventriculo-peritoneal shunt in the patients with hydrocephalus, visual loss continued, and the imaging and laboratory studies focused on the sellar region, with important findings in relation to the diagnosis of NCC.
Although the course of disease was different among patients, the clinical picture was essentially similar in all. Neurologic symptoms started 4.5 months before hospital admission, with headache and progressive diminution of visual acuity as the most important features. At diagnosis, five patients (71%) had severe visual impairment (hemianoptic pattern), and all had clinical or subclinical manifestations of hormone disturbances.
The typical clinical course, diagnosis, and treatment were seen in case 1, but a more aggressive progression manifested in case 2.
Case 1
A 25-year-old female patient had a 4-month history of intracranial hypertension, hemianopsia, and endocrine disturbances (amenorrhea, dry skin, and weight gain). Initial CT showed severe acute hydrocephalus and a cyst in the sella. A shunt was used to treat her intracranial hypertension.
After shunt surgery, the visual and endocrine symptoms continued. A hormonal test confirmed hypothyroidism.
Subsequent CT focusing on the sellar region showed a large cystic lesion with erosion of the sella turcica and the sphenoidal sinus (Fig 1A). In the sagittal reconstruction, thinning and deformity of the posterior wall of the sphenoidal sinus was present, secondary to compression of the sellar structures (Fig 1B).

Intrasellar NCC in a patient with chiasmatic syndrome and hypothyroidism.
A, Axial CT image shows a left hypoattenuated lesion of the sellar region displacing the pituitary
B, Reformatted sagittal CT image shows expansion of the sellar floor into the sphenoidal sinus by the cystic lesion.
C, Sagittal postcontrast T1-weighted image reveals a hypointense extraaxial cystic lesion that displaces the hypophysis laterally, with extrasellar extension and dorsal displacement of the third ventricle and optic chiasm.
T1-weighted MR imaging in the axial plane showed a hypointense lesion that completely occupied the sellar region, surrounded by heterogeneous lesions affecting the walls of the sella turcica. Extreme thinning of the wall limiting the sphenoid sinus, secondary to the compression of the sellar structures, was present (Fig 1C).
Sagittal MR imaging revealed an extraaxial cystic lesion with displacement of the hypophysis lateral and dorsal to the third ventricle and optic chiasm; extreme thinning of the wall of the sphenoid sinus was evident (Fig 1C). Extraction of several vesicles typical of cysticercosis was easily performed by use of the transsphenoidal approach.
After surgery, the patient’s visual acuity improved and hormonal disturbances were corrected; no ongoing therapy was necessary.
Case 2
A 56-year-old male patient had a 4-month history of intracranial hypertension, severe vision loss, hypothyroidism, and hypocortisolism. Initial CT showed hydrocephalus without any other findings. After shunt surgery, the symptoms persisted, and visual deterioration (amaurosis) progressed.
MR imaging showed peripheral enhancement of the pineal region (Fig 2A), and parasellar structures included other basal cisterns, suggestive of focal arachnoiditis with compromise of the optic chiasm and pituitary stalk. An ELISA test of CSF was positive for NCC. Treatment with steroids and albendazole was unsuccessful, and the patient had definitive bilateral blindness and required permanent hormone replacement therapy.

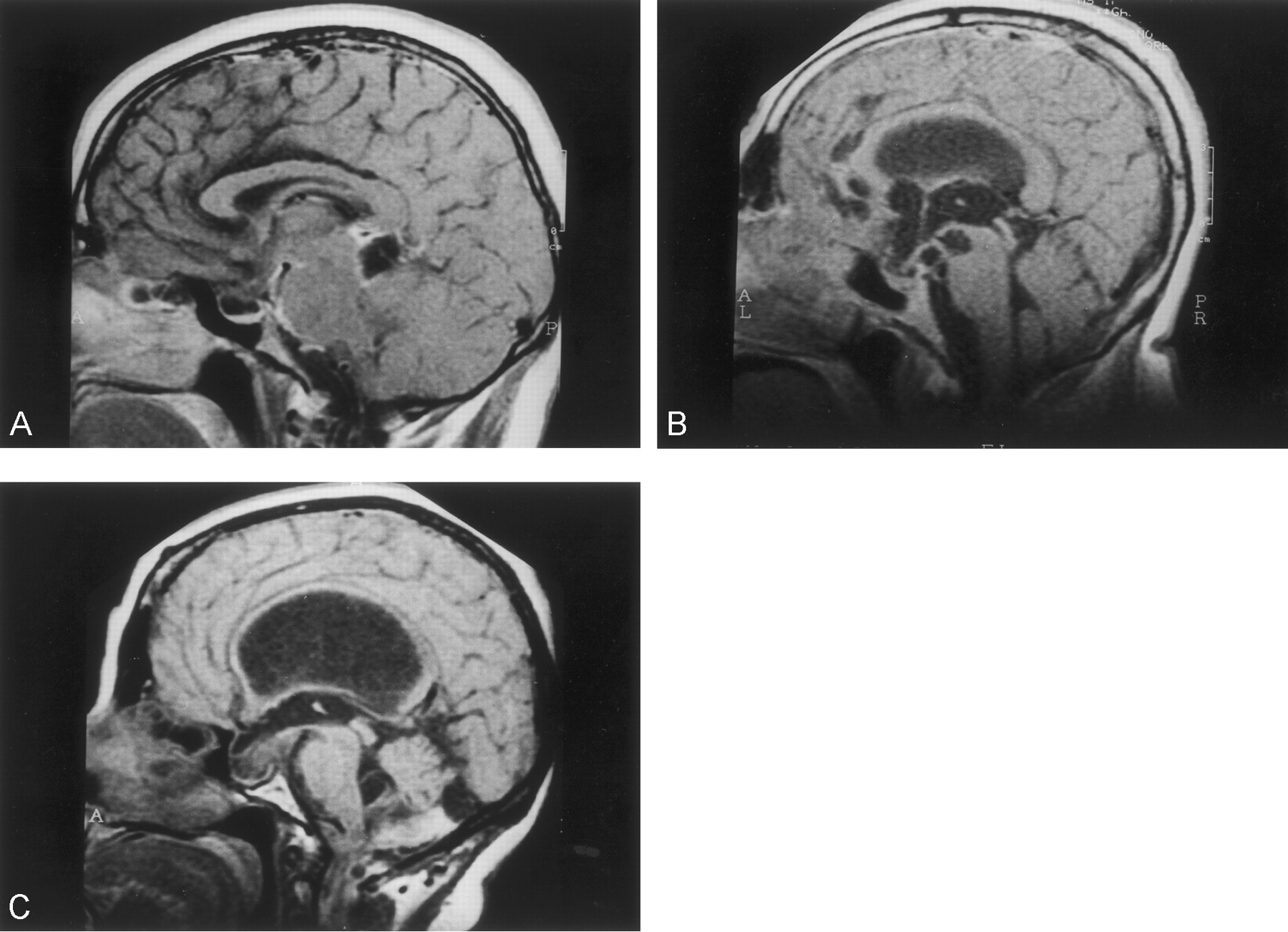
MR findings of NCC in other forms of sellar involvement.
A, Patient with a diagnosis of hydrocephalus, amaurosis, and severe hypothyroidism. Sagittal T1-weighted postcontrast MR image shows leptomeningeal enhancement of the parasellar region, the pineal gland, and prepontine cisterns.
B, Patient with a diagnosis of racemic NCC and symptoms of sellar involvement. Sagittal MR image shows a racemic, extraaxial lesion that displaces the parasellar structures with dorsal compression of the third ventricle, mesencephalic displacement, and hypophyseal compression.
C, Patient with a diagnosis of hydrocephalus, chiasmatic syndrome, and subclinical endocrine dysfunction. Sagittal T1-weighted MR image reveals a ventrally displaced infundibular stem and deformity of the fourth ventricle. ELISA findings for NCC in CSF were positive. Diagnosis was established by means of endoscopic extraction of multiple vesicles from the lateral and third ventricles.
After shunt placement in five (71%) patients, four were successfully treated with albendazole and steroids, and symptoms improved; all had intrasellar or subarachnoid lesions. The patient with severe arachnoiditis became bilaterally blind, and the other two patients with intrasellar or intraventricular cysts needed surgery (trans-sphenoidal or endoscopic approaches) to extract NCC vesicles.
Discussion
The sellar region and the basal cisterns contain many vascular and CNS structures that are separated by only a few millimeters, increasing the possibility that different pathologic entities can affect them simultaneously. Analysis of imaging findings and knowledge of the varied clinical presentations of NCC are important to detect cases of sellar involvement in patients with unexplained visual loss or atypical cystic lesions in the sella, especially in endemic countries. As in other sites of the CNS, the parasite can affect the sellar structures through diverse mechanisms, ranging from direct or indirect invasion to a severe local inflammatory response (5–11).
Mechanisms of Sellar Compromise
Direct sellar invasion.—
Direct invasion of the sella turcica by the NCC vesicle affecting the hypophysis is the most commonly described form in the literature (1–4) and is often confused with the most common tumors of the area (eg, cystic adenoma and craniopharyngioma). The absence of clinical suspicion of intrasellar NCC usually results in surgical treatment of the lesions and postoperative diagnosis of NCC with variable clinical results. In most cases (1–4), NCC cysts are located in the sellar region with displacement and eventual destruction of the hypophysis. Clinical manifestations are the same as for sellar neoplasias, basically bitemporal hemianopsia and endocrine disturbances. Patients can also develop hydrocephalus, which is a clinical clue that supports the diagnosis of NCC, because small focal lesions of the sellar region may be associated with arachnoiditis and only very large tumors usually cause CSF circulation disturbances.
The lesion can be misdiagnosed on the basis of axial CT findings (Fig 1A and B) as a hypophyseal adenoma with cystic degeneration, craniopharyngioma, arachnoid cyst, or a partially calcified giant carotid aneurysm. MR imaging is often more revealing, especially with sagittal views that allow for complete visualization of sellar and parasellar structures (Fig 1C).
Treatment usually consists of surgical excision of the well-localized lesion, generally through a transsphenoidal approach, especially in the case of large cysts or severe visual impairment (4). Serial measurements of hormone levels are important for the early diagnosis and follow-up of residual endocrine disturbances.
Intrasellar arachnoiditis.—
Arachnoiditis is one of the most severe complications of NCC, associated with hydrocephalus, multiple cranial nerve dysfunction, vasculitis, and death (5, 8, 11). Imaging studies show involvement of the leptomeninges (Fig 2A), which must be differentiated from other causes of chronic meningitis such as tuberculosis, sarcoidosis, and cryptococcosis (5).
Clinical symptoms of hydrocephalus are the most common presentation (5, 6); accordingly, therapy is directed at correcting intracranial hypertension with ventricular CSF shunt surgery. Generalized or focal inflammatory responses elicited by the parasite must be treated with high-dose steroids, cysticides, and, occasionally, cyclophosphamide (5).
The presence of focal arachnoiditis affecting the sella and surrounding cisterns has not been described as a clinical entity, but visual impairment in a patient with NCC who has been treated successfully with shunt surgery is a strongly suggestive feature of sellar involvement with NCC, and the patient should be treated with steroids and hormone replacement. Similar to other forms of arachnoiditis in NCC, the prognosis is poor (5, 6).
Subarachnoid involvement.—
It is estimated that 3.5% of the patients with NCC present with parasites in vesicles of the subarachnoid space (5, 9). This is probably an underestimate because of the absence of precise imaging studies and the inability to search specifically for these lesions in patients with relatively few symptoms (8).
Anatomic characteristics of the basal cisterns and the relationship between them facilitate expansion of racemous lesions. Contiguity of several cysts can be detected by use of imaging studies because of the growth of the lesions through the thin walls of the cisterns (Fig 2B). Extension of a large lesion by this mechanism can give rise to visual and hormonal impairment secondary to direct compression of the hypophyseal stem and the optic nerves.
Treatment is determined by the clinical condition of the patient. Small lesions respond well to medical treatment, whereas surgery is necessary for large cysts and severe intracranial hydrocephalus.
Intraventricular extension of NCC.—
Intraventricular cysticercosis is the second most common form of NCC (5). The presence of cystic lesions within the third ventricle can be confused with a colloid cyst (especially when localized in the anterior portion of the ventricle), or subependymal and choroid cysts (5, 9). The most common clinical presentation is hydrocephalus caused by occlusion of the foramina of Monroe or fourth ventricle, with a few reported cases of sudden death due to acute obstruction (5)
In some cases, intraventricular extension of NCC can simulate other causes of hydrocephalus because of dilatation of the third ventricle, but patients commonly present with a typical chiasmatic syndrome. Diagnosis can be established on the basis of MR imaging and endoscopic findings, but extraction of multiple vesicles from the lateral and third ventricles, which are not visible on MR images, is common in intraventricular NCC (12). Diagnosis in one of our patients with visual impairment, who did not have an obvious lesion on MR images, was made after endoscopic extraction of cysts inside the lateral and third ventricle. The diagnosis was suspected because deformation of the content of the sella through the roof of the third ventricle existed (Fig 2C).
Conclusion
Preoperative diagnosis of intrasellar NCC may be difficult when present as the only feature, but the association of hydrocephalus and other lesions revealed by CT and MR imaging may be helpful. The neurosurgeon and neuroradiologist should be aware of intraventricular and subarachnoid cysts that can be missed on conventional imaging studies. The development of newer imaging techniques, including the use of special contrast media, may improve the preoperative diagnosis and result in more targeted medical or surgical treatments. Neuroradiologic studies and a search for antibodies against NCC in CSF as well as hormonal abnormalities should be performed for every patient with NCC who presents with visual loss. Careful analysis of the clinical data can reveal previously unnoticed lesions that may result in early treatment and prevention of future complications.
References
- Received November 14, 2001.
- Accepted after revision February 13, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.